
Abstract
The authors describe a case of a critically ill patient presenting after motor vehicle trauma complicated by anterior myocardial infarction and cardiogenic shock. Assessment of myocardial viability in the territory of a critically stenosed left anterior descending artery (LAD) was necessary to determine the optimal management strategy. Bedside dobutamine stress echocardiography (DSE) demonstrated viability in the LAD territory and the patient underwent uncomplicated single-vessel bypass surgery with subsequent improvement in left-ventricular function. This case illustrates the utility of bedside DSE to assess myocardial viability in patients for whom other non-invasive modalities are not feasible.
Case Report
A 61 year old man with a remote history of coronary disease presented after a motor vehicle collision that was complicated by multiple orthopedic injuries. Three days after initial stabilization which included blood transfusion, brief mechanical ventilation, and open reduction and internal fixation of a right femur fracture, the patient experienced intermittent chest burning similar to his index angina culminating in a prolonged episode of chest discomfort. This event was associated with loss of anterior forces on the electrocardiogram (Fig. 1A–C) and elevated biomarkers (peak troponin I of of 9.4 ng/mL). Cardiac catheterization showed a tortuous and calcified LAD with a critical mid-segment stenosis not amenable to PCI (Video 1). Further, because the patient required additional surgery on his left femur in the near-term, PCI was not felt to be an optimal revascularization strategy given the requirement for dual anti-platelet therapy, which would increase the risk of operative bleeding. One day after this event, the patient required re-intubation for respiratory failure and invasive hemodynamics revealed an LVEDP of 40 mmHg and mixed venous saturation of 60% suggesting cardiogenic shock. A transthoracic echocardiogram showed impaired LV systolic function and akinesis of the mid-distal LAD territory (Video 2A–D). Before the patient was subjected to the risk of surgical revascularization, a viability study was recommended to assess the potential benefit of bypassing the LAD. Given the limited options for determination of viability (ie, the patient was not stable enough to undergo cardiac MRI, cardiac PET, or thallium-SPECT), a bedside dobutamine stress echocardiogram (DSE) was performed. This study demonstrated improvement of contractility of the anterior and anteroseptal walls with increasing doses of dobutamine suggesting viability of the LAD territory (Video 3A–I). Single vessel bypass surgery (LIMA-LAD) was performed with no immediate complications. Five days after CABG, he underwent uncomplicated fixation of his left femur. A follow-up echocardiogram 4 months post-operatively showed normal LV wall motion and left ventricular ejection fraction >75% suggesting that revascularization of the LAD contributed to improvement in LV function (Video 4A–C).
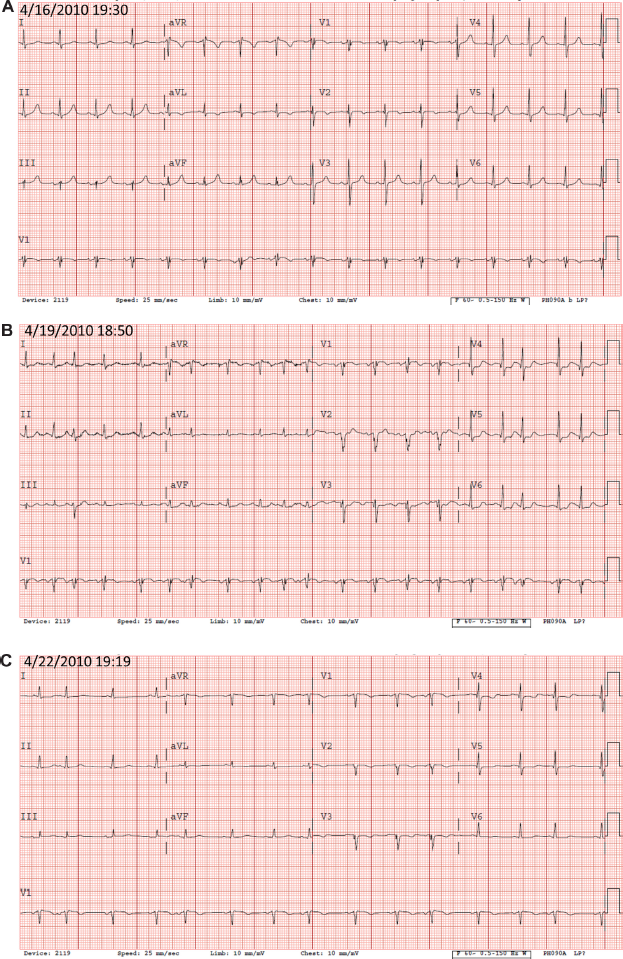
Patient Electrocardiograms (ECG). (
Discussion
Recently published Appropriateness Use Criteria for Echocardiography indicated an appropriateness score of 8 (out of 9) for the assessment of myocardial viability in patients with moderate to severe left ventricular dysfunction who are eligible for revascularization. 1 DSE has become an important modality for the assessment of myocardial viability with a sensitivity and specificity of 71%–97% and 63%–95%, respectively, compared to Positron Emission Tomography (PET), considered the gold standard. 2 Viability is determined by the presence of contractile reserve with escalating doses of dobutamine starting at 2.5 μg/kg/min and reaching 20–40 μg/kg/min. Atropine supplementation may be given if target heart rate is not met at the peak dobutamine dose. Four patterns of dysfunctional contractile response have been described; these include no change in function, worsening of function, sustained improvement in contractility, and initial improvement in function then subsequent decline with increasing doses. This latter pattern, called a biphasic response, is consistent with ischemia and is the most specific for viable myocardium.3,4 Transmural myocardial strain has been described as a bedside technique to assess myocardial viability in the setting of acute inferior myocardial infarction (MI) with sensitivity and specificity of 100% and 96%, respectively, when referenced to cardiac magnetic resonance imaging (CMR). 5 This method would not have been optimal for our patient due to (1) the need for off-line data analysis; and (2) unknown applicability in anterior MI.
When performed with appropriate personnel and monitoring equipment, DSE is a safe procedure with rare major complications. A meta-analysis of >55,000 patients reported the rate of life-threatening complications (cardiac rupture, acute MI, cerebrovascular accident, asystole, ventricular fibrillation, and sustained ventricular tachycardia) to be 1 per 475 studies. 6 Similar complications in patients undergoing exercise or dipyridamole stress testing range from 1 per 1100–1600. 6 An increased complication rate during DSE likely reflects a higher burden of co-morbid conditions which precludes exercise.
In critically ill patients who may be hemodynamically tenuous and on mechanical ventilation, options for viability assessment are limited. Commonly used modalities such as thallium-SPECT, CMR, and cardiac PET are impractical in this population due to, among other reasons, medical device ferromagnetism, safety of patient transportation, and the requirement to lie flat and motionless for optimal image quality. In this patient population, bedside DSE holds a unique advantage in the assessment of myocardial viability and should be considered when knowledge of viability will impact management decisions.
Footnotes
Acknowledgments
with the text The authors would like to acknowledge Erik Funk, MD who assisted with acquisition of the follow-up echocardiogram and update of the patient's status.