
Abstract
This report summarizes a meeting,
Introduction
Obesity (OB) has become a major barrier to the health of people world-wide and is a known risk factor for type 2 diabetes, gestational diabetes mellitus (GDM), ischemic heart disease, hypertension, and several types of common cancers. Maternal pre-pregnancy body mass index (BMI) and gestational weight gain (GWG), which directly or indirectly modify the intrauterine environment, are known to be important predictors of fetal growth 1 and development trajectories as well as contributors to childhood OB.2–10 Infant birth weight is highest in pregnancy complicated by overweight (OW) and OB. Similarly, excessive GWG, independent of pregravid BMI, significantly increases the odds of OW in pre-school, adolescence, and adulthood making fetal development a critical period for downstream OB prevention.11–13 Furthermore, greater GWG is associated with greater post-partum weight retention (PPWR) and subsequent risk of post-partum OB, which has been linked to a wide range of downstream health conditions for both mothers and their offspring.9,14–19 Maternal BMI and GWG are among the most important issues related to the short- and long-term risks for pediatric and maternal OB. Thus, interventions targeted at decreasing maternal pregravid BMI and preventing excess GWG with respect to recently published guidelines from the 2009 Institute of Medicine (IOM) have the potential to significantly impact public health.
In May 2012, a Canadian Institutes of Health Research (CIHR)-funded planning workshop was held that brought together a set of Canadian maternal, fetal, and pediatric health professionals as well as experts in lifestyle intervention, and the relevant knowledge users. Participants, including international speakers from Australia and Brazil, shared expertise and their work in the area of lifestyle interventions aimed to improve maternal–fetal health. The objectives of the workshop were multidimensional and aimed at enhancing national research collaborations prioritizing the development and implementation of a pan-Canadian trial focusing on GWG management to attenuate downstream OB in offspring by promoting optimal growth trajectories. Knowledge synthesis and exchange was accomplished through presentations of the research projects from attendees as well as breakout sessions where subgroups were set up so that those in attendance could discuss and share their expertise, experiences, setbacks, and successes relating back to the pan-Canadian trial design.
The goal of the workshop was to identify the key characteristics and required elements for an effective intervention protocol to minimize excessive GWG and prevent subsequent maternal and childhood OB. Further objectives included:
identifying trial sites, facilitators, and teams of investigators to participate in the development of a pan-Canadian trial targeting the gestational period for submission to peer-reviewed funding agencies and
determining a set of recruitment strategies and study logistics that could be implemented across Canada as well as strategies specific to individual sites that would facilitate successful implementation and execution of the randomized control trial (RCT)
to collaborate with our knowledge users and policy makers as well as stakeholders to promote the trial at the outset and then continue to work with our partner networks and resources to widely disseminate the future trial findings and improve public health outcomes.
Overall, the purpose of this manuscript is to highlight novel and relevant research in the area by summarizing the presentations given on key prenatal lifestyle interventions focusing on physical activity (PA) and nutrition, and outlining the essential elements for implementing a successful trial (eg trial design, recruitment, execution, follow-up, etc.) that were drawn from the workshop.
Conference Presentation Summaries
The Maternal Obesity Management (MOM) Trial–-Kristi Adamo, PhD; on Behalf of the MOM Trial Team, Ottawa, ON, Canada
In Canada, approximately one in two women are OW or OB, 20 and Ontario data suggest that approximately 40% of women enter pregnancy with OW/OB. 21 This is alarming as children born to OB mothers as well as those who exceed GWG recommendations 6 are significantly more likely to be both large-for gestational age1,5,7,15 and OB in infancy and childhood as compared to children of normal weight (NW) mothers who meet recommendations.22,23 Over the last few decades, the incidence of term babies large-for gestational age has increased in both the US 19 and Canada. 24 For women who are OW or OB before conception, an increase in maternal weight gain during pregnancy is correlated with an increase in fetal adiposity 25 and development of insulin resistance in utero. 26 GWG has an independent effect on offspring weight and BMI at pre-school age with data indicating that women who gain equal to or more than the recommended weight during pregnancy increase their risk of having a child who is OW by this age. 22 In addition, the odds of OW in offspring at seven years of age increased by 3% for every 1 kg of GWG. 27 Importantly, children with higher range of BMIs, as early as 24 months, are more likely to be OW at age 12. 28
Thus, it is no surprise that over the past 30 years there has been a parallel and dramatic rise in pediatric OW and OB, which accounts for 26% of 2-17-year-old Canadian children and youth. 29 The battle against child OB is a high priority in Canada from both population health and economic perspectives. Unfortunately, OB tracks closely from childhood to adolescence to adulthood, and more than two thirds of OB children will become OB adults.30–33 Once OB has developed, it is very difficult to reverse and effective treatments are limited making early prevention of paramount importance. It is now evident that weight perturbations during the earliest stages of human development can have lifelong impact on adiposity and associated chronic disease risk.
Therefore, the primary aim of the MOM trial pilot RCT, a study part of the CIHR SOMET (Sherbrooke, Ottawa, Montreal, Emerging Team) grant, is to determine whether a structured prenatal PA and nutrition intervention provided to pregnant women during their second and third trimesters reduces offspring BMI
When designing the MOM trial, it was hypothesized that a greater number of offspring born to women in the intervention group will follow a healthier growth trajectory and thus fewer would be categorized as OW/OB at two years of age. Further, secondary hypotheses were that a larger proportion of participants randomized to the intervention group would meet the IOM-recommended GWG guidelines and that they would give birth to fewer macrosomic offspring while experiencing less PPWR than those in the control group receiving standard obstetrical care.
As both pre-pregnancy BMI and excessive weight gain in all women can contribute to childhood OB, women aged 18 years and more with a BMI above 18.5 were included. Women carrying a single fetus were recruited before 20 weeks gestation through ultrasound clinics, hospitals, obstetricians, midwives, and flyers. Women were randomized into the control or intervention group. Figure 1 outlines the measurements completed on mother and child.

Participant assessments: MOM.
The sample size required detecting a clinically relevant difference of 0.4 in offspring BMI
Limiting Weight Gain in OW and OB Women during Pregnancy to Improve Health Outcomes (LIMIT): A Randomized Trial–-Professor Jodie M. Dodd, Ms Andrea R. Deussen, on Behalf of the LIMIT Investigative Team, Adelaide, Australia
The Australian LIMIT trial was designed to assess whether the combination of dietary and lifestyle (ie PA) advice provided to OW and OB pregnant women to restrict weight gain during pregnancy is effective in improving maternal, fetal, and infant health outcomes. The primary hypothesis of the trial was that dietary and lifestyle intervention provided to OW and OB women during pregnancy would reduce the risk of infants born LGA (defined as birth weight above the 90th percentile for gestational age and sex). In this multi-center RCT, women were eligible for inclusion if they were giving birth to a live, singleton infant; were recruited between 10 and 20 weeks gestation; and were OW or OB. At the time of trial entry, women were stratified according to their BMI (OW vs. OB), parity (nulliparous vs. multiparous), and the center where they planned to give birth.
Women randomized to the dietary and lifestyle intervention group received a comprehensive intervention aiming to limit GWG in pregnancy that included a combination of dietary, exercise, and behavioral strategies, delivered by trained research dietitians and research assistants. The intervention group was divided into three sub-categories: group versus individual dietary and exercise counseling, group versus individual-based exercises, and provision of informational DVD or no DVD. The dietary advice provided was consistent with current Australian dietary standards, whereas PA advice was based on the guidelines of Royal College of Obstetricians and Gynaecologists (RCOG, UK). Booklets of dietary guidelines; exercise guidelines; for recording diet and exercise goals and achievements; and recipe were provided to the intervention group. An informational DVD was given to half of the intervention women. Secondary study outcomes included a variety of maternal and infant clinical health outcomes, maternal quality of life and well-being, and health care costs. Additional measures to inform mechanistic studies designed to explore potential molecular links between maternal OB and GWG and neonatal growth were also collected and are outlined in Figure 2.

Participant assessments: LIMIT.
The estimated sample size for this trial was 2,180 women and was powered to detect a 30% reduction in the risk of infants born LGA from 14.4 to 10.1%, allowing for 15% attrition. Recruitment of women took place at three metropolitan hospitals representing 10,600 births per annum (approximately 400 per week) across 26 obstetric booking clinics each week. At the majority of clinics, women were approached and screened by research assistants.
Recruitment for the trial commenced in May 2008 and was completed in February 2012, and the last infant was born on July 2012. Approximately 150 eligible women were identified each month of which approximately 40% consented to participate. Follow-up of women and their infants at 6 and 18 months post-partum is currently underway. Approximately 45-50 women were randomized each month to either the treatment or control group. Women in the treatment group received written information about healthy diet and exercise in pregnancy, attended two appointments with a dietitian, and were contacted by telephone on three occasions to review diet and exercise changes and goals. Women in the control group received the current standard antenatal care in Australia with limited dietary and exercise information.
The main barriers to recruitment included time constraints at the first prenatal visit, sensitivities regarding weight-related discussions, protectionism of the staff, and resource-intensive nature of the study. On the other hand, some recruitment procedures that aided in patient enrollment (ie “recruitment enablers”) included ensuring research staff members were sensitive and actively listened to women telling their story about the current pregnancy, and ensuring women were informed of the screening process that involved calculation and classification by BMI. Finally, it was important to develop a positive and professional relationship between the research assistants and clinic staff (particularly, research staff respecting and prioritizing the core work of the clinic) that ensured sustained enrollment.
Overall, the LIMIT trial was successful at designing and implementing a multi-centered RCT. A great strength of this trial, which is an important factor to take into account for a pan-Canadian trial, was the integration of study staff at the clinics. This allowed effective recruitment and meeting the large sample size goal.
The Nutrition and Exercise Lifestyle Intervention Program (NELIP) Experience in London, Canada–-Michelle F. Mottola, PhD, FACSM, on Behalf of the NELIP Team, London, ON, Canada
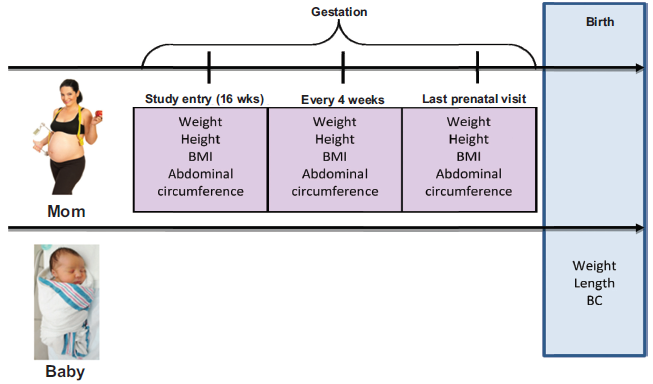
The NELIP investigates the effects of nutrition and exercise on OW and OB pregnant women. It aims to prevent excessive weight gain and the development of GDM. This program was evaluated with a single-arm intervention study using historical controls matched by pre-pregnancy BMI, age, and parity at a ratio of four controls to one intervention participant. All women were medically pre-screened, and 90 women entered the study at 16-20 weeks gestation. Figure 3 outlines the study assessment timeline. They followed NELIP until delivery and completed 24-hour food records weekly. The nutrition intervention was a modified GDM diet with a daily target of 2000 kcal, 200 g carbohydrate (40-55% of total energy), emphasizing small frequent meals and providing education on serving size. The exercise program was individualized based on a peak fitness test (30% of peak heart rate (HR) reserve). Participants were required to walk three to four times per week with an average target HR of approximately 118 beats per minute (bpm). They were also required to wear a pedometer and keep an exercise log.

Participant assessments: NELIP or *NELIP + FBBT. Measures related to NELIP and FBBT only.
The preliminary results found in Table 1 were published in 2010.36,37
NELIP outcomes.
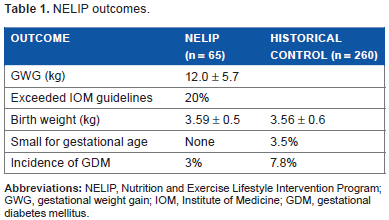
There was also a decrease in the number of babies born with a birth weight between 4.0 and 4.5 kg in the OW NELIP women (3.2%) compared to the matched cohort (18%). At delivery, within 6-18 hours after birth, girth and skinfold measurements were taken for the NELIP babies and compared to a reference group of NW women (
Following the original NELIP evaluation, we examined the weight history of OW and OB women (
Subsequently, we developed a family-based behavioral treatment (FBBT) program to be delivered with NELIP during pregnancy with a re-introduction of the program at two months post-partum (Clinicaltrials.gov (NCT01129505)) with a stroller walking program. We also added a behavioral component in a group session format that included sessions during pregnancy including Phase 1 (weeks 1 and 2 of the program): Motivation and Initiation–-“Healthy Me, Healthy Baby,” Phase 2 (weeks 3-6): Adoption–-“A Time for Change,” and Phase 3 (weeks 7-18): Maintenance–-“Sticking with Things.” We have just completed this study with one year follow-up and are currently examining the difference between the NELIP with no post-partum intervention (
We were concerned with the observation that many of our women gained excessive weight before the intervention began at 16-20 weeks gestation. We have recently published a paper examining 172 pregnant women: 33.7% were NW, 33.7% were OW, and 32.6% were OB 39 who participated in the NELIP program. We examined weight gain before the intervention at 16-20 weeks, and weight gain on the NELIP intervention to delivery. To examine the timing of excessive GWG compared to newborn body fatness at birth, we divided the group of women into (1) appropriate GWG (ie within IOM recommendations) in the first and second halves of pregnancy (overall appropriate), (2) appropriate GWG in the first half of pregnancy and excessive GWG in the second half of pregnancy (late excessive), (3) excessive GWG in the first half of pregnancy and appropriate GWG in the second half of pregnancy (early excessive), and (4) excessive GWG throughout pregnancy (overall excessive) based on their pre-pregnancy BMI category. We then compared these groups to infant birth weight and infant adiposity. The results indicated that the timing of excessive maternal weight gain, specifically during the first half of pregnancy, is a stronger predictor of infant body fatness at birth than total maternal weight gain regardless of pre-pregnancy BMI. Thus, the timing of excessive maternal GWG is important, and perhaps interventions aimed at prevention should occur earlier than 16 weeks, even in the pre-conception period, which may suggest an important role of the early maternal in utero environment on the fetal programming of OB.
Although the use of a historically matched control is a limitation of these studies, this design allowed for successful completion of the study given that retention of control participants is a significant issue with RCTs. The NELIP trial did successfully recruit participants, had low attrition rates, and had results that showed promise toward the direction the group hypothesized. An important finding of these studies was that prevention of excessive GWG should be initiated as early as possible.
Experience from the Community-Based Dietary and Exercise Trials in Manitoba–-Garry Shen, MD/PhD, on Behalf of the IDEA (Impact of Diet and Exercise Activity on Pregnancy Outcome) Trial Team, Winnipeg, MB, Canada
The IDEA study group is led by Dr Garry Shen at the University of Manitoba. The group has conducted a series of epidemiological studies on GDM in Manitoba. Their studies analyzed more than 9,000 women with GDM and >300,000 births between 1985 and 2004 across the province. It was discovered that the prevalence of GDM in pregnant First Nations (FN) women was two to three times higher than in non-FN women in urban or rural areas. 40 The findings demonstrated the tendency toward GDM and other unfavorable pregnancy and/or fetal outcomes (delivery of macrosomic infants and increased risk of dystocia) in Manitoba and the greater risk for FN women, particularly those living in rural/remote regions of Manitoba.
Following these findings, the IDEA group developed a community-based lifestyle intervention program for pregnant women. 41 The program has been evaluated through a randomized controlled trial for urban-living pregnant women who were recruited within 20 weeks of pregnancy. Participants with known diabetes, and medical and obstetric contraindications to exercise or multiple gestations were excluded. All participants consented and were randomized into the control or intervention groups. The primary end point of the study is excessive weight gain according to 2009 IOM guidelines. Secondary outcomes include GDM, LGA infants, maternal PA, and food intake. The exercise program for pregnant women in the intervention group included weekly group sessions and home exercise three to five times per week. Our team developed an instructive exercise video suitable for pregnant women to standardize group exercise and to assist home exercise. A professional trainer and local pregnant women with different cultural backgrounds were invited to be cast members of this video. The video includes walking, and aerobic and strength exercises. Dietary interview and counseling were provided to participants in the intervention group. An example of dietary interview record with assistance of Food Choice Map software is available. 42 Dietitian and interviewee collaboratively placed magnetic stickers with images of foods on the map that represent the frequency and quantity of food intake. The information was scanned into a computer after the interview, and the data were analyzed instantly. Dietitians provided individual counseling to participants based on the data during the session.
At the time of analysis in 2010, 190 participants had completed the program, 88 in the control group and 102 in the intervention group. No significant differences were detected in age, pregravid BMI, proportions of FN, or family income between the two groups. More than 25% of participants had FN status, and more than 70% the participants were from families with low or below average incomes. PA at baseline was comparable between the two groups. Two months after the implementation of the intervention, participants in the intervention group had significantly higher PA than the control group. Similarly, there was no significant difference in total caloric intake between the two groups at baseline; however, two months after enrollment, the intervention group had a significantly lower total caloric intake than the control group as well as a significantly lower intake in total fat, saturated fat, and cholesterol. The intervention group gained 7% less weight during pregnancy than controls, but the difference was not statistically significant. Birth weight and the rates of LGA, GDM, and cesarean-section were not significantly different between the two groups. Excessive GWG in the intervention group was significantly lower than that in the control group according to the 2009 IOM guidelines. 43
The findings suggest that community-based exercise and individualized dietary counseling during pregnancy may increase PA, improve dietary habits, and reduce excessive GWG in urban-living pregnant women. As FN women in rural regions have higher risks for GDM, OB, and type 2 diabetes, the IDEA study group has undertaken non-randomized studies to promote healthier lifestyle to improve the health of FN women and children in rural/remote FN communities in Manitoba. 44
Overall, from the IDEA trial we learned that recruitment of participants may be improved by stronger advertisement and by training family doctors and midwives in the city on the principles outlined in the study. An understanding that randomization may affect recruitment to a certain degree is important when planning a large-scale study. Maintaining adherence is a challenge for the study while close follow-up and peer support may help to improve the adherence of participants to the study. Finally, it is important to note that PA assessments through self-reports may not be sufficiently accurate as previous research has demonstrated. 45 Overall, the messages learned from this study regarding planning and implementation align with the previous prenatal interventions discussed.
The Effect of an Antenatal Physical Exercise Program on Maternal/Perinatal Outcomes and Quality of Life in OW and OB Pregnant Women: A Randomized Clinical Trial–-Simony Lira do Nascimento, São Paulo, Brazil
In this intervention study, OW and OB pregnant women were randomly assigned to either an intervention group that received prenatal nutrition information and an exercise protocol including home exercise counseling or a control group that had prenatal and nutrition information only. The primary outcome in the study was a reduction in excessive weight gain during pregnancy, and the secondary outcomes were maternal weight gain, blood pressure, quality of life, and fetal outcomes (newborn weight, Apgar scores, prematurity rate, and adequacy).
Participants were OW pre-pregnancy, >18 years old, and were recruited at 14-24 weeks gestation. Women with absolute contraindications to exercise during pregnancy 46 were excluded. The data collection took place, according to that outlined in Figure 4, from August 2008 to 2010.
Participant assessments: Brazil.
The intervention program counseling covered IOM GWG recommendations specific to their BMI category, 37 the importance and effects of PA during pregnancy, the optimal amount and intensity of home exercise, general healthy nutrition counseling and appropriate caloric intake for exercising, suitable clothing to wear when exercising, signs and symptoms to look out for during exercise, and when to cease PA. The exercise program was designed to enable pregnant women to increase their level of PA and to improve their quality of life through simple exercises that could be performed without supervision and that did not present a risk to the mother or the fetus. The program was composed of two components: an exercise protocol once a week supervised by a trained physiotherapist and a home exercise protocol or walking five days per week, recorded in an exercise journal/diary. The exercise protocol included 22 exercises with intensity varying from light to moderate for a total of a 40-minute session (10 minutes stretching, 20 minutes muscle training, and 10 minutes relaxation) such that the HR must be kept below 140 beats per minute. 46 Before and after exercise class, their blood pressure was measured and they were weighed.
A total of 40 women were randomized to the intervention and 42 to the control group, and 39 and 41 completed the follow-up, respectively. The majority had less than a high school education, were without remuneration or unemployed, and had more than one child. Prevalence of hypertension and/or diabetes was high in this population. At baseline, most women were at approximately 17 weeks gestation. According to the IOM's weight gain guidelines, 48% of the intervention participants compared to 57% of the controls gained excessive weight (
Limitations included a low adherence/compliance mainly in relation to home exercise counseling. 62% recorded their exercise routine in a diary with a mean of 12.3 weeks of home exercise and the average minutes of weekly exercise with 57 ± 22.2 exercise protocol minutes per week and 79.8 ± 46.9 walking minutes per week while the recommendation was 150 minutes. Another difficulty was in determining and ensuring the optimal type, frequency, intensity, and duration of exercise at home. This study was also limited by the small sample size, social conditions, and barriers to participation, such as cultural perception of having to rest during pregnancy, cost of transportation, proper clothing to wear while exercising, and childcare.
The important lessons learned from these national and international projects to be applied to a future pan-Canadian trial include addressing (i) high attrition, (ii) loss to follow-up, (iii) lifestyle intervention fidelity, (iv) obstacles to recruitment and adherence, and (v) burden to the participant. Randomization to the control group leads to an increased likelihood of participant drop-out; these women enroll because they are ready for a lifestyle change and they seek the support provided in the intervention aspect of the study. It is agreed that an incentive of some sort should be provided to the control participants to increase the likelihood that they continue participating in the trial. However, there are institutional differences in research ethics board acceptance of this practice. Adherence to exercise programs in general is suboptimal, and thus compliance to the intervention itself can be a challenge when the sessions are at scheduled times. In addition, childcare can be an obstacle limiting participation in exercise in weekday group classes for women with other children.
Many health care providers find it difficult to approach OW and OB pregnant women, and some of these women may be resistant to weight-related dialog because of pre-existing weight issues. Pregnancy may exacerbate this sensitivity, making recruitment and adherence to intervention programs challenging. The best approach to recruitment seems to be the integration of research staff into clinics and building relationships with the staff as was done in the Australian LIMIT trial. This approach appeared to have alleviated part of the recruitment issues faced in the MOM trial and Brazilian trial. Moreover, the timing of the intervention is crucial. It appears that intervening before 16 weeks may be necessary to have a significant impact on GWG. Finally, PA self-reporting is notoriously inaccurate and accelerometers are expensive to purchase and replace, thus identifying the need for an affordable and reliable tool that quantifies PA.
Summary of Breakout Sessions
Following the presentations and overview of current prenatal interventions, attendees were divided into groups based on their expertise for the afternoon portion of the meeting to discuss various requirements in planning the pan-Canadian trial. Below is a description of the key consideration points concluded from each breakout session.
Group 1: Methodological Considerations when Implementing a Multi-Site RCT
Among other considerations, the direction of the pan-Canadian pregnancy weight management trial requires the decision of the design (cluster vs. non-cluster) and the primary outcome. The options discussed included (1) child adiposity or BMI outcome downstream, (2) macrosomia (birthweight > 90th percentile), (3) meeting the IOM GWG guidelines, and (4) infant birth weight. Potential secondary outcomes of interest are as follows: rate of weight gain, GWG, LGA, PPWR, adverse prenatal/antenatal outcomes, barriers to adherence, self-efficacy, and quality of life. For the sample size, a realistic target from a costing and logistics perspective would be approximately 1,000 participants; however, there are certain caveats to consider. First if a downstream child adiposity outcome is chosen, there is considerable evidence to suggest BMI
It is customary that multi-center trials have one central coordination site and with the help of health informatics, the management of data would be centralized and electronic to facilitate data sharing. The RCT design could range from two to four arms with options for each arm including diet, exercise, combination (diet and exercise), and control. Furthermore, to simplify the randomization of multiple centers, it was decided that cluster-randomization might be logistically simplest and applied by practice and stratified by BMI category (ie OW/OB/NW).
Group 2: Designing an Effective PA Intervention
For the intervention aspect of the study, there was a debate over personalized plans versus standardized “one-size fits all” programs and how to best assess/monitor the effectiveness of these programs’ ability to change PA behaviors. There was a consensus that an initial in-person visit for safety advice and guidance is necessary. Follow-up may be provided by telephone counseling, internet counseling, or smart phone application. All women would be monitored; however, only those who are falling below PA guidelines or above sedentary guidelines would be prompted with active strategies to encourage guideline attainment. For exercise modality, there was a strong consensus toward implementing a walking program as it is accessible to almost everyone, easy to implement, and requires very little equipment and limited training. However, it is dependent on weather and neighborhood safety; yet walking groups in a safe place (mall, arena, school, etc.) may circumvent this issue. If walking is the exercise of choice, an effective way to monitor it must be selected above and beyond self-reported log books. Options include pedometers (everyday use) or accelerometers (more comprehensive time stamped, capturing omni-directional movement, ability to provide data on intensity), which allow for goal setting and monitoring of progress. A study minimum of a 10,000 steps/day (evidence-based recommendation for health chronic disease prevention) 47 could be set and increased once or several times throughout the pregnancy depending on progress. As for the timing of the PA intervention, there could be multiple arms, intervening during early and later stages of pregnancy as well as post-partum. The type of exercise chosen will ultimately depend on the main outcome of the study (eg GWG vs. general health improvement).
Group 3: Designing an Effective Nutrition Intervention during Pregnancy
The first consideration in designing the nutrition intervention is to decide on a valid and reliable method to quantify baseline eating behavior of study participants. For example, before study initiation a tool must be selected to identify a nutrition plan for the women and may include a seven-day food record, diet prescription based on resting energy expenditure (REE), a food frequency questionnaire, or comprehensive interview conducted by a dietitian. Furthermore, a decision on whether personal circumstances would be taken into account is required and if so how to best manage these considerations. For example, the number of dependent children at home, type of employment, cooking skills, nutrition knowledge, and income are important factors that can enable or prevent the success of the intervention. A “knowledge of nutrition” screening test could be completed at baseline; this could build in cultural components and SES/food insecurity questions. Once this is established, a daily caloric goal and plan will be decided upon. For the nutrition plan, it can be either a general advice or modifications to current dietary habits and the study-specific interventionist will work with the participant to increase adherence. Furthermore, although there are no set guidelines on extra calories, current literature points toward a small requirement for additional calories during the second and last trimesters and Health Canada endorses the IOM recommendation 48 that an additional 1420 kJ (340 kcal) and 1880 kJ (450 kcal) is sufficient to support healthy weight gain during the second and third trimesters of pregnancy, respectively. However, it is important to identify baseline eating behaviors as many women are already consuming calories in excess regardless of pregnancy status. Further, assessment and monitoring of energy intake is important and there are many potential ways this can be accomplished. Consensus from the meeting indicated that this may be done via hand-written logs, online diet records, or 24-hour food recalls. Additional information may be provided through multiple avenues including a pregnancy handbook, webinars, podcasts, or postcards send via mail. Finally, ongoing support may be provided through web application dedicated specifically for the study, through Facebook or automated SMS (ie text) messages. With respect to the exercise information, it was recognized that centralized and uniform messaging is crucial to ensure success for these pregnant women.
Group 4: Strategies to Maximize Recruitment
With respect to intervention enrollment, recruitment may be accomplished by “flagging” potential participants through medical charts at participating centers. Traditional pamphlets and flyers may be an additional strategy and could be posted/distributed through prenatal classes, ultrasound clinics, family physician offices (initial confirmation of pregnancy), OB/GYN clinics, midwives, public health organizations, and pharmacies. Integration of research staff directly into clinics or contributing to a portion of clinic staff remuneration may facilitate recruitment and acknowledge the staffs’ efforts in trial participation. Engaging midwives, family doctors, and clinic staff before the study launch is crucial to ensure reach to as many potential participants as possible.
Group 5: Thinking Forward-Knowledge Translation (KT) Strategies to Improve Nation-Wide Education of Expecting Mothers
KT is a key component for this pan-Canadian study. The future study will be designed to respond to the gap of readily available access to evidence-based information for pregnant women and the inadequate personalized guidance they receive from prenatal health care providers. We plan to engage in a dynamic and integrated form of KT for the key target audiences: pregnant women, health care providers, and policy makers. We plan to adapt the intervention tools through consultation with pregnant women and health care providers over the course of pre-RCT testing. By educating the care providers on the proposed study objectives, goals, purpose, and clinical importance, they will provide information to patients, which is essential for the success of the future trial. To have sustainable impact on prenatal care practice and on long-term health in Canada, it is critical to target policy makers who can facilitate change, and influence implementation and integration of intervention tools into health care planning and delivery strategies.
While our final dissemination strategy is contingent on the study progress, we plan to disseminate the results to pregnant women through social media, pregnancy forums, and blogs using a project “infographic”. To reach health care providers, who expect clear, action-oriented messaging delivered through their professional organization, we intend to leverage our various knowledge user-based partnerships to allow for local, provincial, and national KT to be delivered through various modalities. Importantly, knowledge partners will work with us to champion our quest to incorporate a competency-based OB and GWG theme into their continuing medical education requirements. It is through policy makers and their directives that the usefulness of intervention tools is acknowledged and ultimately accepted as benchmarks of best practice.
Conclusions
We are currently developing a pan-Canadian trial using the information discussed at the meeting as well as the recent evidence that has emerged in the literature since. Our plan is to implement an intervention strategy that will be feasible to integrate within the existing health care system as to complement current health services and not disrupt standard care provision. The main issues to address in the planning of the pan-Canadian trial are as follows:
dealing with the delicate and sensitive weight-related issues during pregnancy (see Canadian Obesity Network 5As for healthy pregnancy weight gain) 49
compliance to behavior intervention and study in general
dealing with randomization effect on drop-out rate
face-to-face recruitment and integrating study into day-to-day activities in clinics and thus build relationship with the staff members
timing of the intervention to have a significant impact on GWG, before 16 weeks
involving a corporate partner to have incentive to keep controls actively enrolled
PA self-reports are not sufficiently accurate, and accelerometers are expensive to purchase or replenish if misplaced. Pedometers are reasonably priced and may be good motivators
lack of childcare limits participation in exercise at home and for group classes
electronic tools to help in management of trial, data, and intervention aspects are necessary.
In-person or provider-based delivery of weight management interventions is not feasible to reach a national population as required from a public health perspective. Workshop attendees indicated that intervention participants require personalized, real-time feedback and a desire for more control over program scheduling. Thus, addressing limitations to current practices in managing and intervening with regard to GWG requires novel, innovative, and strategic approaches to optimize the health of mom and baby. Therefore, the overall recommendation from the workshop indicated the need to capitalize on the rapidly emerging usage of eHealth resources and mobile technologies to deliver health behavior interventions in terms of promoting healthy eating and PA and managing GWG. Mobile and other technologies are now ubiquitous in modern society with 99% of the Canadian population having access to wireless networks and 90% of the population owning a mobile phone.50,51 Furthermore, approximately 70% of women of child bearing age are regular smartphone users.50,51 While studies involving such technologies can improve health behaviors in non-pregnant populations52,53 or in post-partum women, 54 few have explored their utility in the prenatal and early post-partum period. Therefore, mobile technology-based interventions are being developed to curb excessive GWG and convey primary health information that is critical to the well-being of both mom and baby. These interventions are expected to have a beneficial impact as a cost-effective solution for providing frequent, “real-time” feedback to the patient without the use of additional clinic visits, thus reducing the burden of the currently underfunded and overutilized Canadian health care system. The ultimate goal will be adoption of these eHealth technologies into regular prenatal care to provide women with the opportunity to extend their pre and pregnancy-related health knowledge and greater personal engagement in their prenatal care through access to information and regular feedback. Thus implementing a novel study of this nature may ultimately lead to a reduction in pregnancy-related maternal–fetal complications, establish a strong healthy foundation at birth, and promote optimal long-term child wellness for future generation.
Author Contributions
Conceived the concept: KA, ZF, SJP, MM, GS, SN, JD. Wrote the first draft of the manuscript: KA, ZF, SJP, MM, JD, GS, SN. Contributed to the writing of the manuscript: All authors. Agree with manuscript results and conclusions: All authors. Jointly developed the structure and arguments for the paper: All authors. Made critical revisions and approved final version: All authors. All authors reviewed and approved of the final manuscript.
Disclosures and Ethics
As a requirement of publication the authors have provided signed confirmation of their compliance with ethical and legal obligations including but not limited to compliance with ICMJE authorship and competing interests guidelines, that the article is neither under consideration for publication nor published elsewhere, of their compliance with legal and ethical guidelines concerning human and animal research participants (if applicable), and that permission has been obtained for reproduction of any copyrighted material. This article was subject to blind, independent, expert peer review. The reviewers reported no competing interests.
Footnotes
Acknowledgments
KB Adamo acknowledges the Canadian Institutes of Health Research (CIHR) for funding the workshop the led to this publication (KTM-119165). She also acknowledges CIHR-SOMET (MOP-88590) and the Ottawa Dragon Boat Foundation for their support in the MOM trial. M Mottola acknowledges the CIHR and the Rx&D Health Research Foundation for funding support of the NELIP trial. J Dodd acknowledges the support from the Australian National Health and Medical Research Council (NHMRC) for the LIMIT trial. GX Shen acknowledges the grant support from CIHR, Public Health Agency of Canada, and Lawson Foundation for the IDEA study. S Nascimento acknowledges financial support from the Coordination for the Improvement of Higher Education Personnel (CAPES) Foundation. We would also like to acknowledge participants from the University of Adelaide (A Deussen), the Ottawa Hospital Birthing Unit (L McCabe), the Dietitians of Canada (P Vanderkooy), the Canadian Society for Exercise Physiology (M Duggan), CIHR-IHDCYH (E Fowler), the Canadian Association of Midwives (P McGiven), Best Start-Health Nexus (M Brisson), the Royal College of Physicians and Surgeons of Canada (T Horsley) and BORN Ontario (S Dunn, A Sprague) and the Perinatal Epidemiology Research Unit, IWK Health Centre (C Woolcott) and HALO (K Brett, A Harvey) for their contributions to the workshop.