
Abstract
Levorphanol (levo-3-hydroxy-
Keywords
Introduction
Pain is a frequent and disabling symptom experienced by patients with cancer. Treatment of cancer-related pain relies on recommendations by the World Health Organization (WHO), which recommends a stepladder approach, based on pain intensity. 1 Step 1 drugs such as aspirin and or nonsteroidal anti-inflammatory agents treat mild pain. 2 Step 2 drugs such as hydrocodone and oxycodone bound to acetaminophen, or tramadol, treat mild to moderate pain. 3 Step 3 including hydromorphone, oxycodone, oxymorphone, fentanyl, methadone, morphine, and Levorphanol treat moderate to severe pain. 4 Originally developed as an alternative to morphine, Levorphanol remains underutilized. 5 Levorphanol has many similarities to methadone. Palliative care specialists consider Levorphanol for patients when methadone does not control pain or when patients experience adverse effects from methadone. 6 The review examines the pharmacokinetics, pharmacodynamics, and clinical uses of Levorphanol. It also discusses potential uses of Levorphanol.
Structure of Levorphanol
Levorphanol has a phenanthrene structure, much like morphine (Fig. 1). It differs from morphine in lacking an oxygen group and 6-hydroxyl group. The molecular weight of Levorphanol is 443.5 Da.
7
Structure of Levorphanol.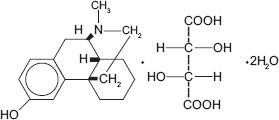
Opioid Receptor Interactions
Levorphanol has a strong affinity for μ, δ, and κ opioid receptors. Ki values (nM) for Levorphanol are 0.21 ± 0.02 at the μ-opioid receptor, and 4.2 ± 0.6 at the δ-opioid receptor. Levorphanol is a full κ agonist, 8 with affinities of 2.3 ± 0.3. These affinity values confirm the strong affinity to the traditional opioid receptors.
NMDA Receptor Interaction
Levorphanol blocks the
Other Receptors
Levorphanol has anticholinergic effects, 10 like other opioids, and similar to methadone, blocks the uptake of serotonin and norepinephrine, making it potentially useful for neuropathic pain. 11
Formulation
Levorphanol is available as an oral tablet (scored), and capsule. Parenteral formulations are not available in the United States.
Compatibility
Parenteral Levorphanol is compatible with anticholinergic agents like atropine, scopolamine, and glycopyrrolate. 12 Parenteral Levorphanol is incompatible with intravenous (IV) pentobarbital, phenobarbital, and phenytoin. It is incompatible with secobarbital, sodium bicarbonate, and thiopental. 12 It is compatible with propofol. 12
Pharmacology/Route of Administration
Levorphanol is effective for pain control when administered by multiple routes including oral, IV, subcutaneous, and intramuscular routes.
Oral Administration
When administered orally, peak analgesia occurs about 1 h after administration. Bioavailability is greater than morphine as suggested by the oral to IV conversion ration of 2:1. Levorphanol has a half-life of up to 30 h. 13 Plasma protein binding is about 40 ± 2.6%. 13 Levorphanol enters the cerebrospinal fluid at 60–70% of corresponding plasma levels. 13 The duration of analgesic effect is between 6–15 h.
Intravenous Administration
When given intravenously, analgesia occurs within 20 min. Levorphanol distributes into tissue after IV administration. It afterwards leaves tissues to be metabolized. Levorphanol has a steady-state volume of distribution of 10–13 L/kg. 13 The duration of analgesia ranges from 6 to 15 h. The reasons for variability of duration of action of analgesia are unknown and may be related to protein binding or large volume of distribution. After IV administration, plasma concentrations decline exponentially with a half-life of about 11–16 h and a clearance of 0.78–1.1 L/kg/h. 13
Subcutaneous Administration
There is no detailed pharmacological information about Levorphanol given by the subcutaneous route. The subcutaneous route is interchangeable with the IV route. Duration of analgesic effect when given by the subcutaneous route is 4–15 h. 12
Intramuscular Administration
When given intramuscularly, absorption is rapid with onset of effects within 15–30 min of administration. 12
Sublingual Administration
Levorphanol has poor absorption by the sublingual route compared with other opioids. 14
Intranasal Administration
There is no detailed pharmacological information about Levorphanol administered via the intranasal route.
Biotransformation
Glucuronidation metabolizes Levorphanol with uridine diphosphate glucuronosyltransferase (UGT) isoenzyme 2B7 converting Levorphanol to Levorphanol-3-glucuronide, an active metabolite. Little unchanged drug exists in the bile, urine, or feces. Cytochrome oxidase enzymes play no role in the drug metabolism of Levorphanol. Levorphanol experiences significant first-pass metabolism to produce its metabolite. 15
Elimination
Kidney disease
Since the kidney excretes the metabolite Levorphanol-3-glucuronide, using Levorphanol in renal disease may lead to accumulation of active metabolites. 5
Levorphanol binds tightly to protein giving it a high volume of distribution. This makes it unlikely to be affected by dialysis.
Liver disease
The liver metabolizes Levorphanol. There is no information on Levorphanol's extraction and clearance in the liver. When using Levorphanol in acute hepatic insufficiency, consider increasing dose intervals. 5
Drug Interactions
Levorphanol does not interact with the CYP450 system. Since glucuronidation is the main route of metabolism, drugs interfering with glucuronidation may influence the clinical effects of Levorphanol. Drugs inhibiting glucuronidation such as tricyclic antidepressants, phenothiazines, and ranitidine potentially increase the effects of Levorphanol. Drugs inducing glucuronidation, such as carbamazepine, phenobarbital, phenytoin, and rifampin potentially decrease the effect of Levorphanol. Using central nervous system depressants with Levorphanol results in additive central nervous effects. Monoamine oxidase (MAO) inhibitors and Levorphanol cause hypertensive crises if given together. 5
Adverse Effects
Levorphanol has adverse effects similar to other step 3 opioids such as nausea, vomiting, sedation, and constipation. Adverse effects increase with dose. Levorphanol releases histamine and causes pruritis. Levorphanol has caused urinary retention. 7 Dizziness occurs 10% of the time. Levorphanol increases bile duct pressure and should be avoided in biliary surgery. 7 A clinical trial evaluating Levorphanol in neuropathic pain showed that patients experienced increased anger, irritability, mood, and/or personality changes with higher doses. 16 This suggests that either the parent drug or the metabolite may be active. 5 There are no reports of QTc prolongation with Levorphanol.
Clinical Studies
One prospective study and one retrospective review of Levorphanol use is available.6,16 The prospective study examined using Levorphanol in several types of neuropathic pain, which included focal nerve injury, post herpetic neuralgia, and spinal cord injury with incomplete myelopathy, central pain after stroke or focal brain lesion, and multiple sclerosis. Patients in the study were taking doses of codeine exceeding 360 mg of codeine per day (40–60 mg morphine equivalent). They also took non-opioid analgesics such as antidepressants (in 24 patients), non-steroidal antiinflammatory drugs (in 24 patients), and anticonvulsants (in 11 patients). Patients received either high-strength (0.75 mg) (16 mg max) or low-strength (0.15 mg) (3 mg max) capsules of Levorphanol for 8 weeks under double-blind conditions. Patients self-titrated the Levorphanol to a maximum of 21 capsules of either strength per day. Dosing schedule was three times daily. Outcome measures included pain intensity, quality of life, effects on psychological and cognitive function, number of doses taken daily, and blood Levorphanol levels. Among the 81 patients evaluated, high-strength Levorphanol capsules reduced pain by 36% compared with a 21% reduction in pain in the low-strength group (
Levorphanol for Refractory Pain
McNulty and co-workers 17 evaluated the use of Levorphanol for cases of refractory pain including a small population of patients with previous methadone use. The authors’ patient population consisted of patients with non-malignant chronic pain and hospice patients with predominantly cancer. Of the patients who were using methadone and switched to Levorphanol because of poor pain control (N = 20), 8 (40%) reported excellent relief and 7 (35%) reported fair relief. In cancer patients enrolled in hospice and treated with Levorphanol, 6 of 11 (55%) patients reported excellent relief and 2 of 11 (18%) reported fair relief. Patients tolerated Levorphanol well.
Opioid Conversions
Equianalgesic dosing
Single dose studies show that Levorphanol is 4–8 times as potent as morphine. 7 Two milligrams of intramuscular Levorphanol tartrate depresses respiration to the same degree as 10–15 mg of intramuscular morphine. 7
Route conversions for Levorphanol
When converting from oral Levorphanol to subcutaneous Levorphanol, a 2:1 ratio is used. 7 When converting from the IV to subcutaneous route, 1 mg of Levorphanol IV is equal to 1 mg subcutaneously. 7
Conversions between morphine and Levorphanol

Rotations Involving Methadone and Levorphanol
The conversion ratio when switching from methadone to Levorphanol is 2:1. 7
Schedule of Administration
Dosing
Oral
Opioid naïve patients start with 6 mg a day orally, divided into three doses.
Intravenous
The recommended starting dose for IV administration is 1 mg given by slow injection or continuous infusion.7,18 This is given every 6–8 h.
Subcutaneous
The starting dose for subcutaneous administration is 1–2 mg and repeated every 6–8 h as needed as the subcutaneous route of administration is felt to be interchangeable with the IV route.
Breakthrough Analgesia
Managing breakthrough pain involves using rapid onset opioids matching the rapid onset of breakthrough pain. 19 Short acting opioids are used with Levorphanol for breakthrough pain. Unlike methadone, Levorphanol is not lipophilic and is not recommended as a breakthrough analgesic. It has the risk of accumulation with repeated short interval dosing.
Pharmacoeconomics
Levorphanol cost.

Conclusion
Levorphanol, belonging to the morphinan series of opioids has greater potency than morphine. It is a NMDA receptor like methadone. Levorphanol has a long half-life, which can lead to accumulation with repeated doses. Levorphanol differs from methadone in being excreted through the kidneys, limiting its use in renal failure. Preliminary evidence shows Levorphanol improving opioid responsiveness in cases where methadone loses effectiveness. Patients with neuropathic pain benefit from Levorphanol. Its true place in cancer analgesic therapy remains to be characterized because of limited clinical trial data available. Possible reasons for the drug being underutilized may be the same reasons that methadone had been underutilized: physician reluctance to use a drug due to unfamiliarity or even concerns about its long half-life and risk of accumulation.
Author Contributions
Conceived the concept: EP. Wrote the first draft of the manuscript: EP. Made critical revisions: EP. The author reviewed and approved of the final manuscript.
Disclosures and Ethics
As a requirement of publication the author has provided signed confirmation of compliance with ethical and legal obligations including but not limited to compliance with ICMJE authorship and competing interests guidelines, that the article is neither under consideration for publication nor published elsewhere, of their compliance with legal and ethical guidelines concerning human and animal research participants (if applicable), and that permission has been obtained for reproduction of any copyrighted material. This article was subject to blind, independent, expert peer review. The reviewers reported no competing interests.