
Abstract
In the United States, approximately 5% of the population is malnourished or has low body weight, which can adversely affect immune function. Malnutrition is more prevalent in older adults and is often a result of energy imbalance from various causes. Dietary supplementation to promote positive energy balance can reverse malnutrition, but has not been assessed for its effect on immune parameters. This 8-week clinical feeding trial evaluated the effect of a commercially available, high-protein, high-energy formula on body weight and immune parameters in 30 adult volunteers with body-mass indices (BMI) <21 kg/m2. After the intervention, participants gained a mean of 3.74 lbs and increased BMI by 0.58 kg/m2. The intervention improved lean body mass and limited body fat accumulation. However, no clinically significant improvements in immune measures were observed. These results support the use of high-protein, high-energy supplements in the treatment of underweight/malnutrition. Further investigation utilizing feeding studies of longer duration, and/or studying severely malnourished individuals may be needed to detect an effect on immune parameters of weight gain promoted by nutritional supplements.
Introduction
Malnutrition, often defined as a body mass index (BMI) of <18.5 kg/m2, is a worldwide public health problem. Unlike nutrient losses due to chronic diseases, such as the Human Immunodeficiency Virus Wasting Syndrome, 1 most often low body weight is the result of a simple imbalance between energy intake from food and energy expended. 2 This phenomenon is seen with greater frequency among older adults, who may suffer from poor dentition, poor appetite, inattention to feeding, or poor mobility as a concomitant of declining cognitive function and/or depression, which may, in part, be attributed to physiologic changes with age.3,4
While the prevalence of underweight is much higher in Asia than most developed countries and Africa, 5 in the United States, approximately 5% of the adult population has BMI below 21 kg/m2. Most individuals who are malnourished or have low relative body weights (BMI < 21 kg/m2) can normalize weight by increasing energy intake through a variety of methods, including dietary supplements or appetite-stimulating medications. 6 The most effective treatment provides a positive energy balance for both total calories and for protein. 7 In the absence of adequate protein levels in the diet, weight gain will tend to increase fat stores rather than increase a combination of adipose and lean tissue.8,9 While malnutrition is known to have dramatic effects on immune function and susceptibility to infectious and other diseases, little is known regarding improvements in immune status upon weight gain or correction of malnutrition.
The current study aimed at investigating the effect supplementation with a high-energy and high-protein, commercially-available formula (Quaker Complete Nutrition, Standard Foods, Taiwan) in malnourished adults and those with a BMI below 21 kg/m2. After 8 weeks of supplementation, we assessed weight and BMI changes, body composition, as well as immune markers and biochemical measures.
Methods
The study protocol was approved by the Johns Hopkins Bloomberg School of Public Health Institutional Review Board, and written informed consent was obtained from all eligible participants prior to participation.
Recruitment and eligibility
Potential participants were recruited from the Baltimore-Washington metropolitan area via newspaper and other advertisements and flyers which were placed around the Johns Hopkins medical campus. Participants were screened initially via telephone and subsequently at the clinic. Originally, participants were defined as eligible if they had a BMI < 18.5 kg/m2. Because of the rarity of extremely low BMIs in our population in the absence of exclusionary factors, such as terminal illness, the BMI cut-point was subsequently increased to <21 kg/m2 Participants were excluded if they were pregnant or nursing, had a food allergy, disliked the taste of vanilla, had a chronic disease such as HIV/AIDS or cancer that might account for their low BMI, or if they were unwilling to have their blood drawn or to gain weight. Participants were paid $10 for each visit, provided reimbursement for parking expenses, and received a $100 completion bonus.
Testing protocol
This was a pre-post supplementation clinical intervention study that included oral supplementation of the diet with 3-6 Quaker Complete Nutritional Shakes daily for 8 weeks. Data collected included height, body weight (BW), mid-arm circumference (MAC), mid-arm muscle circumference (MAMC), and triceps skin fold thickness measurements obtained by a trained technician at baseline (week 0), week 4, and follow-up (week 8) conducted according to ACSM guidelines for Exercise Testing and Prescription. Blood was collected at baseline (week 0) and follow up (week 8) for chemistries and immune function testing. Body composition was assessed via bioimpedence at week 0, week 4, and week 8. Participants were asked to return at weeks 1, 2, 4, 6 and 8 for weighing, completion of questionnaires regarding their diet, including a visual analog scale for assessing degree of hunger and satiety, and resupply with dietary supplements. Further dietary advice was also given; if participants wished/needed to continue efforts to gain weight, referral to a dietitian or medical clinic was made, if desired, in the final week (week 8) of the study.
Anthropometric and body composition measures
Height, body weight, MAC and MAMC measurements were obtained after overnight fasting with participants wearing lightweight clothing and no shoes. Weight and height were measured using a balance beam scale with a stadiometer (Seca, Hanover, MD). MAC and MAMC were measured thrice to the nearest 0.5 cm and averaged. Total body composition was measured using bioimpedance (BIA) testing. BIA is a method of determining fat-free mass and percent body fat that entails measuring conductivity of a very small, painless electric current administered briefly via electrodes taped to the hands and feet.
Blood collection and analyses
Blood samples were collected after an overnight fast (3 tubes, <15 ml total) at baseline and at the end of the 8-week intervention. Blood was drawn from the antecubital vein into a Vacutainer tube. Serum was allowed to clot for 15 minutes and then centrifuged at 2000
Immunological methods
Flow cytometry for the analysis of T-cell subsets and expression of activation markers was conducted according to standard methods. Within 24 hours of phlebotomy, fresh whole blood was incubated with appropriate directly conjugated monoclonal antibodies, as indicated in the Results section, with up to 4 antibodies conjugated to different fluorochromes used in the same staining tube. Red cells were then lysed with Becton-Dickinson lysing solution. Finally, the stained cells were fixed with 1% formaldehyde and analyzed on a Beckman Coulter XL flow cytometer capable of up to 4-color analysis.
Other immunological tests, including the complete blood count and differential and measurement of serum immunological markers were performed by commercial laboratories.
Intervention
Participants were instructed on how to use the Quaker dietary supplements (vanilla-flavored liquids of 250 kcal per 250 mL can), with the goal of incorporating 3-6 cans per day into their diet as snacks and/or meal supplements, thus potentially increasing energy intake by 750-1500 kcal/day. The number of cans recommended per day was based on subject eating habits (i.e. based on the number of meals and snacks that the subject consumed and the number of supplements of one-glass-size the subjects reported believing they could consume in addition to their usual diet).
Data analysis
Paired T-tests were used to analyze statistical significance. Significance was defined as
Results
Subjects
Fifty five men and women aged 21 years or older were screened and 45 were found to be eligible to participate. Of those eligible, 55.6% were African American, 26.7% were Asian/Unknown and 17.8% were Caucasian. The age ranged from 21-77 yrs (mean = 38.9 ± 15) and mean weight was 118.9 ± 19.2 lbs. Mean BMI was 18.2 kg/m2. Thirty participants (67%) completed the intervention. Table 1 describes study population demographics. Participants who dropped out of the study before 8 weeks were slightly younger on average compared to completers but had a similar mean baseline BMI.
Demographic characteristics of study population.

Information in parentheses is percentage of observed population.
Anthropometrics
Participants who completed the 8-week feeding intervention (n = 30) experienced a mean 3.74 lb (3.1%) increase in weight (from 119.91 lbs to 123.65 lbs) (
Anthropometrics for completers only (week 0 vs. week 8, mean ± sd).

Anthropometrics for completers and dropouts (week 0 vs. week 8, mean ± sd).

Change in selected variables (paired t-tests) study completers only (n = 30).

Some glucose samples were hemolysed.
Dietary measures
Completers had a mean total daily energy intake of 2923 kcal, consisting of intake from the nutritional supplement (980 kcal/day, range 625-1500 kcal), and from other foods (1944 kcal/day, range 1190-2374 kcal).
With respect to the composition of the food energy consumed by participants, Table 4 shows the macro-nutrient breakdown of the foods consumed outside of the nutritional supplements provided. When added to the macronutrient profile of the nutritional supplement itself (21.6% fat, 64% carbohydrates, and 14.4% protein), the mean overall macronutrient composition of the total diet of participants was 28.48% fat, 52.79% carbohydrates, and 18.70% protein. Participants largely endorsed liking the taste of the product (see Table 5).
Macronutrient composition of foods consumed exclusive of supplements.

Nutritional supplement taste ratings on a scale of 0 (“hate it”)—5 (“love it”).

The mean rating was 3.0 (SD = 0.76, n = 21).
Immune measures
The immunological studies that were performed were, for the most part, tests of nonspecific immunological parameters, rather than antigen-specific immune functions. Using multicolor flow cytometry, we analyzed the proportions of the major circulating lymphocytes subsets, expression of activation markers on T lymphocytes, and proportions of circulating dendritic cells at two time points, one before and one after the study intervention. Flow cytometry measurements were available for 29 of the 30 participants who completed the study.
Proportions of the maj or lymphocyte sub sets (T cell s, B cells, and natural killer (NK) cells) before and after the study intervention are shown in Table 6. Data are expressed as the percent of lymphocytes belonging to the indicated subset. These three subsets together represent nearly 100% of circulating lymphocytes. None of the subjects studied had overtly abnormal percentages of these subsets. As shown in Table 6, there were no significant changes in the circulating proportions of these cells when comparing the pre- and post-intervention study visits. There were also no significant changes in the two major subsets of T cells (CD4+ or helper T cells, and CD8+ or suppressor-cytotoxic T cells). (Statistical significance was assessed by the paired t-test.)
T cell subsets before and after study intervention, and within-subject changes.
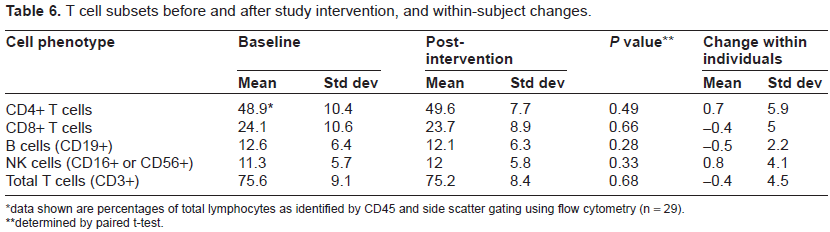
data shown are percentages of total lymphocytes as identified by CD45 and side scatter gating using flow cytometry (n = 29).
determined by paired t-test.
Table 7 shows the expression of several activation markers by circulating T cells (CD3+ lymphocytes). The activation markers assessed were CD69 (an early marker of activation), CD38 (a marker of global cell activation and maturity), HLA-DR (a Class II major histocompatibility protein which is expressed by activated T cells), and CD25 (the α-chain of the high affinity interleukin 2 receptor, expressed on activated T cells and regulatory T cells). Data are expressed as the percent of T cells expressing the indicated phenotype (one or more immunological markers as indicated in the table row headings). Again, there were no major differences between the pre- and post-intervention time points. Only one phenotype (CD38 + CD25-) changed significantly, and that difference was of borderline significance (
Activation marker expression on T cells before and after study intervention, and within-subjectchanges.

data shown are percentages of total (CD3+) T cells as identified using flow cytometry on 25 donors.
determined by paired t-test.
Finally, we analyzed the proportion of circulating lymphocytes that expressed markers characteristic of dendritic cells. These are potent antigen-presenting cells that circulate at very low proportions in the peripheral blood. The dendritic cells were identified by expression of either CD123 or CD11c, along with HLA-DR and a lack of surface markers for T, B, or NK cells. As shown in Table 8, there was a small increase the CD11c+ dendritic cell subset that was of borderline statistical significance (
Percentages of dendritic cells among total leukocytes before and after study intervention, and within-person changes.

data shown are percentages of total (CD3+) T cells as identified using flow cytometry (n = 29)
determined by paired t-test
Table 9 details laboratory blood and serum test results, and is notable for the absence of adverse effects.
Blood and serum laboratory measures: pre vs. post-intervention (mean ± sd) results from all completers/participants with valid lab results, n ≤ 30.

Information in parentheses represents range of values in study population (min-max).
Some post-intervention glucose samples were hemolysed and values may not be reliable.
Discussion and Conclusions
We originally hypothesized that a supplement-enriched diet, in the form of the Quaker Complete Nutrition Foods, would result in improvements in body weight, BMI, and body composition as assessed by bioimpedance. The results suggest that the product did indeed have a significant impact on all these measures over the course of a relatively brief, 8-week intervention period, likely as a result of increasing both total daily energy intake, and amount of protein consumed, both derived from the nutritional supplements themselves, and from an increased consumption of other foods, including those containing a greater amount of protein. 2005 dietary guidelines for Americans from the United States Department of Health and Human Services and the United States Department of Agriculture report that the total daily energy requirements of an average American adult range from 1625 to 3720 kcal, inclusive of height ranges of 59 inches to 71 inches and BMI ranges of 18.5 km/m2 to 24.99 kcal/m2. 10 According to the Food and Agriculture Organization/World Health Organization, between the ages of 20-30 years, an average woman or man with a moderately active lifestyle requires 2410 kcal and 3074 kcal/day, respectively. 11
These figures place our participants completing the study squarely within typical intake levels, in contrast to their pre-study baseline intakes. The mean overall macronutrient composition of the total diet of participants was 28.5% fat, 52.8% carbohydrate, and 18.7% protein. This is also consistent with USDA Food Guide Pyramid recommendations of 20%-35% fat, 45%-65% carbohydrate, and 10%-15% protein, and is sufficiently high in protein to facilitate increases in lean mass accompanying the weight gain experienced. In fact, participants appeared to be more likely to increase their intake of protein from sources even outside of the nutritional supplements provided following initiation of the study.
We also hypothesized that the supplement-enriched diet would result in improvements in body protein stores/albumin, other biochemical parameters, and improvements in immunological function and other immunologic parameters. While biochemical measures other than fasting serum glucose showed no significant change following the intervention, there were no adverse biochemical or blood changes. This suggests, consistent with the anthropometric and bioimpedance results, that the 8-week nutritional supplementation was effective in increasing lean body mass while limiting body fat accumulation. A very recent study conducted in elderly patients with reduced body lean mass showed that dietary supplements with amino acids do increase body lean mass over an intervention period of 8-18 months. 12 We further find that lean body mass can increase over a period as short as 8 weeks in underweight, younger subjects when they are provided with nutritional supplements that contain relatively high levels of protein and are viewed as tasty by participants.
Of note, percent body-fat (% BF), measured by bio-impedance, increased by 1.04 ± 2.65% (
None of the participants experienced significant adverse effects related to consuming the nutritional supplement. Most were able to fully complete the intervention and on average found the taste of the product to be satisfactory. Participants were discharged early from the study if they missed more than 2 consecutive visit appointments and could not be reached by phone to set up follow-up visits. While we do not have a breakdown of reasons for dropout (all subjects dropped were due to missed appointments), many dropouts found it difficult to continue the study if they did not have a ready means of transportation or did not wish to have repeat blood draws.
As a result of the intervention, there were no significant changes in CBC values and/or biochemistry values, except for absolute basophil counts, which saw a modest increase of 9.28 cells/mcl (
We also tested the hypothesis that the immune system would be affected by the nutritional supplement intervention. Tests of general immune function were performed on samples from before and after the intervention. These tests measured serological and cellular immune parameters reflecting overall, rather than antigen-specific status of the immune system. The data indicate that there were very few immune-related changes associated with the intervention. We studied proportions of dendritic cells in the peripheral blood because nutritional interventions have been reported to affect these, but no convincing effect of the intervention in this study was found. There was a slight increase in the number of circulating basophils, the proportion of circulating T-cells expressing one activation marker phenotype out of 19 measured, and one subset of circulating dendritic out of two measured. All of these increases were small and their statistical significance was borderline. If one takes into account the fact that multiple statistical comparisons were made in this study, these changes must be considered preliminary findings that will require replication.
Overall, there were no significant changes in immune function and/or T-cells, nor in dendritic and activation cells following this 8-week intervention. Thus, the data do not support any important changes in numbers or proportions of circulating granulocytes or lymphocytes, or in the activation level of the immune system.
It remains possible that functional assays of immune functions, such as lymphoproliferation assay, detection of secreted cytokines by ELISA, or enumerating individual cytokine-producing T-cells by ELISPOT assay, detection of intracellular cytokines by multi-parameter flow cytometry, measurement of cytokine mRNA levels by real time quantitative RT-PCR, quantifying CTL precursors by LDA, 13 which are more sensitive for assessment of these functions, might have detected effects of the study intervention. However, these tests were beyond the scope of the present study.
Other possible factors that might have contributed to the lack of immunological effects in this study are the relatively short intervention period and the fact that the subjects studied did not show evidence of immunological abnormalities at baseline. Relevant to this conclusion is that a randomized, controlled study involving 96 elderly men and women (mean age 74.5) showed that at the end of 12 months, several immunological responses were statistically significantly improved in the nutritionally-supplemented group. These positive effects included increases in number of T-cells and NK cells, IL-2 production, IL-2 receptor release, NK cell activity, and antibody response to influenza vaccine. This study also showed that improvement in immunological responses was greater among the subjects who were nutrient deficient at baseline and had shown evidence of correction following the use of nutritional supplementation over 12 months. 14
This suggests that, while the current study only showed immune effects that were borderline in significance, a longer-term study and/or one which studies older, more severely nutritionally compromised individuals would be more likely to show a benefit of this type of supplementation on multiple immune markers. On the other hand, the lack of effect of the intervention is reassuring in that there was no apparent adverse effect of the intervention on the parameters measured, including T-cell subsets and immune activation markers. Another limitation of the study is that it utilizes a pre-post design, rather than a parallel control group. While a control group is preferable, we did not feel it was appropriate to offer placebo treatment to undernourished individuals seeking treatment. Moreover, we feel the practical question of whether nutritional supplements do help reverse under/malnutrition can be addressed without a control group.
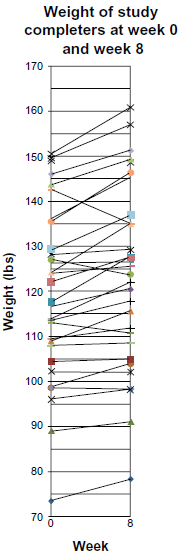
Weight (in lbs) of each study completer at Baseline (week 0) and Post-Intervention (week 8).
Lastly, we hypothesized that the diet would be of favorable palatability, and this was confirmed by the overall high taste ratings from participants in this study. This suggests that Quaker Complete Nutrition Foods may be well-tolerated and of benefit for malnourished individuals interested in using nutrition supplements long-term. While the significance of some findings of this study was constrained due to the relatively small sample size, there are a number of positive outcomes and study strengths. For example, the range of body sizes and the distribution of race, gender, and age was broad, providing a suggestion that the results may generalize across demographic groups.
Given the aforementioned results, we conclude that the findings of this study provide strong support for the utility of the product tested for the short-term treatment of underweight and malnutrition in a broadly-based, US adult population. Future work should explore the outcomes of supplement-enriched diets for long-term use. If such a study is undertaken, we suggest that, although no consistent general immune effects were found in the present short-term study, any future long-term study should look at additional functional parameters of immune function, such as response to immunologic challenge.
Disclosures
This manuscript has been read and approved by all authors. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The authors and peer reviewers of this paper report no conflicts of interest. The authors confirm that they have permission to reproduce any copyrighted material.