
Abstract
We experienced a successful surgical Williams's syndrome case of extended aortoplasty by means of Doty's method (two sinus reconstructions) for congenital supravalvular aortic stenosis. Case was 29-year-old woman, who had no complaint except heart murmur and dyspnea. The retrograde aortography and Digital Subtraction Angiography (DSA) demonstrated localized stenosis just above the aortic valve, and it was an hour-glass type. This case showed excellent results. Doty's aortoplasty was favorable method for supravalvular aortic stenosis without deformity of aortic valve and coronary obstruction.
Introduction
Williams syndrome is a rare genetic condition (estimated to occur in 1/7,500 births) which causes medical, intellectual and developmental problems.1–3
Williams's syndrome was first recognized as a distinct entity in 1961. It is present at birth, and affects males and females equally1,2
The syndrome is characterized by varying degrees of left ventricular outflow tract obstruction beginning superior to the aortic valve, hypercalcemia, elfin faces, and mental retardation. Logan described patients who had a familial form of supravalvular aortic stenosis with normal face and normal mental development, which may delay diagnosis.2–5
It can occur in all ethnic groups and has been identified in countries throughout the world. Supravalvular aortic stenosis is a familial autosomal dominant disorder with variable expression and affects both sexes equally. The vascular pathology of familial supravalvular aortic stenosis and Williams's syndrome results from mutations involving the elastin gene on chromosome 7q11.23.2–6
Case Report
A 29-year-old woman was referred to our clinic because of a cardiac murmur and dyspnea. She had moderate mental retardation (with WISC-R test). Aortography, coronary angiography, echocardiography and Digital Subtraction Angiography (DSA) were performed before the operation, and all demonstrated a typical hour-glass type stenosis just above the aortic valve (Fig. 1). The preoperative peak systolic pressure gradient between the left ventricle and ascending aorta was 70 mmHg. There was no coronary stenosis or other cardiac anomalies.

Digital Subtraction Angiography (DSA). Typical hour-glass type stenosis.
We performed successful surgical repair of extended aortoplasty using Doty's method (two sinus reconstructions) for congenital supravalvular aortic stenosis. After standard cardiopulmonary bypass, bi-sinusal inverted Y incision was made between noncoronary cusp and right coronary cusp; and the ridge was removed with sharp dissection above the left coronary sinus. Resulting defect on the aorta was then repaired with Dacron patch (Fig. 2). The systolic pressure gradient between the left ventricle and ascending aorta improved to normal (0–5 mmHg) postoperatively. The patient was extubated 7 hours following surgery, and was discharged at the 5th postoperative day. The patient was fine and had no complaints.
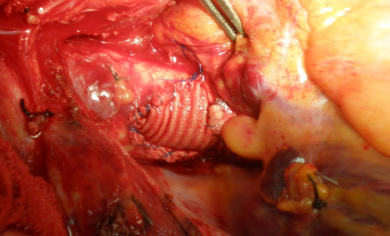
Doty technique (Y patch).
Discussion
Supravalvular aortic stenosis is an obstructive congenital deformity of the aorta which originates just distal to the origin of coronary arteries and produced either localized or diffuse narrowing of ascending aorta. 7
Historically supravalvular aortic stenosis was originally described by the Italian Mencarelli in 1930. In 1958 Denie and Verheug reported 13 pathological examples of this disorder. The designation Williams or Williams-Beuren syndrome have been applied to the distinctive picture produced by coexistence of cardiac and multiple system disorders.2–8
There are three specific anatomic types of supravalvular aortic stenosis: The membranous type (A), which consists of a simple fibrous diaphragm containing a single perforation. The hypoplastic type (B), which consists of a unifortn hypoplasia of the entire ascending aorta. The hourglass type (C), which characterized by extremc thickening of the medial layer of the ascending aorta.2,6,7
Cardiac anomalies in Williams's syndrome include supravalvular aortic stenosis, narrowing of peripheral systemic and pulmonary arteries. Occasionally, there is moderate thickening of the aortic cusps and valvular pulmonary stenosis. Children with supravalvular aortic stenosis appear to be subject to the same risks of unexpected death and infective endocarditis as those with valvular aortic stenosis. Studies of the natural history of supravalvular aortic stenosis indicate that the aortic lesion is progressive due to poor growth of ascending aorta.6–10
Treatment for supravalvular aortic stenosis is surgical intervention. Expansion of one sinus with patch can easily be performed for localized type stenosis. Using two sinus reconstructions technique, Doty has tried to remove supraaortic stenosis by means of patches placed in inverted Y shape (pant patch) on non-coronary and right coronary sinus Valsalvas.
In their study conducted with 8 patients operated with single sinus patch reconstruction method, Daglar et al observed a gradient with an average of 7.6 ± 7 mmHg (0–17 mmHg) in echocardiography tests conducted within late periods of the patients, although no residual gradient was detected during intra-operative measuring (We believe that it is more appropriate to conduct gradient measuring in postoperative period than intraoperatively). 6 Although this technique is preferred for positive results obtained in long periods, it is reported that in some series residual gradient between 15–30 mmHg was observed.6,9 During the examinations, it was considered that the main reason for the gradient involved was invasion of fibrotic intimal coat into left coronary leaflets upon expansion of non-coronary sinus with patch. However, such an occurrence was not observed for patients treated with two sinus reconstructions (Doty technique). Even though the procedure seems to be a little more complicated, by means of appropriate cut and expansion with patch applied on both right coronary cusp and non-coronary cusp, it is possible to provide complete protection against fibrotic intimal thickening, which is likely to develop in the future. For the phenomena involved, fibrotic tissue was quite firm, even calcific on particular areas due to the age of the patient. Because of the reasons we mentioned above, when the stenosis is very close to the valves and the coronary ostia, the use of the Doty technique may be preferred.
There are several variations of the surgical technique for correcting this type of defect. In a study concerning the efficacy of several techniques, Hazekamp et al, did not find any significant differences in change in valve function, and found the efficacy of reducing the pressure gradient was similar and acceptable in all techniques. In the cases of recurrent serious stenosis, an alternative is to use a valved conduit between the free wall of aortic root and the stenosis free aorta. Similarly, autologous arterial graft from the pulmonary artery, as described by Al-Halees et al, can be used as another option not only for cases of recurring stenosis but also for complex cases with diffuse stenosis.2,5–7
Conclusion
Supravalvular aortic stenosis is a complex and uncommon disease that requires careful preoperative evaluation and proper selection of surgical treatment method. We conclude that Doty's inverted Y patching method may be an effective choice for correction of the supravalvular aortic stenosis.
Disclosures
The authors report no conflicts of interest.