
Abstract
Myxomas are rare neoplasms of mesenchymal origin. Diagnostic evaluation requires histopathological confirmation. We report a rare case of atypical orbital myxoma with radiographic and histopathological correlation.
Keywords
A 40 year old, previously healthy female complained of retro-orbital pressure, recurrent upper eyelid swelling, photophobia, headache and an increasingly protruding left eye of 3 months duration. She had experienced more subtle signs of orbital congestion for approximately a year. Her past medical history was unremarkable, and no extra-orbital manifestations had been reported.
General physical exam was normal without any appreciable skin lesions. Uncorrected visual acuity was 20/20 in both eyes. Her pupils were symmetric, briskly reactive to light, and without relative afferent pupil defect. Evaluation of extraocular movements, slit lamp bimicroscopic examination, and indirect ophthalmoscopy were unremarkable. Intraocular pressures were 16 mm OD and 23 mm OS.
Orbital evaluation confirmed 3 mm of left hypoglobus and 6 mm of axial non-pulsatile proptosis. There was mild non-erythematous edema of the left upper and lower eyelids, increased resistance to retropulsion, but no discreet palpable mass.
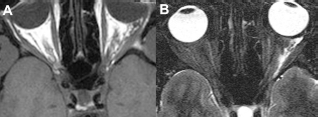
Preoperative contrast enhanced computed tomography (CT) of the orbits revealed a minimally enhancing soft tissue mass in the intraconal left orbit. The mass had ill-defined borders and was located primarily inferolaterally, inseparable from the inferior and lateral rectus muscles and extended to the inferior orbital fissure. The optic nerve was separate from the mass but deviated medially. There was no obvious bone involvement (Fig. 1). On MRI, the mass demonstrated isotense signal intensity to muscle on T1-weighted images, markedly increased signal intensity on T2 weighted images and heterogeneous enhancement on gadolinium-enhanced T1 weighted images with fat saturation.

preoperative Diagnostic Imaging. (
The patient underwent an inferior-lateral orbitotomy via swinging eyelid incision (Fig. 2), after a fine needle aspiration biopsy revealed “neoplastic cells of an undetermined origin.” An indistinct purple mass with the consistency of friable mucosa intermixed with stringy mucoid-like material was encountered and dissected in a piecemeal fashion from the orbital fat with pituitary forceps. Histopathological examination of the mass revealed a myxoid lesion around extraocular skeletal muscle. (Fig. 3A) The lesion exhibited a patternless yet focal and fascicular spindle cell neoplasm with short tapering nuclei and indistinct cytoplasm. (Fig. 3B) These cells were distributed in a copious myxoid matrix containing a small number of capillaries. Mild nuclear hyperchromasia was present without any significant pleomorphism and mitotic activity was not easily visualized. The neoplastic cells were immunoreactive to vimentin (Fig. 3C) and negative to CD34, Myo D1, desmin, factor XIIIa, SMA, ER, PR and S-100 protein. Cytogenetic study revealed a “female karyotype with multiple aberrations in four cells, finding can be seen in mesenchymal neoplasm but nonspecific to further classify the lesion”. The final diagnosis was an atypical myxoid spindle cell neoplasm.

Intraoperative photograph, surgeon's view, depicting diffuse nature of tumor, approached using a bone-sparing infero-lateral orbitotomy.

Histological appearance of orbital myxoma (
The patient has been followed with serial examinations and MR imaging for 3 years without recurrence (Fig. 4). There was normalization of the clinical examination. MRI demonstrated a small amount of residual T2 signal. The follow-up 18 F-FDG PET also demonstrated uptake in the lateral aspect of the left orbit (SUV of 6.7) consistent with residual tumor. There was no evidence of increased remote FDG uptake to suggest metastatic disease.
postoperative MRI (2 months) (
Discussion
Myxoma is a benign neoplasm derived from connective tissue, consisting chiefly of polyhedral and stellate cells that are loosely embedded in a soft mucoid matrix, thereby resembling primitive mesenchymal tissue. 1 These mesenchymal derived cells develop along fibroblast cell lines that procure excess glycosaminglycans, hyaluronic acid and chodroitin sulfate that inhibit the polymerization of normal collagen fibrils. 2 Although myxoma may appear encapsulated owing to compression and condensation of the surrounding tissues, they lack a true capsule and are locally infiltrative. Histologically, the tumor is composed of scattered stellate or spindle-shaped cells and a few multinucleated cells in the background of myxoid stroma, rich in hyaluronidase. Nuclear atypia and mitoses are infrequent. Lymphocytes and plasmacytes are regularly found. Hemosiderin, a result of hemorrhage into the tumor, is commonly present. Myxoma cells usually express interleukin-6 3 and some tumor have abnormal cellular DNA content. 4 Due to the tumor's high concentration of acid mucopolysaccharides and hyaluronic acid, the mucoid tissue stains red and blue with mucicarmine and Alcian blue respectively. Alcian blue also stains positive in chondromas and chondrosarcomas. While these stains are not diagnostic they can be valuable in the differential diagnosis of these mucoid-producing soft tissue tumors. 5
While these tumors are most commonly associated with intramuscular pathologies of the heart, skin, subcutaneous tissues, and skeletal muscle, there are only a few reported cases existing within the orbit. The most common ocular presentation is in the eyelid as a solid lesion,2,6–7 but cases have been described affecting the conjunctiva, 8 11 cornea, 12 as well as in association with the Carney's complex. 13
It is unclear why myxomas rarely involve orbital tissue. Approximately 23 cases have been described affecting the orbit and orbital bones.5–7,14–26 However we present the first case of an orbital myxoma with nuclear atypia, an exceedingly rare finding on histopathological examination. Myxomas are true neoplasms of primitive mesenchyme that do not metastasize, but local recurrence is possible after incomplete surgical resection. Soft tissue myxomas usually present clinically as painless masses. Growth is usually slow and progressive. Occasionally, there may be a period of accelerated growth, due to myxoid degeneration in these tumors. 22
It is important to differentiate myxomas from the wide spectrum of benign neoplastic processes that show myxoid degeneration, such as, nodular fasciitis, schwanomma and neurofibromas, and malignant lesions such as myxoid chondrosarcoma and malignant fibrous histiocytoma. Unlike benign myxomas, sarcomas display areas of increased cellularity, pleomorphism, mitotic activity, and a rich vascular network. Before confirming a diagnosis of myxoma, all myxomatous tumors should have a thorough histologic evaluation for mitotic activity and an immiunohistoxhemical evaluation to eliminate the possibility of a sarcomatous component. 22 Upon confirmation of the diagnosis, wide local surgical resection is the optimum treatment of choice. However there has been a report of successful medical management of the tumor with cyclophosphamide. 27 Incomplete excision is a common reason for tumor recurrence.
Disclosure
Author(s) have provided signed confirmations to the publisher of their compliance with all applicable legal and ethical obligations in respect to declaration of conflicts of interest, funding, authorship and contributorship, and compliance with ethical requirements in respect to treatment of human and animal test subjects. If this article contains identifiable human subject(s) author(s) were required to supply signed patient consent prior to publication. Author(s) have confirmed that the published article is unique and not under consideration nor published by any other publication and that they have consent to reproduce any copyrighted material. The peer reviewers declared no conflicts of interest.
Footnotes
Acknolwedgement
This work was supported in part by an unrestricted grant from Research to Prevent Blindness, New York, New York, The Eye Institute of New Jersey, Newark, and the Gene C. Coppa Memorial Fund, Newark.