
Abstract
Background
The purpose of this study was to investigate the acute effects of a nutritional supplement containing a proprietary blend of Phellodendron and Crape Myrtle on serum glucose and insulin in response to a modified oral glucose tolerance test (OGTT).
Methods
Using a randomized, double-blind, cross-over design, 10 exercise-trained, non-diabetic men reported to the lab in a 10 hour fasted state, on two different mornings separated by 1-2 weeks, and were subjected to an OGTT by ingesting a 75 gram dextrose solution. Fifteen minutes prior to the OGTT subjects ingested either a dietary supplement containing a blend of Phellodendron and Crape Myrtle (SUPP) or a placebo (PLA). Blood samples were collected before ingestion of the SUPP or PLA and at 15, 30, 45, 60, and 75 minutes postingestion of the dextrose load. Samples were analyzed for serum glucose and insulin.
Results
In relation to serum glucose, a condition effect was noted (P = 0.01), with values lower for SUPP compared to PLA. In relation to serum insulin, a trend for a condition effect was noted (P = 0.06), with values lower for SUPP compared to PLA.
Conclusion
These findings indicate that acute ingestion of a dietary supplement containing a blend of Phellodendron and Crape Myrtle can lower the serum glucose response to a modified OGTT, while resulting in a non-significant attenuation in insulin response. These data are specific to a small sample of exercise-trained, non-diabetic men.
Background
Approximately 25.8 million Americans (8.3% of the population) are currently living with diagnosed (18.8 million) or undiagnosed (7.0 million) diabetes. 1 An additional 79 million Americans are estimated to have pre-diabetes—evidenced by a hemoglobin A1c value of 5.7%-6.4% and/or fasting blood glucose of 100-125 mg • dL-1; an alternative criteria includes a 2-hour post oral glucose tolerance test (OGTT) blood glucose of 140-199 mg • dL-1. 1 Unfortunately, the overall prevalence of these conditions continues to rise, as indicated by the 1.9 million newly diagnosed cases of diabetes in 2010, within people aged 20 years and older. 1 Indeed, a need exists to aid the millions of individuals with blood glucose management issues.
Methods to control blood glucose through the use of exercise, 2 dietary manipulation, 3 pharmacologic agents, 4 and nutritional supplements 5 have all been investigated with varying degree of success. While the combination of “alternative medicine” approaches including regular physical exercise and the consumption of a nutrient dense diet is arguably the best approach aimed at managing blood glucose levels, the use of selected nutritional supplements may also be considered as an adjunct to this plan. In particular, several plant based nutrients have been studies in recent years with mixed success.6–8 Although most studies have been conducted using animal models, or with use of in vitro approaches, data for selected nutrients have shown promise, with multiple mechanisms of effect being identified.9–13
Two plant based nutrients that appear to have efficacy are Phellodendron and Crape Myrtle. Phellodendron contains the active ingredient berberine, which has been shown to regulate glucose and lipid metabolism in vitro and in vivo, with multiple proposed metabolic effects.10,11,14–17 Crape Myrtle, or more specifically banaba (Lagerstroemia speciosa L.), contains corosolic acid, which also has been reported to possess multiple in vitro and in vivo metabolic effects related to blood glucose management.9,18–21 To our knowledge, only two human studies have been performed to investigate the blood glucose lowering effects of corosolic acid, within a mixed sample of diabetic and non-diabetic subjects 21 and type 2 diabetics. 22
Recently, a nutritional supplement containing a proprietary blend of Phellodendron and Crape Myrtle (Anabolic Pump™) has been developed. It is postulated that this product may aid in the management of blood glucose and allow for increased glucose clearance following an OGTT. The present study sought to investigate the acute effects of this nutritional supplement on serum glucose and insulin in response to a modified OGTT.
Methods
Subjects
Ten healthy, exercise-trained men were recruited from the University of Memphis Campus and surrounding community and completed all aspects of this study. Subjects were not smokers and did not have diagnosed cardiovascular or metabolic disease (including diabetes). One subject reported using a daily aspirin (325 mg) and one subject used an anti-depressant (Sertraline). No other subject reported the use of prescription medications. Subjects were not using dietary supplements believed to influence blood glucose disposal—but were allowed to continue their routine use of a daily multi-vitamin/multi-mineral supplement and/or a daily protein/meal replacement powder. Subjects were instructed not to alter their current supplementation schedule over the course of the study period. In addition, subjects were instructed to maintain their current physical activity and dietary intake programs throughout the study. However, they were instructed to refrain from strenuous exercise during the 24 hours prior to each test session, as this may have influenced their response to the modified OGTT. Health history, drug and dietary supplement usage, and physical activity questionnaires were completed by subjects to determine eligibility. Subject characteristics are presented in Table 1. The study was approved by University of Memphis Institutional Review Board and all subjects provided written consent.
Characteristics of 10 men.

As this was a pilot study, we did not conduct a power analysis to determine the optimal sample size necessary to observe a given effect in our outcome measures. It was our objective in this initial study to generate data to determine the general pattern of response in blood glucose and insulin following use of the supplement. These data could then be used for planning potential larger future studies related to the tested supplement. Our small sample size, although consistent with studies of this nature, as well as our failure to include a power analysis, is a limitation of this work.
Screening
During the initial visit to the laboratory, subjects completed the informed consent form, health and physical activity questionnaires. Subjects’ heart rate and blood pressure, height, weight, waist and hip circumference, skinfold thickness (7-site test using Lange calipers and the Siri equation for estimating body fat percentage) were measured and used for descriptive purposes. Subjects were provided with food logs and instructions regarding how to complete these logs during the day prior to each test day.
Testing
Subjects reported to the laboratory in the morning hours (6:00-8:00 am) following a 10 hour overnight fast. During the two visits subjects consumed in random order, separated by 1-2 weeks, either a placebo (microcrystalline cellulose) or a nutritional supplement (proprietary blend of 750 mg of Phellodendron [bark] and Crape Myrtle [Lagerstroemia Speciosia] stem [Anabolic Pump™ USPlabs, LLC, Dallas, TX]). The formulation dosage of 750 mg was based on prior studies using Phellodendron and Crape Myrtle in isolation,21–23 while our decision to use the standard single capsule 750 mg dosage was based on our intention to determine the practical application of the finished product when used at the recommended dosage. Although using a dosage greater than 750 mg may have provided greater effects, we would not have truly tested the efficacy of the supplement when taken as suggested by the manufacturer. The supplement was produced using a proprietary process involving a series of solvent-based extraction and chromatographic techniques, to produce highly purified active components of Phellodendron and Crape Myrtle. Both Phellodendron24,25 and Crape Myrtle 21 are thought to be safe and non-toxic.
Subjects consumed the conditions in capsule form. Fifteen minutes following the ingestion of the assigned condition, a modified OGTT was administered. This consisted of 75 grams of 100% pure dextrose powder (NOW Foods, Bloomingdale, IL) mixed into 12 ounces of water. Subjects consumed the entire solution within two minutes. While we do not have data pertaining to the optimal time period in which the supplement should be ingested prior to the OGTT, our timing was similar to and based on the prior work of Fukushima and coworkers who tested the glucose lowering effects of corosolic acid in a mixed sample of diabetic and non-diabetic subjects. 21 It is possible that ingestion of the supplement at times closer to or further from the ingestion of the dextrose solution may yield differing results as compared to those presented here.
Blood samples were taken before the ingestion of the assigned condition (following a 10 minute quiet rest period) and at 15, 30, 45, 60 and 75 minutes following ingestion of the dextrose load. It should be noted that while standard procedures for an OGTT include sampling every 30 minutes for a period of 2-3 hours, 26 we have noted that when using healthy non-diabetic men as test subjects, such a time course is not optimal. That is, serum glucose values after ingestion of a 75 gram dextrose load are close to baseline values within one hour post-ingestion and remain close to this level (or lower than this level) for the following two hours. 27 While it is possible that differing results may have been observed with the present group of subjects, in particular when ingesting a supplement designed to lower blood glucose, we did not choose to continue measurement beyond 75 minutes post ingestion of the dextrose load. Our failure to do so may be considered a limitation of this work. Related to this, it should be understood that the methods employed in the present study are different than those of a standard OGTT, and therefore our findings may not be directly compared to those obtained using the traditional timing schedule (ie, every 30 minutes for a period of 2-3 hours). 26
Prior to each blood draw, heart rate (via 60 second palpation) and blood pressure (via auscultation) were taken. Although not a primary outcome, our rationale for obtaining these measures was based on the observation that a postprandial rise in serum glucose is associated with an increase in reactive oxygen species (ROS) production,28,29 which is known to induce an acute state of endothelial dysfunction.29,30 This potential rise in ROS may lead to vascular dysfunction and elevated blood pressure. We hypothesized that if the supplement was effective at significantly lowering the serum glucose response to the OGTT, it may have affected the postprandial blood pressure response.
No food or calorie containing beverages were allowed during the test period, although water was allowed ad libitum and matched for each subject during both days of testing. These exact procedures were followed for both test days.
Blood processing and biochemistry
At each time of blood collection, venous samples were taken from subjects via needle and Vacutainer®. Following collection, blood samples were processed accordingly and immediately stored at −70 °C until analyzed. Glucose was determined in serum using standard enzymatic procedures as described by the reagent manufacturer (Thermo Fisher Scientific; Waltham, MA). Glucose assays were performed in triplicate. Insulin was determined in serum using a solid phase enzyme linked immunosorbent assay (ELISA) kit following the instructions of the manufacturer (Calbiotech; Spring Valley, CA). Insulin assays were performed in duplicate.
Physical activity and dietary intake
Subjects were asked to refrain from strenuous physical activity during the 24 hours before test days. Subjects were asked to record all food and drink consumed during the 24 hours prior to each test day. Upon receipt of the first 24 hour diet record, subjects received a copy and were asked to duplicate this intake during the 24 hour period immediately prior to the subsequent test day. All records were analyzed for total calories, protein, carbohydrate, fat, vitamin C, vitamin E, and vitamin A (Food Processor SQL, version 9.9, ESHA Research, Salem, OR).
Statistical analysis
Outcome variables were analyzed using a 2 (condition) × 6 (time) repeated measured analysis of variance (RMANOVA). Tukey post hoc testing was performed as necessary. The area under the curve (AUC) was calculated for glucose and insulin using the trapezoidal method as described in detail by Pruessner et al. 31 Data are presented as mean ± standard error of the mean. Subject descriptive characteristics are presented as mean ± standard deviation. All analyses were performed using JMP statistical software (version 4.0.3, SAS Institute, Cary, NC). Statistical significance was set at P ≤ 0.05.
Results
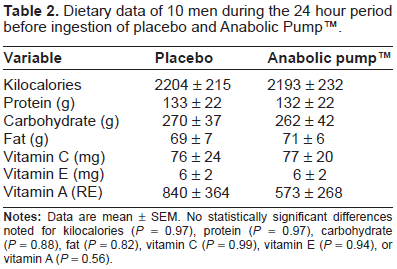
All subjects successfully completed both test sessions. Regarding dietary data, no differences of statistical significance were noted between conditions for any measured variable (P > 0.05), with typical values noted for all variables. The largest difference between conditions was noted in vitamin A, which is mainly attributed to an almost 5-fold increase in vitamin A intake for one subject during the day prior to ingesting the placebo as compared to the supplement (3030 RE vs. 614 RE). Dietary data are presented in Table 2. Regarding hemodynamic data, no interactions or main effects were noted for heart rate, blood pressure, or rate pressure product (P > 0.05). Data are presented in Table 3.
Dietary data of 10 men during the 24 hour period before ingestion of placebo and Anabolic Pump™.
Heart Rate (HR), Systolic Blood Pressure (SBP), Diastolic Blood Pressure (DBP), and Rate Pressure Product (RPP) before and following ingestion of placebo and Anabolic Pump™.

Biochemical measures
For serum glucose, a condition effect was noted (P = 0.01), with values lower for supplement compared to placebo. A time effect was also noted (P < 0.0001), with values at the 15 and 30 minute collection times higher than pre-ingestion (P < 0.05). No condition × time effect (P = 0.69) or AUC effect (P = 0.23) was noted. However, the supplement resulted in a 9.9% reduction in glucose AUC compared to placebo. Glucose data are presented in Figure 1.

Serum glucose before and following ingestion of placebo and Anabolic Pump™.
For serum insulin, the condition effect failed to reach statistical significance (P = 0.06); however values were generally lower for supplement compared to placebo. As with serum glucose, a time effect was noted (P < 0.0001), with values at the 15, 30, 45, and 60 minute collection times higher than pre-ingestion (P < 0.05). No condition × time effect (P = 0.95) or AUC effect (P = 0.29) was noted. However, a 33.3% reduction in insulin AUC was noted with the supplement compared to the placebo. Insulin data are presented in Figure 2.

Serum insulin before and following ingestion of placebo and Anabolic Pump™.
Discussion
We report that acute ingestion of a dietary supplement containing a proprietary blend of the plant-based ingredients Phellodendron and Crape Myrtle can lower the serum glucose response to a modified OGTT in a sample of young, healthy, exercise-trained, non-diabetic men. This response is observed along with a slightly attenuated insulin response to the OGTT when subjects ingest the supplement, as compared to placebo. While the condition effect for insulin failed to reach statistical significance (P = 0.06), a post-hoc power analysis indicated that a sample size of 12 subjects would be adequate to yield statistically significant findings.
Although our data are specific to a small sample of exercise-trained men, they support the notion that this blend of plants may improve glucose disposal while reducing the level of insulin required for such activity. These data provide rationale for continued study with this dietary supplement, in particular within a sample of individuals with impaired glucose tolerance, as more robust findings may be noted within such a population. Of course, the optimal timing of supplementation, as well as the dosage needed to provide for a measureable effect, first needs to be determined. Although the present study simply provided a single serving of the supplement 15 minutes prior to the OGTT (a timing similar to that used by many diabetic patients taking oral hypoglycemic agents prior to feeding), it is unknown whether or not chronic use of the supplement would yield stronger findings. Additional study is needed to generate an answer to this question.
Phellodendron, or more specifically the dried bark from this plant, is rich in the active ingredient berberine. Berberine is known to regulate glucose and lipid metabolism in vitro and in vivo, with multiple proposed metabolic effects. Specifically, berberine has been reported to mimic insulin activity in mouse models by increasing glucose uptake in adipocytes and myocytes, reducing phosphatase activity of tyrosine, and increasing receptor-mediated phosphorylation of insulin receptor substrates (IRSs). 11 In vitro, insulin messenger RNA and protein expression have been noted to increase in a variety of human cell lines after being treated with berberine.14,16 Berberine has also been shown to increase glucagon secretion while increasing insulin levels and beta-cells in the pancreas in rat models. 15 It has been suggested that berberine may increase GLUT1 activity, adenosine monophosphate–activated protein kinase, and acetyl-coenzyme A carboxylase phosphorylation. 10 The up-regulation of hepatocyte nuclear factor 4alpha (HNF4a) and hepatic glucokinase activity have also been suggested to play a role in enhanced glucose metabolism through the treatment of berberine. 17
The effects of Phellodendron may be complemented by Crape Myrtle. Much like Phellodendron, Crape Myrtle is believed to contain certain active ingredients within the leaves that have anti-diabetic properties. Specifically, banaba (Lagerstroemia speciosa L.) is a variety of Crape Myrtle that grows in certain parts of the world (eg, Philippines, India, Malaysia, Australia) and contains corosolic acid, for which increased interest exists in relation to its potential role in treating type 2 diabetes. Multiple metabolic effects have been reported for corosolic acid, including stimulated glucose uptake with a similar induction time and a dose-dependent response to that of insulin in adipocytes in vitro. 9 In type 2 diabetic mouse models, orally administered corosolic acid significantly increased the translocation of GLUT4 in muscle. 19 With regards to hepatic glucose metabolism, corosolic acid has been shown to inhibit gluconeogenesis via increased production of Fructose-2, 6-Bisphosphate, lowering cAMP levels, and inhibiting cAMP-dependent protein kinase; and possibly promote glycolysis via increased glucokinase activity independent of glucose-6-phosphate activity. 20 Also, in cultured cells, corosolic acid has been noted to induce insulin receptor phosphorylation by increasing the level of tyrosine phosphorylation of insulin receptor β. 32
While the potential impact of Phellodendron and Crape Myrtle is significant, with many overlapping effects on various aspects of glucose disposal, the molecular mechanisms related to any synergistic effect of these two plant-based ingredients remains to be determined. Future in vitro work using Phellodendron and Crape Myrtle, in isolation and in combination, may provide such mechanistic data.
Human studies using berberine have reported promising results. For example, Yin et al noted similar effects with berberine as compared to the anti-diabetic drug metformin. 23 Additionally, Zhang and colleagues 24 concluded that “Berberine is effective and safe in the treatment of type 2 diabetes.” Fasting plasma glucose concentrations have been noted to decrease in type 2 diabetic subjects when 0.3-0.5 g of berberine was ingested three times daily in three different investigations conducted in China.33–35 Taken together, these findings suggest a potential role for this agent in the management of blood glucose.
Human studies using corosolic acid have reported potential anti-diabetic effects, 21 which may be dose dependent. 22 For example, Fukushima and colleagues reported a lowering of blood glucose in response to an OGTT in a mixed sample of diabetics and those with impaired glucose tolerance, impaired fasting glucose, and normal glucose tolerance. 21 It is unknown how exactly our results compare to those of Fukushima et al, 21 as we used an OGTT with a modified blood sampling time period. Moreover, considering the dose-dependent nature of corosolic acid, 22 it is possible that our findings may have been stronger if we would have treated subjects with a higher dosage of the supplement. Future studies may consider different dosing patterns of this blend, possibly based on body mass, in order to more fully elucidate the potential role of this supplement on glucose disposal.
Although not a main outcome in the present study, we measured hemodynamic variables pre and post the modified OGTT. No differences were noted between conditions or across time for any measured variable. We hypothesized that a significant reduction in blood glucose following supplement intake may be associated with a reduction in blood pressure. This was based on the observation that a postprandial rise in blood glucose has been noted to be associated with an increase in ROS production,28,29 which correlated to acute endothelial dysfunction29,30—possibly involving elevated blood pressure. Although we failed to note statistical significant in our postprandial hemodynamic measures, values for blood pressure and rate pressure product were slightly lower for supplement compared to placebo (Table 3). It is possible that our small sample size and the use of healthy, non-diabetic men may have impaired our ability to detect more robust findings. Further investigation is needed, with the inclusion of a larger sample size, in order to extend these findings.
Conclusion
We conclude that when compared to a placebo, a finished dietary supplement containing a blend of Phellodendron and Crape Myrtle can lower the serum glucose response to a modified OGTT, while resulting in a non-significant (P = 0.06) attenuation in insulin response. Data from this initial study are specific to a small sample of young, healthy, exercise-trained, non-diabetic men. Future investigations may consider the inclusion of diabetic men and women of varying age, as well as the study of different dosing patterns of each ingredient, as such work may provide information as to the potential therapeutic role of this plant-based combination.
Competing Interests
Financial support for this work was provided in part by USPlabs, LLC. None of the authors have a financial interest in this company. RJB has received research funding or acted as consultant to nutraceutical and dietary supplement companies. All other authors declare no competing interests.
Author Contributions
REC, TMF, and CGM were responsible for data collection/entry and assistance with manuscript preparation. RJB was responsible for the study design, overseeing data collection, biochemical work, statistical analysis, and preparation of the manuscript.
Disclosures
Author(s) have provided signed confirmations to the publisher of their compliance with all applicable legal and ethical obligations in respect to declaration of conflicts of interest, funding, authorship and contributorship, and compliance with ethical requirements in respect to treatment of human and animal test subjects. If this article contains identifiable human subject(s) author(s) were required to supply signed patient consent prior to publication. Author(s) have confirmed that the published article is unique and not under consideration nor published by any other publication and that they have consent to reproduce any copyrighted material. The peer reviewers declared no conflicts of interest.
Footnotes
Acknowledgements
Funding for this work was provided by USPlabs, LLC and The University of Memphis. Trial Registration: ACTRN12610000928011.