
Abstract
Although ocular tissues involved in aging macula disorder (AMD) were already known in 300 BC, the last type of photoreceptors was discovered only 10 years ago. The earliest descriptions of AMD appeared around 1850. It took over 150 years, till a clearer concept of AMD was formulated and even longer to grasp its pathophysiology. The uncertainty of researchers about the pathogenesis of AMD over the last century is reflected in its changing terminology. The evolution of this terminology is provided in a table to afford the reader a better insight into explanations proposed by researchers during this quest.
Keywords
Introduction
Without a clear concept of a disease, it is hardly possible to perform good research, such as epidemiologic and genetic. For example, amyotrophic lateral sclerosis was described in 1874, and eluded for decades genetic researchers, until it was found to comprise over 20 different disorders. I suspect that the same may hold for open-angle glaucoma. Only since 1970 we know substantially more about aging macula disorder (AMD). However, I discovered that the first descriptions of AMD, although under a different name, appeared in 1852. It took over a century and a half before a clearer conception of AMD emerged, and its high prevalence, as well as its impact on the quality of life of many elderly people, was appreciated.
The purpose of this article is to give a historical overview of the earliest descriptions of retinal and surrounding tissues associated with AMD. I also comment on earlier theories about their functions. Next, the later development of its terminology is reviewed, which partly reflects the pathophysiological considerations over time. In a historical medical investigation, one may adopt a strictly chronological approach or a more anatomical one. I preferred the latter to avoid a jumble of dates and medical terms. Therefore, the different historical facts relevant to each adjacent layer of the eyeball, from the sclera to the retina, are mentioned. An overview of the anatomy of the eye around the start of our era may be found elsewhere. 1
The Choroid
The choroid was known before the retina and seems to have been drawn by Democritus of Abdera around 400 BC. 2 He named the outer coat of the posterior pole of the eye chitoon puknotatos (dense tunic) and its inner coat chitoon malista somphos (more spongy tunic). About 100 years later, Hippocrates replaced the term dense outer tunic of the eye with to leukon (the white) and divided the spongier tunic into the two parts: an outer meninx leptotera (delicate membrane) and an inner arachnoeides (the cobweb like), all encircling to hugron (the moist). 2 Thus, both the spongier tunic and its outer delicate membrane appear to have been what we now call the choroid. The ancient Greeks did not use the word chorion for our choroid; the chorion was a membrane enclosing the fetus in the womb, the after birth, or the membrane on the inside of the egg-shell. The name chor(i)oeides chitoon (tunic like a chorion) in the eye appears for the first time in Celsus at the start of our era. 2
The human choroid adheres to the sclera with a lamina fusca (dark brown layer), a loose cellular tissue with elongated pigmented cells. In 1722, Ruysch 3 demonstrated the detailed choroidal vasculature, in drawings of choroidal casts he made with a secret wax formula, 40 years before Haller. Modern textbooks, nevertheless, mention that the choroid is divided into the large vessel layer of Haller, the smaller vessel layer of Sattler (who mentioned nine layers in the choroid), and the choriocapillaris. According to Eschricht, 4 Hovius 5 first described the choriocapillaris. On translating Hovius's Latin text, however, I could not find a capillary layer or membrane mentioned in it. 6 In any case, the name choriocapillaris was coined by Eschricht. 4 Henric Ruysch called the choroidal layers tunica Ruyschiana, to honor his father Frederik, but on close reading, this tunic seems to be a collective name for the choroid, the choriocapillaris, the retinal pigment epithelium (RPE), the tapetum, and Bruch's membrane (BrM).
The Retina
It remains unclear why the name arachnoeides (like a cobweb) which Hippocrates gave around 350 BC to the layer surrounding to hugron (the vitreous) was changed later to amfibles-teroieides chitoon (tunic like an amfiblestron). Amfiblestron at that time had seven meanings, and one of these, casting net, was arbitrarily preferred above encircling wall or bond (of the vitreous) for retina, hence the word rete (net) in retina. 1 The word retina was coined around 1150 AD in a Neo-Latin translation of an Arabic text. 7 In his Coliget, Ibn Rushd Aver-roes (1126–1198) might have attributed photoreceptor properties to the retina, and he was possibly the first to suggest that the principle organ of sight was the arachnoid membrane (aranea). 8 His work led to much discussion in the 16th century Europe as to whether the principle organ of sight was the traditional Galenic crystalline humor or the Averroist aranea. Platter 9 claimed in 1583 that the retina and not the lens was the light-sensitive organ in the eye. Nearly 100 years later, van Leeuwenhoek 10 mentioned clootgens at the end of the fibers of the optic nerve spreading in the eye, which transmitted visible objects to the brain. He used the word clootgens in Dutch both to indicate cells and fat globules. The translation of clootgens as globules in his letter to the Royal Society in London simply may have blurred this distinction. About 150 years later, the photoreceptors were rediscovered, 11 and Kölliker 12 separated cones and rods in the human retina as two types of photoreceptors. It was only in 2002 that a third type was described, photosensitive ganglion cells. 13
Bruch's Membrane
Let us now first consider BrM, and the RPE with their AMD-associated changes, before moving on to the macula. BrM is an extracellular matrix between the choriocapillaris and the RPE and may be considered to belong both to the choroid and the retina. Bruch 14 described this membrane, which was named after him, in his monograph of 1844 on granular pigments in vertebrates. Bruch wrote that Eschricht had already described this membrane in the seal six years earlier. Eschricht actually mentioned an extremely thin, serous membrane between the choriocapillaris and the retina (Table 1), so BrM should have been called Eschricht's membrane. 4 Early researchers noticed that BrM becomes thicker around age 70 years. 15 It thickens over time by 135% whether signs of AMD are present or not. 16 Histologically, half of 13 eyes with disciform macular degeneration (dMD) had ruptures in BrM, which were crossed by new vessels. 17 So for about 80 years, people knew that changes in BrM were associated with neovascularization and what we now call wet late AMD. BrM has a basement membrane on both sides and three inner layers, 18 and only recently three types of multilaminar sub-RPE hyperreflectivity were detected with optical coherence tomography in the inner, the outer, or both layers of BrM in eyes with regressing drusen. 19
Various names for Bruch's membrane in chronological sequence.

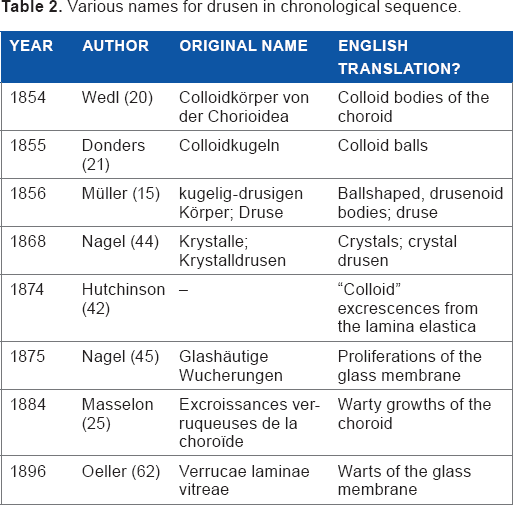
Drusen, the hallmark of AMD, were first described in 1854 by Wedl 20 who had no idea where they came from or what they indicated. Their connection with AMD remained obscure for over a century, and even Haab who first coined the term senile macular illness (Fig. 1) explicitly denied that drusen had anything to do with this disorder. Around 1850, three authors, Wedl, Frans Donders, and Heinrich Müller, gave drusen different labels (Table 2). Wedl named them colloid bodies of the choroid and thought that they were incompletely developed cells, because they had no cell membrane or nucleus. 20 Donders called them colloid balls surrounded by pigment, noting their preference for the macular area. He was convinced that drusen originated from the nuclei of the pigment cells, which he believed to belong to the choroid. 21 Müller mentioned deposits on the inner side of the choroid that had a ball-shaped or drusenoid form. In this 1856 article, he coined the word druse. He thought that drusen originated from thickenings of the structureless membrane on the choroidal inner side behind the pigment cells. 15 Druse is the German word for geode, a cavity in rock filled with crystals, and Müller probably chose this name because of the crystalline core in some large drusen. Later, the theory was formulated that drusen originate from leucocytes. 22 It is striking that 160 odd years on, we still do not know where exactly drusen originate from. The latest candidate again is the RPE, 23 as Donders suggested. Over the years, several subtypes of drusen were discovered, one of the most recent being reticular, cuticular, or pseudodrusen. 24
Various names for drusen in chronological sequence.

(
Around 1884, drusen were even thought to be the cause of posterieur glaucoma because drusen usually were located around the optic disk, leading to the assumption that thickening of the glasslike layer around the choroidal ring hampered the outflow of ocular fluid. 25 This view was supported by the fact that drusen as well as glaucoma normally were present in both eyes of old persons.
The RPE
Mondini 26 desrcibed in 1791 an actual net-shaped membrane composed of numerous interlinked, black globules, and thus was the first to mention the RPE. He also wrote that Malpighi told Valsalva that the inner side of the choroid was lined by small black globules. Mondini already thought that the pigment served to dampen stray light rays and to attach the retina to the pigment layer. His son Francesco added that the pigmented globules were polygonal that there were no blood vessels between this pigmented layer and the retina and that the black pigment possibly was iron oxide because it was heavier than water and was attracted by a magnet. 27 Around 1820, Jacob 28 confused many authors by referring to a membrane under the retina, running from the optic nerve to the ciliary processes, and this led to a tiring discussion according to Eschricht. 4 On rereading Jacob, one has no idea what he meant, although Bidder thought that Jacob's membrane was the rod layer of the retina. In the first description of the RPE as the membrane of the pigment, hexagonal cells were mentioned that were circular in the human fetus and in albino animals. 29 Bruch 14 gave an elaborate description of the RPE and was struck by its monolayer and regular, hexagonal shape. He pointed out that the cones were standing directly on the RPE cells without any membrane or structure between them and that they had a pigment sheath. Donders mentioned in 1855 RPE atrophy between groups of drusen. 21 It gradually became clear that the RPE could become hypertrophied and after fibrous metaplasia could contribute to fibrous tissue in disciform lesions.17,30–32
Basal laminar or basal linear deposits are located between the cell membrane and the basement membrane of the RPE and are often present before drusen appear. Tese terms were not used in the original electron microscopic descriptions of these deposits. 33 Gass 32 called them “eosinophilic material between an irregularly thickened BrM and overlying degenerated RPE”. Shortly later in 1970, Sarks identified three types of deposits, 34 and it seems that she coined the term basal linear deposit. 35
The Macula
In 1782, Buzzi described the macula lutea after dissecting the eyes of a 35-year-old man in the following terms. Thus, in a point lateral to the optic nerve, and also in a healthy condition, one may often see that the retina is colored yellow, be it rather vague. 36 Soemmering 37 thought in 1796 that the macula was a hole in the central retina surrounded by a yellow ring, but soon later, it was mentioned that the macula was just a thin spot in the retina.38–40 Cuvier 38 wrote that the macula had no color in the neonate but was yellow in the adult. The exact size of the macula was a matter of long discussion, and the area of the central fovea was calculated to be 0.12 mm2 in accordance with its capillary-free zone. 41
First Reports on AMD
The pathogenetic process underlying AMD is still not clear, or the tissue primarily involved in it. It seems generally accepted that thickening of BrM and drusen formation in BrM and the RPE, as well as RPE detachments and subretinal hemorrhages, precede retinal changes of a secondary nature like photoreceptor loss and scarring.17,42,43
In his early medical career, Donders performed many autopsies. From 1852 on, he realized the gap in understanding between what he saw using the ophthalmoscope (for a few months in his possession) and the microscope. So he started collecting healthy postmortem eyes for histology. In 1855 after examining 38 apparently healthy eyes, he wrote “An important question is in how far the degeneration described here (in the retina), can lead to visual disturbances”. 21 Using microscopy, he noticed rods, obliquely oriented, around small drusen as well as degeneration of the choriocapillaris and the RPE. Rods and cones often were absent above drusen that sometimes penetrated the retina halfway, without expanding the retina on the vitreous side. Drusen compressed the retina (Fig. 2) and rarely were absent in the eyes of persons aged 70–80 years. In none of the eyes he examined postmortem, the visual acuity had been carefully recorded before death. However, Donders considered that the anatomical relation of the drusen to the retina and the degeneration of the RPE had to have an influence on retinal function. He was convinced that the white flecks that he had seen several times with the ophthalmoscope in the eyes of old people suffering from senile amblyopia (as loss of visual acuity in the elderly was called at that time) were not fatty metamorphoses but colloid degenerations. 21 An enviable clinical insight on his part.
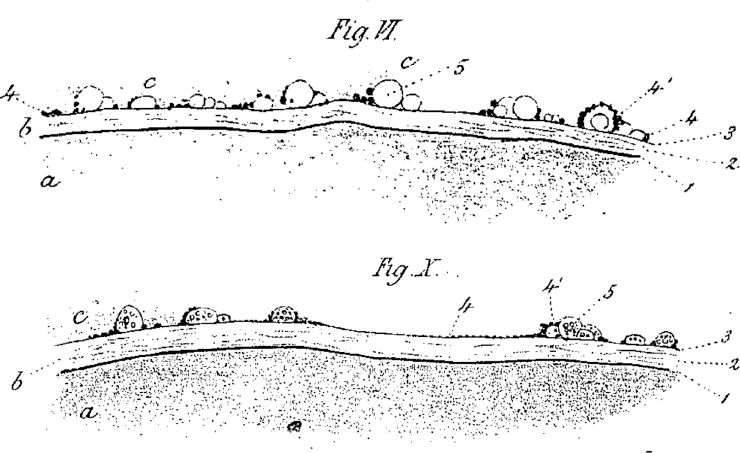
Large drusen 5 pressing against the retina (c). a is choroid, b is probably Bruch's membrane, and c is retina in which drusen protrude. 21
Nagel 44 was probably the first to publish on AMD, using both clinical and histological data from the same patient. In 1868, he published on a 64-year-old woman with a dark-red net and partly confluent white flecks around both maculae who complained about marked amblyopia, metamorphopsia, and a quivering image. Fine brilliant specks were seen with ophthalmoscopy, creating the impression of Krystalldrusen. In 1874, the patient complained about more metamorphopsia. This involved, for instance, human legs appearing bent. Nagel 45 published again on this and two more cases in 1875. The visual fields of these patients were normal, and the eyes were never painful or inflamed. His first patient died at age 73 years due to an abdominal tumor; the eyes were enucleated 27 hours postmortem, and one was put in Müller's fixative. In the nonfixated eye, there were small, sparkling irregularities in the posterior pole on the inner side of the choroid. Flecks around these irregularities were created by thickening of the elastic layer where the dissolved drusen had been and the outer retinal layer over them was markedly thinner. Nagel thought that this could explain the metamorphopsia and amblyopia the patient complained of. So Donders and Nagel described drusen that caused degeneration of the choriocapillaris, the RPE, and thinning of the neuroretina with vision loss without, however, formulating a concept of macular degeneration (MD).
Descriptions of AMD from 1855 Onward
Table 3 lists the huge variety of terms, which have been applied to what was probably AMD during the last 160 years. Only those that seem relevant, either because of their widespread use or because of the pathophysiological concept they indicate, will be commented on.
Terminology of aging macula disorder (AMD) from its very beginning †
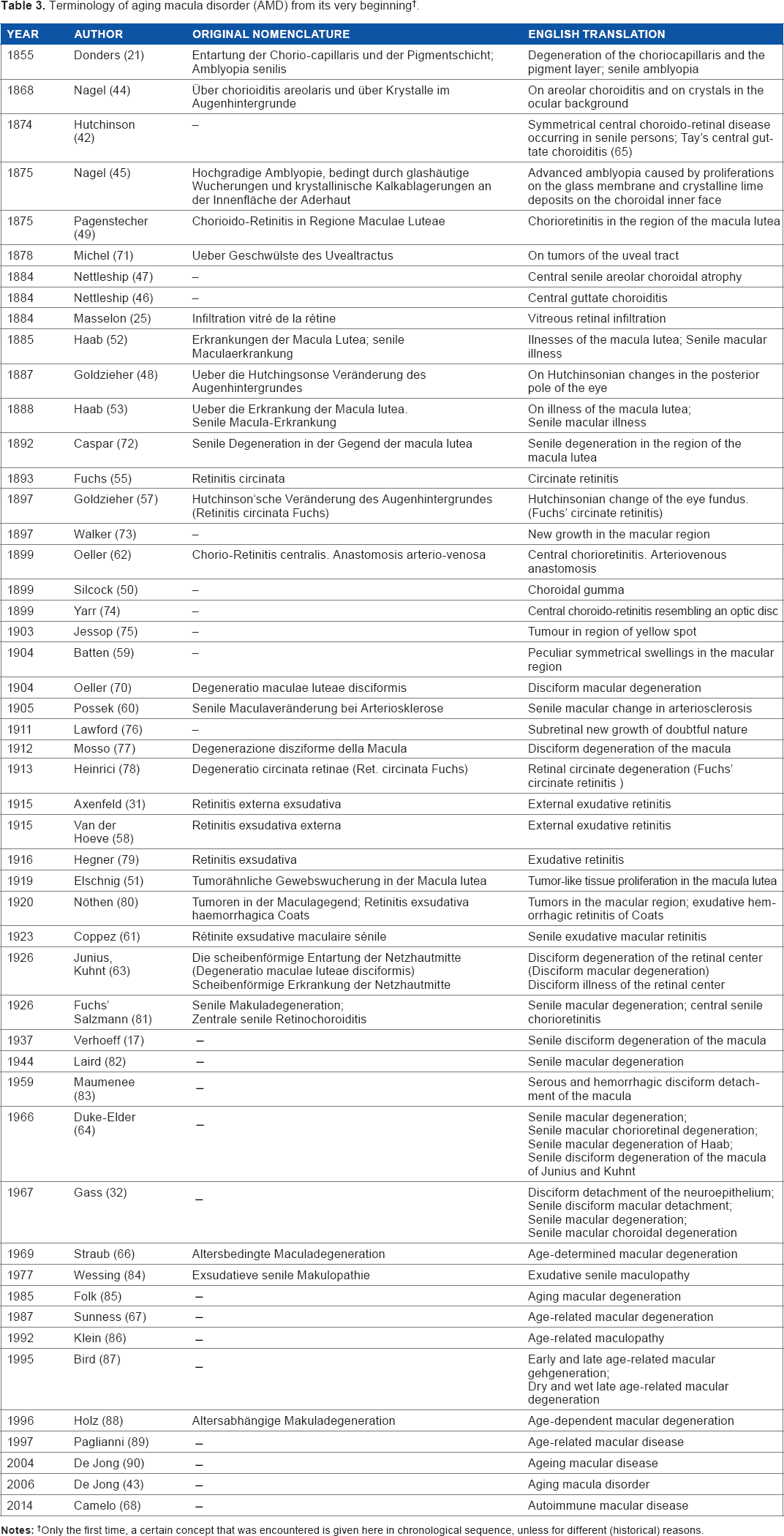
Only the first time, a certain concept that was encountered is given here in chronological sequence, unless for different (historical) reasons.
In 1874, Hutchinson 42 described a choroid, “speckled with minute dots of yellowish white deposits”. He considered the spots to be “colloid excrescences of the lamina elastica” and wrote “There is no doubt that the disease is confined to the choroid in the first instance, while the great defect of sight which accompanies it points to implication of the retina secondarily.” He formulated the following three stages in the disease: (1) scattered yellow-white spots; (2) coalescence of these to patches with irregular borders; and (3) hemorrhage at the yellow spot and absorption of the blood. Essentially, his formulation had anticipated the present-day paradigm of the clinical course from drusen to late AMD. His first three cases dealt with a family, in which three sisters who had experienced the onset of disease at the ages of 40, 48, and 57 years. 42 He actually described Doyne's honeycomb retinal dystrophy, given the rather early age of onset and the fact that there were other cases of visual loss in the family. Hutchinson ended his account by mentioning that his friend Mr. Waren Tay “made the ophthalmoscopic examination, and drew my attention to the peculiarities presented”. In 1884, Nettleship 46 had already noticed central guttate choroiditis, with a plate that clearly showed drusen, so what we now would name early AMD (Fig. 3A). He also published in the same year on central senile areolar choroidal atrophy, now called dry late AMD (Fig. 3B). 47 Soon later, AMD was referred to as “Hutchinsonian changes of the posterior pole of the eye”. 48 Goldzieher reported on four eyes of unspecified age with drusen-shaped flecks around the macula and assumed that the changes were due to atheromatosis. Unlike Hutchinson, he did not consider these changes a choroidal disorder, or colloid excrescences of the vitreous membrane of the choroid, but compared them with cerebral leukomalacia caused by occlusions of the macular arterioles. In subsequent years, diagnoses such as chorioretinitis, 49 syphilis 50 and tumors 51 most likely were referring to AMD. Thus, the choroid gradually loses attention as the tissue where these diseases originate from and researchers focus on pathophysiological concepts such as atheromatosis, infections, and tumors.

Although Nettleship 47 had already mentioned central senile areolar choroidal atrophy, Haab 52 was the first to report one year later in 1885 on Senile Makulaerkrankung (senile macular illness), as a separate entity among the MDs, starting in the RPE (Fig. 1B). No other articles by Haab have come to light, explaining why he decided that senile macular illness was a separate entity. He concluded from analyzing over 50,000 patient files that this senile macular illness was about as frequent as traumatic ones and myopic macular affection. Senile illness was often bilateral, and one should be wary of the outcome of a mature cataract operation when the fellow eye had this illness. 53 It is striking that Haab explicitly stated that drusen, “quite innocent changes in old persons”, had nothing to do with senile macular illness (Fig. 1A). 54
An article in 1893 by Fuchs on circinate retinitis, a circle of white flecks around the fovea, 55 precipitated an avalanche of over 50 articles on this topic.56–58 Circinate degeneration 57 or senile exudative retinitis were proposed as more precise terms. 58 A review on 61 out of 129 eyes with disciform MD (dMD) having white spots showed that 36% had circinate retinitis. 17 In 1904, 30 years after Hutchinson's article, subretinal hemorrhages in AMD came again to the attention of researchers 59 and one year later, atherosclerosis was suggested as a possible cause. 60 Also fibrous plaques in the macular area of old persons, in conjunction with punctate yellowish dots, followed by hemorrhages, were drawn and described as senile exudative macular retinitis. 61
In the legend accompanying the image of the eye of a 79-year-old man from Oeller's 62 atlas (Fig. 4), the word disciform appears to have been used in 1896 for the first time. The first image of disciform macular disease (dMD) was probably image number 6 in Pagenstecher's atlas from 1875 called “choroido-retinitis in the region of the macula lutea” (Fig. 5). 49,63 One should not confuse this idea of a disk under the macular area with the clinical expression disciform reaction, introduced later, and meaning any development of a neovascular membrane under the macula, whatever its cause. The breakthrough in relation to disciform MD, however, was the classic monograph by Junius and his predecessor Kuhnt. 63 They described exhaustively 10 cases with an age range from 36 to 76 years, having a disciform process including five monocular ones, each with a good fellow eye. One case received a diagnosis illness of the retinal center, one case received degeneration of this center, and eight cases had both diagnoses. Junius and Kuhnt concluded that circinate retinitis and disciform disease of the retinal center belonged to one large cluster of diseases. Only Case I had increasing drusen-like spots along the inferior temporal venule, and the term druse or colloid body did not otherwise appear in any description of their cases. The word senile appeared once in Case II with senile vessel diseases. The causes suggested for the dMDs varied from alcoholism and lues to hypertension and atherosclerosis. This monograph is valuable for the following three reasons: first, the excellent overview of the past literature on dMD; second, the detailed color drawings; and, finally, it informed the wider public about dMD. 63 On page 132 of the epilog, they wrote: The expression disciform illness of the retinal center may appear somewhat bleak or dull. Would this be the reason that they changed the title of their monograph from Erkrankung (illness) to Entartung (degeneration) in order to attract attention? So what I always considered to be a monograph on end-stage AMD was actually a monograph on dMD caused by different retinal disorders, including a few cases with late AMD. Verhoeff and Duke-Elder added the word senile to the original title of this monograph of Junius and Kuhnt and started a sub-chapter with “Senile disciform degeneration of the macula (of Junius and Kuhnt)”. But in doing so, they incorrectly linked all the various causes of dMD with AMD.17,6 4 The limited knowledge of or interest in AMD around 1965 may be apparent from Duke-Elder's System of Ophthalmology. It covered AMD in seven pages in the chapter “Uveal manifestations of systemic diseases”, under the sub-head “Vascular sclerosis”, using the terms “Senile macular chorioretinal degeneration, Senile macular degeneration of Haab (Haab named it senile macular illness), or Senile macular degeneration”. 64 Drusen were dealt with in a few pages under the subcategory secondary degenerations. 65

Disciform macular degeneration. 70 male, 79 years old. Round center, over 2.5 diopter prominence.

According to Junius and Kuhnt, the first drawing of disciform macular disease as seen in the eye by low magnification after removal of the anterior segment. It was called Choroido-retinitis in the region of the macula lutea. “Between the papilla and macula lutea is a whitish tract which extends downwards, becoming whiter, and terminates in a sharp point.” this atlas was published in English and German. 49
Terminology over the Last Decades
The terminology of AMD showed fewer variations after 1965 (Table 3). Ophthalmologists gradually became aware that senile MD is not a diagnosis that patients are eager to hear, quite apart from its visual implications. Age-determined as a substitute for senile was first used in Germany 66 and later age-related appeared in the American literature. 67 Table 3 lists a gradual change after 1965 from senile maculopathy and age-related MD to age-related macular disease, ageing macula disease, aging macula disorder, and the latest term being autoimmune macular disorder. 68 All these terms share the common abbreviation AMD. The terms early and late AMD were coined around 1995. 69 Early AMD indicates that drusen with pigmentary changes in the macula are present in persons with the age of ≥50 years and usually it produces few visual symptoms. Late AMD is often associated with visual loss and is divided into dry late AMD, similar to geographic atrophy, and wet or neovascular AMD due to fluid leakage or hemorrhages from (new) blood vessels in the macular area.
We have achieved much since Donders, Nagel, Hutchinson, and Haab published their pioneering articles but still do not really know the cause of drusen or of AMD. I hope that this overview will place various historical concepts in proper perspective and stimulate young researchers to tie the loose ends still attached to AMD. This association was already described in 1875 42 and only 120 years later vascular endothelial growth factor became associated with AMD. 91
Author Contributions
P.T.V.M. de Jong collected and read all literature as given in the references, wrote the first and subsequent drafts of the manuscript, thus agrees with its contents and conclusions, made critical revisions, and approved of the final manuscript.
Footnotes
Acknowledgments
I am greatly indebted to P. G. Breen BA HDE, J. M. B. V. de Jong MD PhD, J. M. J. Dony MD PhD, G. Eisner MD PhD, B. P. Gloor MD PhD, J. Jonas MD PhD, J. E. E. Keunen MD PhD, H. R. Koch MD PhD, P. J. Koehler MD PhD, M. J. M. Koomen MD DPharm, P. Stoutenbeek MD, and Dr L. They for critically reviewing the text and/or help in obtaining or translating old manuscripts. Also to the Royal College of Ophthalmology, London UK, for permission to re-use ![]() and to Springer, Heidelberg, Germany, for permission to re-use the other figures. Part of this manuscript appeared in Historia Ophthalmologica Internationalis. This study was partly presented at the 28th meeting of the Julius Hirschberg Gesellschaft, Bonn, Germany, October 4, 2014, and partly at the joint Cogan– Hirschberg Society meeting, New York, USA, March 28, 2015. All references may be obtained from the author unless protected by copyright or library regulations.
and to Springer, Heidelberg, Germany, for permission to re-use the other figures. Part of this manuscript appeared in Historia Ophthalmologica Internationalis. This study was partly presented at the 28th meeting of the Julius Hirschberg Gesellschaft, Bonn, Germany, October 4, 2014, and partly at the joint Cogan– Hirschberg Society meeting, New York, USA, March 28, 2015. All references may be obtained from the author unless protected by copyright or library regulations.