
Abstract
Critical limb ischemia (CLI) due to obstructive atherosclerosis causes pain and tissue damage and may result in amputation and death. Revascularization saves the limbs and lives of patients with CLI. This review addresses adjunctive tools for lesion crossing, including mechanical atherectomy, laser atherectomy, crossing devices, and luminal reentry devices. Mechanical atherectomy devices are designed to excise atheroma, often heavily calcified, thereby preparing a channel for further intervention. Mechanisms (and devices) include directional (SilverHawk™, TurboHawk™, RockHawk™), rotational (Jetstream™, Pheonix™), and orbital (Diamondback 360°™, Predator 360°™, Stealth 360°™) atherectomy. A laser atherectomy device (Turbo Elite™) vaporizes atheroma by heating tissues with ultraviolet light. Crossing devices specifically designed for chronic total occlusions either navigate a vessel's true lumen or guide a controlled subintimal course with reentry into the distal true lumen. Crossing devices include Crosser® Catheter, Wildcat™, Ocelot™, Kittycat™, TruePath™, Viance™, Frontrunner™, TOTAL across™, and PowerWire™. When a guidewire or crossing device traverses a lesion via a subintimal course, a luminal reentry device may facilitate deployment of the guidewire in the distal vessel lumen. Reentry devices include Outback LTD™, Offroad™, Pioneer Plus™, and Enteer™.
Introduction
Critical limb ischemia (CLI) occurs when multilevel calcific atherosclerosis obstructs arteries such that residual blood flow is chronically insufficient to meet the metabolic demands of tissues in the downstream angiosome, resulting in pain at rest, nonhealing ulceration, or gangrene. As opposed to acute limb ischemia, which results from thrombotic or embolic events, CLI develops over months to years. Complications of CLI may include amputation, sepsis, and death.1–3
Revascularization saves CLI patients’ limbs and lives. 4 In particular, a meta-analysis of 2,029 patients with chronic peripheral arterial disease (PAD) demonstrated a reduction in amputation frequency from 95% to 25% when revascularization was undertaken in patients with CLI, defined as Rutherford class IV–VI symptoms, ankle systolic blood pressure <50 mmHg, nonpulsatile photoplethysmography, or transcutaneous oxygen pressure <30–50 mmHg. 5 The BASIL trial compared percutaneous transluminal angioplasty (PTA) and bypass surgery for CLI in patients whose diagnostic imaging demonstrated anatomy subjectively amenable to either approach: generally, this excluded patients with very long lesions or bilateral or multilevel aortoiliac disease (Trans Atlantic InterSociety Consensus Class D). BASIL demonstrated similar rates of amputation-free survival at 1 year (71% vs 68%) and 3 years (52% vs 57%) and reduced intensive care unit admission (27% vs 7.5%) with PTA. Given this lower inpatient morbidity, PTA is the preferred initial approach to CLI revascularization in patients with appropriate lesion anatomy. Indeed, PAD patients represent a high-surgical-risk population given the prevalence of comorbidities such as ischemic heart disease (35.8%), stroke (16.2%), renal disease (27.1%), and chronic respiratory disease (18%), 6 so a minimally invasive percutaneous approach is favored whenever possible.
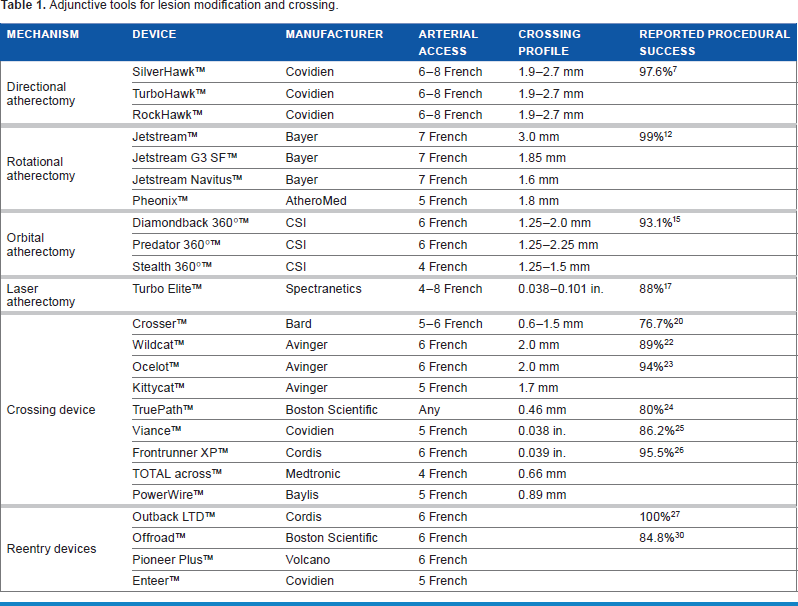
Percutaneous revascularization requires accessing an atherosclerotic target lesion with a catheter, crossing the lesion with a wire, and balloon-dilating a channel for blood flow. The following review will address adjunctive tools for lesion modification and crossing, including mechanical atherectomy, laser atherectomy, crossing devices, and luminal reentry devices (Table 1). Catheters, wires, balloons, stents, and distal protection devices are discussed separately in this review.
Adjunctive tools for lesion modification and crossing.
Mechanical Atherectomy
CLI lesions present challenging targets for PTA or surgical revascularization: their length and heavy calcification impede wire-crossing and increase the risks of dissection and perforation. Mechanical atherectomy devices are designed to excise atheroma, often heavily calcified, thereby preparing a channel for further intervention. Mechanisms include directional, rotational, and orbital atherectomy.
Directional atherectomy devices resect atheroma circumferentially in the longitudinal plane. A rotating, angled blade excises the plaque into a microefficient compression compartment. Current FDA-approved directional atherectomy devices include the single-blade SilverHawk™, its more efficient, four-blade successor TurboHawk™ (Fig. 1), and RockHawk™, in which a rotating burr distal to the blades ablates calcified lesions at the expense of increased risks of dissection and distal embolization (Covidien). The Covidien directional atherectomy devices require 6–8-French vascular access. The TALON Registry of 601 PAD patients treated with SilverHawk™ followed by PTA or stenting demonstrated 80% primary patency at 1 year. 7 Results of the DEFINITIVE-LE study have been presented, and are pending publication: in 799 patients with claudication or CLI treated with SilverHawk™, primary patency at 1 year was 78% among claudicants and 71% in the CLI cohort. 8 The DEFINITIVE-Ca++ study applied SilverHawk™ or TurboHawk™ to 133 patients including 21 with CLI, reporting a mean 33.3% residual diameter stenosis, only nine major adverse events within 30 days, and no 30-day patient mortality. 9 Principal risks include target vessel dissection, perforation, and distal embolization. However, a two-center, randomized trial of SilverHawk™ versus PTA in 58 PAD patients demonstrated no difference in rates of successful revascularization or repeat revascularization at 1 year. 10

TurboHawk™ four-blade directional atherectomy device. 11 Turbohawk is a trademark of a Medtronic company. © Medtronic. All rights reserved.
In rotational atherectomy devices, a rapidly spinning, diamond-coated burr ablates atherosclerotic plaque, releasing 5–10 micrometer particles into the distal circulation for eventual clearance by phagocytosis. The 7-French Jetstream™ system (Bayer) was evaluated in the Pathway PVD trial of 172 PAD patients: at 1 year, restenosis was observed in 38.2% of patients. 12 The Tissue Removal by Ultrasound Evaluation (TRUE) study demonstrated a mean 11.8% reduction in plaque volume with use of the Jetstream™ device. 13 The Jetstream G3 SF™ is indicated for proximal vessels, while the Jetstream Navitus™ employs a smaller burr for use below the knee. The investigational Phoenix™ rotational atherectomy system (AtheroMed, Inc.) is currently undergoing evaluation.
Orbital atherectomy employs a rapidly spinning shaft topped by an eccentrically shaped, diamond-coated crown. As the crown ablates the plaque, its rotational radius increases, and a centrifugal force is applied to the crown against calcified plaques with increasing force as the luminal area increases, while allowing normal vessel walls to flex away from its pressure. By reducing arterial calcium while preserving normal vessel wall, orbital atherectomy is hypothesized to increase vessel compliance, allowing for safer balloon delivery and minimizing the need for bailout stenting. 14 The original 6-French Diamondback 360°™ (CSI) is marketed along with two newer devices, the Predator 360°™, with a solid tungsten crown shaped to optimize frontal sanding of chronic total occlusions, and the Stealth 360°™, with a 4-French profile and flexible shaft designed for use in tibioperoneal vessels. The CALCIUM 360° trial of 50 CLI patients with tibeoperoneal disease demonstrated 93% procedural success, 3.4% dissection, and 7% stenting in patients treated with orbital atherectomy and PTA compared with 82% procedural success, 17.1% dissection, and 14% stenting in those treated with PTA alone. At 1 year, freedom from target lesion revascularization and all-cause mortality were 93% and 100%, respectively, in the orbital atherectomy plus PTA cohort versus 80% and 68% in the PTA-alone cohort. 15 The CONFIRM registry of 3,135 PAD patients with 4,766 lesions treated with orbital atherectomy reported an 11.3% dissection rate and 5.7% stenting frequency.
A 2013 single-center, retrospective analysis of 418 tibial interventions for CLI compared 79 cases of any atherectomy modality plus PTA to 339 cases of PTA alone, finding no difference in successful revascularization, primary or secondary (successful re-intervention) patency at 12 and 36 months, limb salvage, or survival. 16 Further studies are necessary to confirm or refute these findings.
Laser Atherectomy
Predating mechanical atherectomy devices, the excimer laser fiber-optic catheter vaporizes atheroma by heating tissues with ultraviolet light. Slow catheter advancement is required to allow for maximal plaque diameter reduction. The Turbo Elite™ (previously CliRpath™; Spectranetics), available in 4–8-French sizes, was initially evaluated for CLI use in a study of 40 patients, 26 with CLI, with procedural success in 88% of cases and 12-month primary patency of 44%. 17 The multicenter LACI trial of 145 CLI patients with contraindications to bypass surgery reported procedural success in 86% of lesions and limb salvage at 6 months in 110 (92%) of 119 surviving patients. 18 The multicenter CELLO trial of 65 PAD patients undergoing laser atherectomy plus PTA or stenting reported 54% 12-month vessel primary patency. 19
Crossing Devices
Given the difficulty of crossing long, calcified lesions with standard wires and catheters, a variety of specialty lesion-crossing devices have been developed. Specifically designed for chronic total occlusions (CTOs), these devices either navigate a vessel's true lumen or guide a controlled subintimal course with reentry into the distal true lumen.
The Crosser® Catheter (Bard) is composed of a nitinol core with a stainless steel or titanium tip that vibrates at 20,000 cycles per second with 20 µm amplitude to effectively drill an intraluminal course through calcified lesions (Fig. 2). A single-center trial of 56 PAD patients with 73 CTOs reported 77% primary and 88% secondary successful recanalization. 20 Failure was predicted by lesion length longer than 100 mm and calcification within 10 mm of the distal cap. The Crosser™ system is available in 5- and 6-French compatibility.

Bard® Crosser® vibrating crossing device. 21 © 2015 C.R. Bard, Inc. Used with permission. Bard and Crosser are registered trademarks of C. R. Bard, Inc.
The Wildcat™ catheter (Avinger) has a rapidly rotating distal tip with retractable wedges that give the tip a drill-bit configuration. With the wedges retracted, the catheter is atraumatically advanced through a 6-French sheath to the lesion's proximal cap; then, the wedges are deployed, and the tip is spun to traverse the cap. The remainder of the lesion may be crossed with the wedges retracted or extended as necessary. The CONNECT study of 84 PAD patients reported 89% primary successful recanalization with four perforations sealed by prolonged balloon inflation. 22 Avinger's Ocelot™ catheter adds optical coherence tomography (OCT) to the Wildcat™ design. A study of 33 patients with superficial femoral artery CTOs reported 94% primary and 100% secondary successful recanalization with decreased procedure time and contrast dose when compared with data from Wildcat™. 23 Avinger's 5-French, 150 cm Kittycat™ with a shapeable tip is marketed for diminutive vasculature and infrapopliteal lesions.
The TruePath™ device (Boston Scientific) consists of a 0.018 in. (0.46 mm) wire with a diamond-coated tip that rotates at 13,000 rpm. Sized like a guidewire, TruePath™ is compatible with almost any vascular access sheath, and its 165 cm length and shapeable tip permits access to infrapopliteal lesions. In the ReOpen study of 85 PAD patients, lesions were crossed in 80% of patients, with distal guidewire access achieved in 77%; only one perforation was reported. 24
The Viance™ blunt microdissection catheter (Covidien) has a coiled, multiwire shaft and a rounded 3-French tip. Operated through a 5-French sheath and over a guidewire, Viance™ is rapidly rotated manually using a torque device as the catheter tip is pushed along a luminal or subintimal course. A retrospective registry analysis of 58 PAD patients treated with Viance™ reported lesion crossing in 88% of patients and procedural success in 86%, but 52% of lesions received stents. 25 Target vessel repeat revascularization or limb amputation was 5.2% at 30 days.
The Frontrunner XP™ blunt microdissection catheter (Cordis) has a braided shaft that may be shaped distally and a blunt actuating tip that is controlled by a mechanical handle and torque device. Frontrunner™ is operated through a 6-French sheath without a guidewire. In addition, Cordis’ Micro Guide™ hydrophilic catheter may be employed to provide additional support to the Frontrunner™ and to facilitate guidewire placement after the lesion in crossed. A retrospective study of 22 CLI patients treated with Frontrunner™ after failure of traditional guidewire crossing reported successful distal lumen guidewire access in 21 patients without reported complications. 26
Several crossing devices are currently undergoing clinical investigation. The TOTAL across™ catheter (Medtronic) is a stainless steel tube with a 2-French tapered tip. The manufacturer states that the steel construction provides maximum radioopacity and “pushability,” while the tapered tip complements a guidewire in pushing through tight lesions. The PowerWire Radiofrequency Guidewire™ (Baylis), initially used for chronic venous occlusions, boasts an atraumatic tip that delivers radio frequency energy to vaporize a channel through CTOs.
Luminal Reentry Devices
When a guidewire or crossing device traverses a CTO via a subintimal course, a luminal reentry device may facilitate deployment of a guidewire in the distal vessel lumen.
The Outback LTD™ device (Cordis) consists of a soft-tipped, hydrophilic, 6-French catheter with a side hole to allow the deployment of a 22 gage nitinol cannula (Fig. 3). Radioopaque orientation markers allow the alignment of the side hole toward the true lumen. Once the cannula is deployed, a guidewire is advanced into the distal vessel. A 2013 trial randomized 52 CLI patients to subintimal intervention with either manual reentry or Outback LTD™-guided reentry. Reentry was achieved in 42% of the 26 manual reentry patients and in 100% of the 26 Outback LTD™ patients, who also had shorter procedure and fluoroscopy times. 27 However, a 2011 retrospective review of 52 PAD patients including 18 with CLI reported procedural success in only 65% of patients, citing calcification as the primary predictor of failure. 28

Outback® LTD® Re-Entry Catheter with side hole, allowing deployment of nitinol cannula. 29 Courtesy of Cordis Corporation. Outback® LTD® Re-Entry Catheter is a trademark of Cordis Corporation.
The Offroad™ reentry catheter system (Boston Scientific) consists of a tipless conical balloon to anchor the over-the-wire, 6-French catheter system and a side hole through which a flexible, needle-tipped microcatheter is advanced into the distal true lumen to facilitate guidewire access. A platinum–iridium marker facilitates visualization of the needle exit side hole. The multicenter Re-ROUTE trial of 92 PAD patients reported technical success in 85% of patients with three adverse events at 30 days, all peripheral emboli. 30
The Pioneer Plus™ catheter (Volcano) offers intravascular ultrasound (IVUS) guidance for luminal reentry. The six-IVUS French catheter system deploys a 24 gage nitinol needle to an adjustable depth of 3, 5, or 7 mm via a side hole. A guidewire is then advanced into the distal true lumen.
Designed to pair with the Viance™ catheter, the Enteer™ reentry device (Covidien) consists of a catheter with a flat balloon that self-orients parallel to the vessel and a guidewire. Through an exit port in the catheter perpendicular to the orientation balloon, the angled reentry probe at the tip of the Enteer™ guidewire is advanced into the true lumen.
Discussion
Published studies of lesion crossing devices in CLI have been small, few clinical trials have been conducted, and study criteria and endpoints have been inconsistent. In our experience, each device has a learning curve, and success rates improve with increasing procedural volume. In addition, certain devices may penetrate specific lesion types better: atherectomy and crossing devices penetrate heavily calcified lesions, and reentry devices circumnavigate very long lesions. Long, calcified chronic total occlusions represent the most technically challenging lesion subset that endovascular specialists face. The above devices have improved success rates and enabled treatment of a number of patients who were previously unapproachable with traditional endovascular techniques.
No single, perfect device suits all patients or navigates every challenging lesion. Treatment of patients and specific lesions should be individualized to yield the best results.
Author Contributions
Conceived and designed the experiments: AMG, FH, CM. Analyzed the data: AMG, FH, CM. Wrote the first draft of the manuscript: AMG. Contributed to the writing of the manuscript: AMG, FH, CM. Agree with manuscript results and conclusions: AMG, FH, CM. Jointly developed the structure and arguments for the paper: AMG, FH, CM. Made critical revisions and approved final version: AMG, FH, CM. All authors reviewed and approved of the final manuscript.