
Abstract
Severe but silent coronary artery disease may rarely exist in young patients with a low-risk profile but with a family history of coronary artery disease. We describe the case of a 33-year-old Caucasian male with progressive shortness of breath caused by a huge left atrial myxoma who was diagnosed to have significant coronary artery disease in the preoperative assessment. After investigations, the patient underwent resection of the left atrial tumor and coronary artery bypass grafting (CABG) with a successful outcome. Even in the case of a young male, it may be prudent to investigate silent coronary artery disease in the presence of cardiovascular risk factors and family history of coronary artery disease. The learning objective of this case is to debate about the usefulness of a preoperative coronary study even in the young population with cardiac nonischemic pathologies (ie, valve pathology, cardiac tumors, etc.).
Keywords
Introduction
Coronary artery disease may coexist with the presence of other cardiac pathologies such as valvular diseases and cardiac tumors.
Nevertheless, the main symptom could be related to only the presence of the left atrial mass. In the presence of low-risk profile for coronary artery disease, a cardiac computed tomography (CT) scan could be an attractive primary investigation tool in young population to detect silent but severe coronary pathology.1,2
Case Report
A 33-year-old Caucasian male with a family history of coronary artery disease (his father suffered from acute myocardial infarction and was treated by thrombolysis and medical therapy) presented to our hospital for sudden severe resting dyspnea, hemodynamic instability, and supraventricular tachycardia. He had a history of smoking and mild hypertension.
Physical examination was unremarkable. The transthoracic echocardiography revealed a huge (4 x 5 cm) left atrial mass attached to the atrial septum. The appearance was suggestive of atrial myxoma. The patient was immediately admitted to the intensive cardiac care unit and surgical excision of the mass was planned. As the patient was considered to have a low risk for the presence of coronary artery disease, he underwent a 64-slice cardiac CT scan rather than coronary angiography as preoperative coronary evaluation. The CT scan well visualized the huge left atrial mass (Fig. 1).
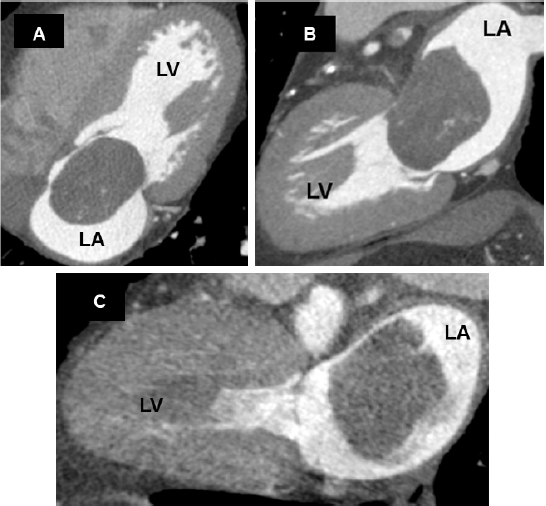
Multiplanar reconstruction of the left cardiac chambers. Left atrial myxoma prolapsing into the mitral valve orifice, going into the left ventricle during the diastolic phase of heart cycle (
The scan also showed a significant proximal lesion of the left anterior descending (LAD) artery and a moderate lesion of a nondominant left circumflex artery, with narrow peripheral vessels; the right coronary artery was normal (Fig. 2).
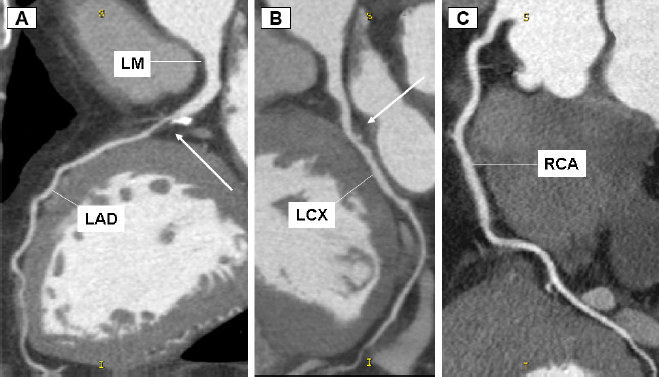
Multiplanar reconstruction of the coronary tree. (
The patient underwent successful operation of resection of left atrial mass associated with coronary artery bypass grafting (CABG) on LAD, using the left internal thoracic artery (LITA). Histological analysis of the tumor confirmed the preoperative diagnosis of left atrial myxoma. The postoperative course was uneventful, and the patient was shortly discharged home. The patient has given consent for publication of this report.
Discussion
The association between silent coronary artery disease and other surgical cardiac conditions is well established.
This case aims to underline that unsuspected silent severe coronary artery disease and conditions such as a left atrial myxoma may coexist, even in the setting of a young population.
There is still no consensus whether preoperative coronary angiography should be always performed or made in the presence of ischemic symptoms or never for the fear of potential risk of sudden death.3,4
In our opinion, young patients with known cardiac myxoma with a family history of coronary disease and in the presence of cardiovascular risk factors may benefit from a preoperative coronary screening as a routine workup in order to rule out any concomitant coronary artery disease before surgery.
Cardiac CT imaging could be a helpful diagnostic tool in detecting unsuspected coronary lesions, providing additional relevant diagnostic information to the surgeon and eventually addressing the patient for a more invasive cardiac catheterization. 5
In this case, the preoperative coronary investigation led us to change the planning of the surgery.
Although the case presented is not sufficient to broadly extend the indications to other cases, we suggest that investigation of the coronary artery tree is remarkable in all instances before performing cardiac surgery even in the case of young population.
Hence, we hope that further randomized clinical trials will be able to fix guidelines of noninvasive coronary investigation in a cohort of low-risk young patients.
Author Contributions
Conceived and designed the experiments: MG, MA. Analyzed the data: MG, MR. Wrote the first draft of the manuscript: MG. Contributed to the writing of the manuscript: MA, GP. Agree with manuscript results and conclusions: DA, MR. Jointly developed the structure and arguments for the paper: MA. Made critical revisions and approved final version: MA. All authors reviewed and approved of the final manuscript.