
Abstract
Background
1,3-dimethylamylamine is a commonly used ingredient within dietary supplements. Our prior work with this agent indicates a transient increase in blood pressure (systolic in particular) following oral ingestion of a single dosage, but no significant increase in resting blood pressure following chronic ingestion. Moreover, intervention studies involving both two and eight weeks of treatment with finished products containing 1,3-dimethylamylamine indicate minimal or no change in bloodborne markers of health. The present study sought to extend these findings by using a 10 -week intervention trial to determine the change in selected markers of health in a sample of men.
Methods
25 healthy men were randomly assigned to either a placebo (n = 13) or to a supplement containing 1,3-dimethylamylamine (n = 12) for a period of 10 weeks. Before and after the intervention, resting blood pressure and heart rate were measured, and blood samples were collected for determination of complete blood count, metabolic panel, and lipid panel.
Results
No significant differences were noted between conditions for blood pressure (P > 0.05), although systolic blood pressure increased approximately 6 mmHg with the supplement (diastolic blood pressure decreased approximately 4 mmHg). A main effect for time was noted for heart rate (P = 0.016), with values decreasing from pre to post intervention. There were significant main effects for time for creatinine (increased from pre to post intervention; P = 0.043) and alkaline phosphatase (decreased from pre to post intervention; P = 0.009), with no condition differences noted (P > 0.05). There was a significant interaction noted for low density lipoprotein cholesterol (LDL-C) (P = 0.043), with values decreasing in the supplement group from pre to post intervention approximately 7 mg · dL-1 (P = 0.034). No other effects of significance were noted for bloodborne variables.
Conclusion
These data indicate that a dietary supplement containing 1,3-dimethylamylamine does not result in a statistically significant increase in resting heart rate or blood pressure (although systolic blood pressure is increased ~6 mmHg with supplement use). The supplement does not negatively impact bloodborne markers of health. Further study is needed involving a longer intervention period, a larger sample size, and additional measures of health and safety.
Background
While somewhat controversial, 1,3-dimethylamylamine has been suggested to be a component of the Pelargonium graveolens plant; 1 a simple aliphatic amine 2 with sympathomimetic properties. Aside from 1,3-dimethylamylamine, common chemical names cited for this agent include 2-amino-4-methylhexane, 1,3-dimethylpentylamine, methylhexaneamine, and 4-methyl-2-hexylamine. It is also known by the trade-marked name geranamine™ (Proviant Technologies, Inc, 2005: US trademark number: 78542697).
The use of 1,3-dimethylamylamine is widespread within the dietary supplement industry, in particular as a component of weight loss and pre-workout products. A recent report published by the Human Performance Resource Center (http://www.humanperformanceresourcecenter.org) provides a detailed listing of close to 100 products believed to contain 1,3-dimethylamylamine. While anecdotal reports of improved exercise performance are common, we are aware of only one published experiment designed to investigate the ergogenic properties of 1,3-dimethylamylamine alone or in combination with caffeine, 3 which noted little impact on aerobic exercise performance. Regardless of actual ergogenic effectiveness, the overall safety of the ingredient needs to be considered.
In our recent article in which 1,3-dimethylamylamine was administered alone and in combination with caffeine in a single dosage to healthy men and women, 4 we noted that heart rate was unaffected by treatment, but blood pressure was elevated when consuming 1,3-dimethylamylamine—generally in a dose-dependent manner. The peak percent change in systolic (~20%) and diastolic (~17%) blood pressure was noted at 60 minutes following ingestion of the combination of 250 mg of caffeine and 75 mg of 1,3-dimethylamylamine. A second study investigated the blood pressure and heart rate response of 1,3-dimethylamylamine and caffeine alone and in combination (compared to a placebo) in a sample of endurance trained men and women before, during, and following strenuous exercise. 3 In this study, heart rate was relatively similar across conditions, and blood pressure was generally highest for caffeine and 1,3-dimethylamylamine alone compared to other conditions.
Research on the use of 1,3-dimethylamylamine in combination with other ingredients within finished products demonstrated first that, in terms of acute changes in blood pressure and heart rate, dietary supplements containing 1,3-dimethylamylamine result in minimal change in heart rate but do increase systolic blood pressure transiently.5,6 Second, in terms of chronic changes in blood pressure and heart rate, we have noted little or no change in resting measures after a two-week 5 or eight-week 7 intervention. Third, in terms of chronic changes in bloodborne biomarkers of health and safety, we have noted little or no change in measures after a two-week 5 or eight-week 7 intervention.
Collectively, the above findings indicate relative safety of this ingredient, at least with regard to the included outcome measures. However, due to the transient increase in systolic blood pressure, the need exists to further evaluate the potential for this agent to raise resting blood pressure following a longer period of chronic intake. The present study sought to extend our prior findings related to the use of 1,3-dimethylamylamine in a combined product by using a 10 week intervention trial to determine the change in selected markers of health and safety in a sample of healthy men.
Methods
Subjects
Thirty resistance-trained men were recruited from the local university campus and surrounding community. Sample size was chosen based on studies of similar magnitude and scope; however a power analysis was not performed a priori. Subjects were self- reported non-smokers, and did not have cardiovascular or metabolic disease. Health history, drug and dietary supplement usage, and physical activity questionnaires were completed by subjects. Subjects were instructed to maintain their current exercise training and dietary intake programs throughout the study period with the exception of refraining from strenuous exercise during the 48 hours prior to each lab session. Subjects did not use dietary supplements, with the exception of meal replacements and protein powders, during the study period. The study was approved by the University of Memphis Committee for Human Subject Research.
Design
This study involved a randomized, placebo-controlled design. Although the study was also double-blinded, the stimulant effects of the supplement suggest that blinding from the subject standpoint is essentially lost. During the first visit to the laboratory, subjects provided written informed consent and completed health and physical activity questionnaires.
Lab protocol
Subjects reported to the lab in the morning hours following a minimum of an eight-hour overnight fast, before and after the 10-week intervention. Upon arrival to the lab, subjects rested quietly in a supine position for 10 minutes. Heart rate (via palpation) and blood pressure (via stethoscope) were then measured and recorded. A blood sample was then obtained from subjects (~20 mL). Blood was processed and sent to Laboratory Corporation of America for analysis of complete blood count, comprehensive metabolic panel, and lipid panel. The complete blood count was determined using an automated cell counter (Coulter LH750). The comprehensive metabolic panel was determined using automated procedures (Roche/Hitachi Modular). The lipid panel was determined using enzymatic procedures (Roche/Hitachi Modular). To better characterize subjects, body mass (using an electronic scale) and body composition (using dual energy x-ray absorptiometry) was measured. These same procedures were used both pre and post intervention for all subjects.
Physical activity and dietary intake
Subjects were asked to maintain their usual physical activity and dietary patterns and to record all food and drink consumed during the seven days prior to each lab session (both pre and post intervention). All records were analyzed for total calories, protein, carbohydrate, fat, vitamin C, vitamin E, and vitamin A (Food Processor SQL, version 9.9, ESHA Research, Salem, OR).
Conditions
The two conditions consisted of a placebo powder (microcrystalline cellulose, silicon dioxide, citric acid, natural flavor, acesulfame-K, sucralose, vegetable stearate, chlorophyll for coloring; at a volume equal to that of the supplement) and a dietary supplement containing a proprietary blend of 1,3-dimethylamylamine, caffeine, creatine monohydrate, β-alanine, schinzandrol A, and arginine alpha-ketoglutarate (Jack3d™, USPlabs, LLC. Dallas, TX). Subjects were instructed to consume 1-3 servings on each workout day, 30 minutes prior to their exercise session. The mean number of workout days per week for subjects was four and the supplement was not consumed on non exercise days. Subjects reported back to the laboratory as needed for receipt of an additional container of their assigned condition. Both the supplement and placebo powder were to be mixed into eight ounces of water and both had a similar lemon-lime taste. Subjects ingested the assigned condition for the duration of the 10 -week study period.
Statistical analysis
Data were analyzed using a 2 (condition) × 2 (time) factorial analysis of variance (ANOVA) with use of Fisher's LSD. Data are presented as mean ± standard deviation. All analyses were performed using PASW statistical software (version 18). Statistical significance was set at P ≤ 0.05. Standardized effect sizes (ES) were calculated for means comparisons. 8 Effect size magnitudes can be interpreted as follows: 0.2 small, 0.6 moderate, and 1.2 large.
Results
Although 30 subjects began the study, only 25 subjects successfully completed all lab sessions. Of the five subjects who failed to complete the study, two were initially assigned to the placebo and three were initially assigned to the supplement. One subject in the supplement group was injured while training and was unable to complete the intervention, and thus was excluded from analysis. The remaining four subjects failed to complete all testing due to personal reasons. These five subjects are not included in the analyses. Additionally, two subjects in the placebo group were unable to provide blood samples pre- and post intervention and are thus excluded from the bloodborne variable analysis. No subjects reported adverse events attributable to the supplement or placebo.
Of the 25 subjects in the analysis, self reported use data of subjects indicate that the mean number of scoops of the supplement consumed on training days was 2.4 ± 0.3 (2 subjects = 3 scoops; 7 subjects = 2 scoops; 3 subjects = 1.5 scoops), which was greater than (P = 0.0003) the mean number of scoops of the placebo consumed (1.7 ± 0.4; 7 subjects = 2 scoops; 3 subjects = 1.5 scoops; 3 subjects = 1 scoops). Subject characteristics are presented in Table 1.
Characteristics of men assigned to supplement (N = 12) or placebo (N = 13) for ten weeks.

Significant main effect for time (P < 0.05).
Blood pressure and heart rate data
No significant differences were noted between conditions for blood pressure (P > 0.05). However, systolic blood pressure increased approximately 6 mmHg with the supplement, while diastolic blood pressure decreased approximately 4 mmHg from pre to post intervention. A main effect for time was noted for heart rate (P = 0.016, ES = 1.1), with values decreasing from pre to post intervention. No other findings were of statistical significance (P > 0.05). Blood pressure and heart rate data are presented in Table 1.
Bloodborne data
There were significant main effects for time for creatinine (increased from pre to post intervention; P = 0.043, ES = 1.1) and alkaline phosphatase (decreased from pre to post intervention; P = 0.009, ES = 0.5), with no condition differences noted (P > 0.05). There was a significant interaction noted for low density lipoprotein cholesterol (LDL-C) (P = 0.043), with values decreasing in the supplement group from pre to post intervention approximately 7 mg · dL-1 (P = 0.034, ES = 0.9). No other effects of statistical significance were noted for bloodborne variables. Data are presented in Table 2 for complete blood count, Table 3 for metabolic panel, and Table 4 for lipid panel.
Complete blood count data for men assigned to supplement (N = 12) or placebo (N = 11) for ten weeks.

Comprehensive metabolic panel data for men assigned to supplement (N = 12) or placebo (N = 11) for ten weeks.

Significant main effect for time (P < 0.05).
Lipid panel data for men assigned to supplement (N = 12) or placebo (N = 11) for ten weeks.
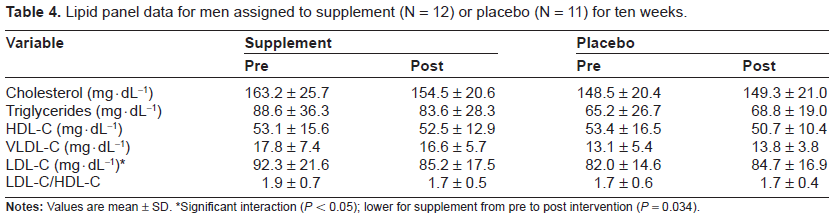
Significant interaction (P < 0.05); lower for supplement from pre to post intervention (P = 0.034).
Dietary data
There was a significant main effect for time for dietary fiber (P = 0.018, ES = 0.8), which decreased from pre to post intervention. A main effect for time was also noted for dietary selenium (P = 0.032, ES = 0.8), which increased from pre to post intervention. Dietary data are presented in Table 5.
Dietary intake for men assigned to supplement (N = 12) or placebo (N = 13) for ten weeks.

Significant main effect for time (P < 0.05).
Discussion
Our data indicate that a dietary supplement containing 1,3-dimethylamylamine does not significantly increase resting heart rate or blood pressure (although systolic blood pressure increased ~6 mmHg with the supplement). Moreover, the supplement does not adversely impact bloodborne biomarkers of health, but rather, results in a decrease in LDL-C. These findings are in reference to a small sample of healthy men who exercise regularly. Due to the fact that our sample size is small, additional well-designed experiments of similar scope, inclusive of larger sample sizes, are needed to extend the findings presented within. It is only through such work that our ability to generalize these findings to the population at large will be possible.
These data extend our prior work using 1,3-dimethylamylamine in combination with other ingredients, including those considered to be stimulants.5,7 Collectively, these data provide some support for the relative safety of this agent; at least with regards to the measured outcomes used in this study, as well as others which we have conducted. Despite this, more work is needed involving a longer intervention period and the inclusion of additional measures of health (eg, toxicology, cardiac function), to more fully elucidate the safety of oral 1,3-dimethylamylamine ingestion. Additionally, since products containing 1,3-dimethylamylamine are marketing not only to men but also to women, more work using a larger sample of women may be considered.
The majority of subjects in the present study consumed the supplement at a dosage of two scoops per training day. No adverse events were noted and the supplement was well-tolerated based on subject self report. This agrees with our prior work with this same supplement, in which all subjects successfully completed a two-week intervention period, without incident, in which two-scoops of the supplement were consumed daily. 5
As can be viewed in Table 1, systolic blood pressure increased approximately 6 mmHg with the supplement, while diastolic blood pressure decreased approximately 4 mmHg from pre to post intervention. Neither change was of statistical significance. Heart rate was lower from pre to post intervention, which would subsequently impact the rate pressure product (systolic blood pressure × heart rate). That is, when calculating the rate pressure product values at pre (7245) and post (7265) intervention (using the mean data provided in Table 1), it is noted that values are near identical. This may be of interest to those with concern over the increase in systolic blood pressure and the potential for increased myocardial stress.
Findings of minimal change in heart rate and blood pressure (and hence, rate pressure product) have been noted in our two-week intervention using the same supplement. 5 Little change in blood pressure was noted in our eight week intervention using another supplement containing 1,3-dimethylamylamine, 7 while an increase of ~6 bpm in resting heart rate have been noted. Interestingly, in our two-week intervention using another supplement containing 1,3-dimethylamylamine, 5 resting heart rate was decreased by ~4 bpm. More work is needed to better understand the role of 1,3-dimethylamylamine in relation to hemodynamic variables.
Related to bloodborne variables, we included the routine panels as used as part of a physical examination (ie, complete blood count, metabolic panel, lipid panel). No adverse effects were noted for any measured variable, including those related to liver function (eg, SGOT, SGPT, GGT). Variables were very similar from pre to post intervention for the supplement group. Creatinine was noted to be higher from pre to post intervention, in particular for the supplement group (Table 3). This small increase may have been due to the inclusion of creatine within the dietary supplement. The measures of triglycerides, total and LDL cholesterol decreased slightly from pre to post intervention, with statistically significant findings noted only for LDL-C (Table 4). As with blood pressure and heart rate, these bloodborne data extend our prior work involving a two-week intervention study using the same supplement 5 (with the exception of an increase in fasting blood glucose noted in our prior work), as well as in our eight week intervention study using a different supplement containing 1,3-dimethylamylamine. 7
Conclusion
Findings from the present study indicate that a dietary supplement containing 1,3-dimethylamylamine consumed for a period of 10 weeks does not result in a statistically significant increase in resting heart rate or blood pressure in a sample of healthy men, nor does the supplement negatively impact bloodborne biomarkers of health. The supplement results in a small decrease in LDL-C, which may suggest a potential cardioprotective role. While this may have clinical relevance, additional studies inclusive of larger samples are needed to replicate these findings, as well as to extend and expand upon other findings associated with this work. In particular, longer intervention periods and the inclusion of additional measures of health and toxicity are needed in future studies involving 1,3-dimethylamylamine. Finally, it should be noted that despite our lack of statistical significance, the supplement did result in a mean increase in systolic blood pressure of ~6 mmHg, indicating that it would be prudent for those with elevated blood pressure to avoid use of dietary supplements containing 1,3-dimethylamylamine.
Competing Interests
RJB has received research funding or acted as consultant to nutraceutical and dietary supplement companies. All other authors declare no competing interests.
Author Contributions
PNW, BKS, and TMF were responsible for data collection/entry/analysis and assistance with manuscript preparation. RJB was responsible for the study design and preparation of the manuscript. All authors read and approved the final manuscript.
Disclosures
Author(s) have provided signed confirmations to the publisher of their compliance with all applicable legal and ethical obligations in respect to declaration of conflicts of interest, funding, authorship and contributorship, and compliance with ethical requirements in respect to treatment of human and animal test subjects. If this article contains identifiable human subject(s) author(s) were required to supply signed patient consent prior to publication. Author(s) have confirmed that the published article is unique and not under consideration nor published by any other publication and that they have consent to reproduce any copyrighted material. The peer reviewers declared no conflicts of interest.
Footnotes
Acknowledgement
Funding for this work was provided by USPlabs, LLC.