
Abstract
Introduction
It has been shown that in experienced hands repeated CABG is doable procedure. However the quality of life after third time CABG has not been evaluated so far.
Patients and Methods
The peri-operative data of 25 (22 male, mean age of 65.5 ± 8.0 years) consecutive patients in a single centre undergoing third time-CABG from 4/96 to 11/06 were studied. Quality of life (QoL) was assessed by Short Form (SF)-36 Questionnaire.
Results
30 day mortality was 12% (3/25). Seven died during follow-up. In 15 survivors median follow-up was 94 months (2–122 months). 1-, 5-, and 10-year survival were 77.8%, 65.0%, and 53.1%, respectively. Present NYHA status was significantly improved in comparison to preoperative values (2.4 ± 0.8 vs. 3.2 ± 0.56, p = 0.012). QoL was comparable with an age matched general population with heart insufficiency.
Conclusion
Third time CABG can be performed with acceptable peri-operative mortality. Significant improvement of NYHA status and acceptable quality of life results justifies our surgical approach in this challenging patient cohort.
Introduction
Coronary artery bypass grafting (CABG) for therapy of patients with symptomatic multi-vessel coronary artery disease is now an established procedure. It offers well documented relief of angina pectoris and prolongs the life of patients. However, coronary artery disease (CAD) is progressive and degenerative changes are known to occur in bypass conduits, especially Saphenous vein grafts. Thus, CABG is not a curative but a palliative therapy. It has been estimated that almost 7% of all patients undergoing CABG will have a repeat operation within 10 years following primary surgery. Consequently, the number of patients requiring a third–-time CABG (Re-redo CABG) has also increased.
It has been shown that in experienced hands repeated CABG is doable procedure.1–4 However the quality of life after third time CABG has not been evaluated so far.
We report our single center experience with 25 patients undergoing third time CABG with particular emphasis on quality of life after this procedure.
Quality of life can be measured by different methods. One measure is Short-Life 36(SF36).5–6 It has been found to be a useful method for assessing quality of life and measuring clinical outcome. This questionnaire is commonly used after CABG surgery to evaluate the quality of life of a patient.
Patients and Methods
From April 1996 to November 2006, 25 patients underwent Re-Re CABG at our institution. Patients receiving concomitant cardiac procedures were excluded from the study. There were 22 males and 3 females. The mean age was 65.5 ± 8 years. The peri-operative data of these patients were reviewed.
Pt. characteristics are given in Table 1.
Patient characteristics.
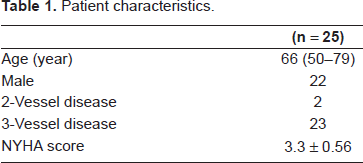
Their average age at the first operation was 51.4 ± 7.9 years, and their average age at the second operation was 56.9 ± 7.7 years. The average interval between the first and second operation was 60 ± 54.5 months and the interval between the second and third operation was 102.2 ± 47.7 months.
The indication for the third CABG was angina refractory to maximal medical management. Four of these patients (4/25) had high grade stenosis of the bypass conduits, fifteen pts. (15/25) had complete blockage of conduits and six (6/25) had a combination of progression of CAD and blockage of the conduits.
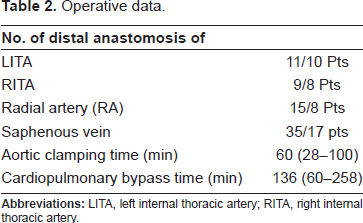
The peri-operative data are given in Table 2.
Operative data.
Pre-Operative management
All patients underwent standard pre-operative examinations e.g.: chest X-ray, electrocardiogram (ECG), routine blood tests, Doppler examination of extra-cranial vessels and pulmonary functional test. Coronary angiography (with special attention to the course of the LIMA graft in relation to the sternal wires) and echocardiography were done to evaluate the coronaries and cardiac valves as well as cardiac function. Computed tomography (CT) scans of the chest were performed to evaluate the distances of the brachio-cephalic vein, the aorta and the right ventricle from the sternum. Furthermore, gross evaluation or if necessary, a Doppler examination of the femoral vessels was performed in anticipation of possible groin cannulation.
Surgical technique
In the operation theatre, after the skin incision and removal of the previous sternal wires, the sternum was divided using the oscillating saw. Ventilation was discontinued immediately prior re-sternotomy. In addition, patients were placed in Trendelenburg position to decrease the right ventricular pre-load. Care was taken to avoid hypertension during sternotomy. The skin above one femoral artery was marked with a clamp for optional emergency cannulation.
After sternotomy, mediastinal structures as well as the right atrium and the ascending aorta were carefully dissected.
After systemic heparinization, in most cases, the ascending aorta was cannulated. In the majority of the cases, venous return was established with a two stage cannula placed in the right atrium. Cardiopulmonary bypass (CPB) was then initiated.
In patients with high risk of injury during sternotomy to the bypass grafts or the meadiastinal structures, CPB was initiated through peripheral cannulation either through the groin or the subclavian artery prior to sternotomy.
The patients were cooled usually to a target temperature of 32 °C.
After clamping the ascending aorta, myocardial protection was achieved by antegrade administration of cold blood cardioplegia (6 °C–8 °C).
In patients with a patent left internal thoracic artery (LITA) graft, it is carefully dissected and clamped. In case it is difficult to dissect the LITA graft, the patient is cooled down to 28 °C and then the aorta clamped, leaving the LITA graft open.
Graft material
Eleven distal LITA anastomosis was done in 10 patients, nine distal RITA anastomosis was done in 8 patients. 35 distal Venous anastomosis were done in 17 patients and 15 distal ansatomosis were done with Radial artery in 8 patients.
The average number of distal anastomosis was 2.8 ± 1.
Short Form 36(SF-36)
The SF-36 Health Survey is an extensive standardized, self administered, generic questionnaires for measuring both the physical and mental health of a patient. It was developed to assess the functional status and well-being of a patient. It consists of 36 questions in 8 areas. These 8 items include physical functioning (being able to perform physical activities), physical role (being able to do his/her job and daily activities), bodily pain (no pain or limitations due to pain), general health perception (evaluates personal health), vitality (enjoying life), social functioning (performing normal social activities or not), emotional role (problems with work or daily activities as a result of emotional problems), and mental health (feeling happy, peaceful and calm).
Three scales (i.e. physical functioning, role physical, and bodily pain) show high correlation with the physical component (PCS). Mental health and emotional role items mostly correlate with the mental component (MCS). Vitality, general health and social functioning correlate with both. Scores are converted to a 0–100 scale, which allows us to measure the scales numerically. The lowest scores indicate the lowest state of health and show functional limitation, severe social and role disability and distress. High scores indicate the absence of limitations and disability. In brief higher scores indicate a better health status.
Statistical Analysis
A score for each of the 8 items covered in the SF-36 from was calculated for each patient and compared with that of age matched general population. The results were then evaluated statistically using a paired samples t test, two-tailed correlation, and variant analysis. A p value smaller than 0.05 was considered to be statistically significant.
Results
All the pts. survived the operation. The 30 day mortality was 12%(3/25). Seven patients died during follow-up. Two of whom died of non-cardiac causes.
Follow-up
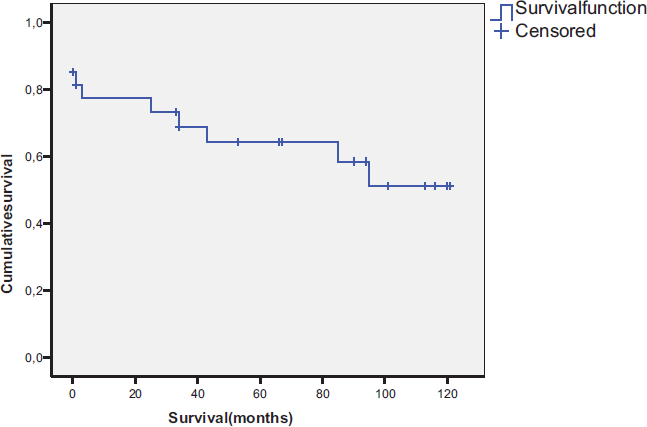
In 15 survivors median follow-up was 94 months (2–122 months). 1-, 5-, and 10-year survival were 77.8%, 65.0%, and 53.1%, respectively. Present NYHA status was significantly improved in comparison to preoperative values (2.4 ± 0.8 vs. 3.2 ± 0.56, p = 0.012). They had a mean survival of 6.4 ± 3.2 years.
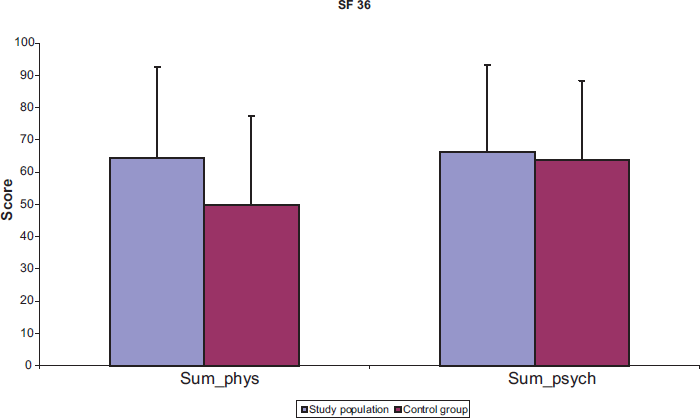
Quality of life was assessed by Short Form (SF)-36 Questionnaire. The scores were compared with age- matched general population. The SF-36 results for the pt. cohort were superior to those for the age matched general population.
The data are shown in Figure 1. The survivor curve is shown in Figure 2.
Discussion
Although the peri-operative risk of complications of first redo is higher than that of primary procedures, mortality of repeat CABG appears to be acceptable taking into consideration the technical difficulties and critical status of coronaries in these group of patients. 6
Recurrent angina pectoris due to bypass graft failure was a major indication for second and third CABG procedures, with venous grafts being more involved in our study.
The interval between the first and second operation was 60 ± 54.5 months and that between the second and third operation was 102.2 ± 47.7 months. This difference may be explained by the increased use of IMA and other arterial grafts as well as the fact that repeat operations are usually performed by more experienced surgeons, thus potentially reducing technical mistakes resulting in graft occlusion.
Many previous studies have shown that third time CABG is doable with acceptable results in selected group of patients.2–4,7 However, as far as we know no studies have been performed to assess the improvement in quality of life in this challenging patient cohort.
The main focus in this study was to compare the late surgical outcome and the quality of life after third time CABG in the survivors with an age matched population.
Assessment of quality of life using SF-36 is useful to evaluate the improvement in physical and mental state of the patients after CABG. It can also document successful therapies, especially from the patient's point of view.
One limitation in this study is the lack of pre-operative SF-36 assessments. This would require a prospective study design. There is however a pre-operative and post-operative NYHA classification. Post-operative NYHA status was significantly improved in comparison to pre-operative values (2.4 ± 0.8 vs. 3.2 ± 0.56, p = 0.012). Another limitation is the small number of patients in this patient cohort. There is a need for further studies.
Although the risk of a third redo CABG is relatively low, this is not a procedure that should be recommended lightly. Patients should be carefully assessed and other therapies e.g. Cardiac transplantation should also be considered. In our view, each patient should be considered separately and decision should be taken considering all the factors, including the availability of graft conduits.
Conclusion
This study suggests that both long-term survival and quality of life after third time CABG is acceptable compared to age matched general population. Significant improvement of NYHA status and acceptable quality of life results justifies the surgical approach in this challenging patient cohort.
Conflicts of Interest
The authors have no ethical problems or conflicts of interest associated with this manuscript.