
Abstract
Objective
To outline the pharmacodynamics, efficacy and safety of besifloxacin ophthalmic suspension 0.6% in the treatment of bacterial conjunctivitis.
Quality of Evidence
MEDLINE database was searched to review recent pharmacodynamic and clinical studies evaluating besifloxacin and comparing besifloxacin to other topical antibiotics for ophthalmic use. Findings were limited to full-text articles from clinical journals in the English language.
Main Message
Bacterial resistance is a common source for treatment failure in bacterial conjunctivis. Besifloxacin, a novel fourth generation synthetic fluoroquinolone is likely to show lower resistance rates due to its mechanism of action and its short-term use for ocular infections only (decreased systemic exposure). Besifloxacin displays improved pharmacodynamic properties compared to other commonly used fluoroquinolones and has shown to be efficacious and safe in clinical studies.
Conclusion
Besifloxacin ophthalmic suspension 0.6% provides safe and efficacious treatment for bacterial conjunctivitis. The factors leading to bacterial resistance are diminished, which allows besifloxacin to be a favorable treatment option.
Introduction
Acute conjunctivitis is a common ocular condition that affects all age groups. While viral conjunctivitis, also known as pink eye, is thought to be most common, it is estimated that up to 78% of all cases of acute conjunctivitis in children and 50% of cases in adults are of bacterial origin. 1 In fact, bacterial conjunctivitis is the most common eye condition seen by primary care physicians, and may account for up to 1% of all primary care visits. 1 Bacterial conjunctivitis can be often be distinguished from viral conjunctivitis by signs such as mucopurulent discharge, chemosis, conjunctival injection and crusting with mucopurulence being a key distinguishing factor. The most common causative microbes in adults include gram-positive: Staphylococcus aureus, Staphylococcus epidermidis and Stretococcus pneumoniae and the gram-negative pathogen Haemophilus influenzae. S. aureus is the most common in adults, while children are most prone to H. influenzae.
Like viral conjunctivitis, bacterial conjunctivitis is generally a self-limited condition usually lasting 7 days. 2 Level I evidence has shown that patients not treated with antibiotics have high spontaneous remission rates, marginal benefits, and low risk of adverse outcomes. 3 Nonetheless, evidence also suggests that topical antibiotics can shorten the disease time, reduce contagious spread, reduce time off work/school, 4 and reduce the risk of progression to potentially irreversible ocular damage. 5 Thus, the current recommended strategy for managing acute infectious conjunctivitis is to promote supportive care for the first couple days of symptoms and then, if no improvement, start topical antibiotic drops. 3 Supportive care includes frequent eye cleansing with sterile water and gauze, warm water compresses, proper hand and eyelid hygiene, and temporary use of artificial tears for comfort. However, if the conjunctivitis presents with marked mucopurulence, it would not be unreasonable to immediately begin topical broad-spectrum antibiotic treatment along with the supportive care.
Once antibiotics are clinically indicated, the standard of care for bacterial conjunctivitis is broad-spectrum topical ophthalmic antibiotic eye drops. Various classes of antibiotics have been used including aminoglycosides, polymyxin B combinations, macrolides, sulfonamides and fluoroquinolones. Aminoglycosides (tobramycin and gentamycin) require frequent dosing (1–2 drops every four to six hours for ten days), which can lead to poor patient compliance. In addition, despite their frequent use, aminoglycosides demonstrate poor antimicrobial activity against Streptococci, which limits their use as a broad-spectrum treatment for conjunctivitis. 4 Azithromycin is not preferred due to its unequal gram-negative and positive coverage. 6 Erythromycin is no longer recommended because its activity against S. aureus has diminished. 4 Fluoroquinolones are still considered by many to be the antibiotics of choice for ocular infections on account of their broad-spectrum potency and low toxicity.7,8
One major consideration in the selection of an antibiotic is bacterial resistance. In the absence of routine swabbing, microbial culture and sensitivity determination, clinicians rely upon low levels of resistance to increase the likelihood the treatment choice will be efficacious. Development of resistance may be caused by a number of factors including antibiotic overuse in systemic infections, prophylactic use, sub-therapeutic use and misuse in non-bacterial infections. 9 Resistance has been noted in the third generation fluoroquinolones (ciprofloxacin, levofloxacin and oxfloxacin) 10 12 and rates of resistance are increasing, especially for gram-positive bacteria. 13 Although the newer fourth generation fluoroquinolones, gatifloxacin and moxifloxacin have lower published rates of resistance, 7 these numbers are increasing likely due, in part, to their use in systemic infections 11 and in part to their ubiquitous use in the treatment of conjunctivitis and prophylaxis of the ocular surface at the time of surgery. The Ocular Tracking Resistance in the United States Today (Ocular TRUST) has documented that 18.9% methicillin-sensitive S. aureus isolates are resistant to gatifloxacin and 15.9% are resistance to moxifloxacin. 11 Of particular concern is the increase in methicillin-resistant S. aureus (MRSA) isolates. Between 2000 and 2005 the proportion of MRSA isolates in ocular infections has jumped from 29.5% to 41.6%. 12 Studies have shown that resistance rates for MRSA range from 68%–85% for moxifloxacin and 71%–85% for gatifloxacin.11,14,15
Thus, there is an increasing demand for an effective antibiotic for bacterial conjunctivitis with low rates of bacterial resistance that is effective in treating the most prevalent ocular infections and which can be used reliably as an empiric therapy due to its broad-spectrum coverage. The aim of this paper is to provide evidence based information on besifloxacin to evaluate its role and patient preference in the treatment of acute bacterial conjunctivitis.
Sources of Information
MEDLINE was searched up to a cut off of October 2010 using the following MeSH terms: conjunctivitis with bacterial, epidemiology, antibiotic therapy, besifloxacin with safety, clinical trials, pharmacodynamics and pediatrics. The results of the search were limited to full-text articles from core medical journals in the English language.
Main Message
Besifloxacin
Besifloxacin ophthalmic suspension 0.6% (Besivance, Bausch & Lomb Inc., Rochester, NY, USA) is fourth generation topical fluoroquinolone recently approved by the FDA and HPB (in Canada) for treatment of bacterial conjunctivitis in adults and children older than 1 year. Besifloxacin is the only fluoroquinolone specifically designed for ocular use. Unlike older antibiotics of this class, besifloxacin is not used for systemic infections. Restriction to topical use only, renders besifloxacin unique in its class and theoretically reduces the risk for the development of resistance due to decreased systemic exposure. 2
Mechanism of Action
Consistent with other fluoroquinolones, besifloxacin binds to DNA gyrase and topoisomerase IV, two enzymes that are critical for DNA replication in bacteria. Unlike previous generations in this class, besifloxacin has a relatively equal affinity for inhibiting the above enzymes. 16 The preferential targeting of one enzyme over the other is one factor that contributed to the resistance rates in the previous fluoroquinolone generations. 13 Resistance to besifloxacin would require spontaneous mutation in two enzymes, which is a less probable event.
Besifloxacin (7-[(3R)-3-aminohexahydro-1H-azepin-1-yl]-8-chloro-1-cyclopropyl-6-fluoro-1,4-dihyrdo-4-ixi-3-quinolinecarboxylic acid) has a novel C8 chlorine group and C7 amino-axepinyl group (Fig. 1) that are thought to increase potency and increase broad spectrum activity. 17 Besifloxacin has shown to have broad spectrum activity against gram-positive, gram-negative and anaerobic bacteria. 18

Chemical formula of besifloxacin.
Pharmacokinetic Studies
In order for a topical antibiotic to be effective, it must achieve a therapeutic concentration on the ocular surface. Eye drops are quickly diluted by tears, spilled on the skin and absorbed through the nasolacrimal ducts. 19 Besifloxacin is an ophthalmic suspension 0.6% (rather than a solution) and, as such, is formulated with a mucoadhesive agent (Durasite; Insite Vision, Inc., Alameda, CA), which increases the drug exposure to the ocular surface. 20
A number of pharmacokinetic parameters are important in predicting the clinical efficacy of a topical antibiotic. These include:
Cmax – peak concentration
AUC – area under the concentration vs. time curve (24 hours)
MIC90 – minimum concentration to inhibit 90% of a specific pathogen
MBC90 – minimum concentration to eradicate 90% of a specific pathogen
Kill rate – rate at which a specific pathogen is eradicated
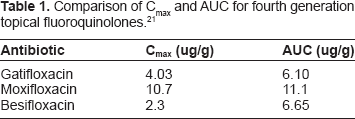
Pharmacokinetic trials on humans comparing the most recent generations of topical fluoroquinolones have been completed (Table 1). Although having a lower Cmax and AUC, besifloxacin demonstrates the longest mean residence time (MRT) in the conjunctiva at 4.7 hours. 21
Comparison of Cmax and AUC for fourth generation topical fluoroquinolones. 21
The ratio of AUC:MIC90 is an important predictor of an antibiotic's efficacy. In fact, for fluoroquinolones, the AUC:MIC90 is the pharmacodynamic parameter that best correlates to clinical efficacy. 22 25 In keeping with this finding, the above pharmacokinetic data is only relevant when the MIC90 of specific pathogens for each antibiotic is considered (Table 2).
Comparison of the AUC:MIC90 for new generation fluoroquinolones 100. 21

The AUC:MIC90 quantifies how much antibiotic is present compared to the minimum concentration required to kill 90% of pathogens over a 24 hours period. Besifloxacin demonstrates a higher AUC:MIC90 among the common isolates found in bacterial conjunctivitis and is present in therapeutic amounts in methicillin resistant infections. In addition, dosing of besifloxacin at three-times-a-day (t.i.d) results in a doubling to tripling of the AUC, ensuring that the antibiotic is present at concentrations substantially higher than the MIC90.
It is important to note that the above studies do not account for the high concentration of antibiotic in the tear film. The effect of antibiotic in the tear film on bacterial eradication has not been studied, but one could speculate that this would be a synergistic factor.
Furthermore, besifloxacin demonstrates a lower MBC (minimum bacteriocidal concentration) than moxifloxacin, gatifloxacin, ciprofloxacin, azithromycin and trobramycin for S. aureus, S. epidermis and S. pneumoniae. This indicates that besifloxacin is the most potent antibiotic against the above-mentioned pathogens. However, gatifloxacin and ciprofloxacin have a lower MBC for H. influenzae. In addition, time-kill assays have demonstrated that besifloxacin has dose dependant bactericidal activity and has more rapid bactericidal activity than moxifloxacin and ciprofloxacin for many of the common bacterial isolates in conjuncitivitis. 18
Pharmacokinetic studies indicate that systemic toxicity of besifloxacin is unlikely. Topical t.i.d dosing of besifloxacin to human subjects with bacterial conjunctivitis resulted in a negligible (<0.5 ng/ml) systemic exposure, thus resulting in low systemic toxicity. 26
Clinical Studies
Besifloxacin ophthalmic suspension 0.6% has been evaluated in three clinical trials, all of which have demonstrated efficacy.2,27,28 All studies used dosing as per besifloxacin guidelines: 3 drops per day (at 6 hour intervals) for 5 days. The three clinical trials were industry sponsored.
A 2009 multicenter, randomized Phase III study involving 390 patients demonstrated superior clinical resolution and bacterial eradication with besifloxacin compared to the vehicle (Table 3). 28 All patients had culture-confirmed bacterial conjunctivitis. Patients receiving besifloxacin demonstrated significantly more clinical resolution than patients receiving the vehicle at day 5 (45.2% vs. 33.0%, p = 0.008) and day 8 (84.4% vs. 69.1%, p = 0.0011). In addition, besifloxacin-treated patients had significantly higher rates of microbial eradication at day 5 (91.5% vs. 59.7%, p = <0.0001) and 8 (88.4% vs. 71.7%, p = <0.0001).
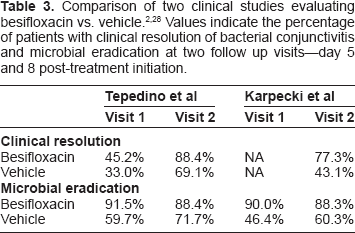
Another study published in 2009 was a multicentre, randomized Phase II study involving 118 patients. The results demonstrated superior clinical resolution and bacterial eradication with besifloxacin compared to the vehicle (Table 3). 2 Again, all patients had culture-confirmed bacterial conjunctivitis. Patients receiving besifloxacin demonstrated significantly more clinical resolution than patients receiving the vehicle at day 8 (77.3% vs. 43.1%, p < 0.0001). In addition, besifloxacin-treated patients had significantly higher rates of microbial eradication at day 4 (90.0% vs. 46.4%, p = <0.001) and 8 or 9 (88.3% vs. 60.3%, p = <0.001).
A 2009 multicenter, randomized study involving 533 patients demonstrated that besifloxacin was not inferior to moxifloxacin in the treatment of bacterial conjunctivitis. 27 All patients were culture-confirmed. There was no significant difference in clinical resolution between besifloxacin and moxifloxacin on day 5 (58.3% vs. 59.4%, 95% CI = –9.48 to 7.29) and day 8 (84.5% vs. 84.0%, 95% CI = –5.67 to 6.75). In addition, there was no significant difference in bacterial eradication between besifloxacin and moxifloxacin at day 5 (93.3% vs. 91.1%, 95% CI = –2.44 to 6.74) and day 8 (87.3% vs. 84.7%, 95% CI = –3.32 to 8.53).
A post hoc, subgroup analysis of the studies described above found that besifloxacin was efficacious in pediatric patients aged 1–17. 29
Safety and Tolerability
A recent meta-analysis of data from 1192 patients taking part in besifloxacin trials demonstrates a favorable safety profile. 30 Systemic exposure was negligible. The most common adverse events in patients receiving topical besifloxacin were local and included blurred vision (2.1%), eye pain (1.8%), eye irritation (1.4%), nonspecific conjunctivitis (1.2%) and eye pruritis (1.1%). Of note, blurred vision, eye irritation and eye pruritis occurred more commonly in patients receiving only the vehicle (p < 0.05). Besifloxacin topical administration did not affect visual acuity.
Conclusions
Patient preference and place in therapy
The current recommendation for management of acute infectious conjunctivitis is a short course of supportive management followed by the use of topical ophthalmic antibiotic drops if symptoms are not improving. Besifloxacin ophthalmic suspension 0.6% is a reasonable treatment option because of its low resistance profile, clinical efficacy and safety. Besides resistance, patient compliance is another route for failure in the treatment of bacterial conjunctivitis due to frequent dosage. 4 Besifloxacin has the most favorable dosing schedule (one drop, three times a day for seven days) of all the fluoroquinolones, which could aid in patient compliance. Approximate pricing of besifloxacin falls between that of moxifloxacin and gatifloxacin (Table 4).
Approximate prices (CAD) of fourth generation fluoroquinolone ophthalmic solutions.

London Health Sciences Centre, Drug Formulary. Accession date: December 15, 2010.
Development of bacterial resistance is inevitable in heavily prescribed antibiotics. It is essential to be cognizant of these resistance rates and to be knowledgeable of new agents when empiric and efficacious treatment is essential. Besifloxacin is a new molecule in the family of fourth generation fluoroquinolones with improved efficacy, making it useful in the treatment of acute bacterial conjunctivitis.
Disclosures
This manuscript has been read and approved by all authors. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The authors and peer reviewers of this paper report no conflicts of interest. The authors confirm that they have permission to reproduce any copyrighted material.