
Abstract
Training medical students to understand the effects of culture and marginalization on health outcomes is important to the future health of increasingly diverse populations. We devised and evaluated a short training module on working with diversity to challenge students’ thinking about the role of both patient and practitioner culture in health outcomes. The workshop combined didactic teaching about culture as a social determinant of health using the cultural humility model, interactive exercises, and applied theater techniques. We evaluated changes in the students’ perceptions and attitudes over time using the Reaction to Diversity Inventory. There was initial significant improvement. Women and students with no past diversity training responded best. However, scores largely reverted to baseline over 12 months.
Background
In 2012, the Sydney Medical School introduced a Longitudinal Patient Partnership Program called Integrated Population Medicine (IPM). IPM aimed to expose senior medical students in the final two clinical years (Stage 3) of a four-year postgraduate entry program to the intersection of population medicine principles and clinical practice through longitudinal partnering with people living with chronic disease and disability.
In IPM, each student was required to recruit a person living with a chronic disease or disability and meet with them over a period of around 14 months. Through a series of meetings with their patient-partner, students then reflected on the patient's healthcare experience in the broader context of their lives and communities outside the hospital environment through a social determinants lens.
The details of the IPM curriculum are reported elsewhere; 1 however, helping students to understand the effects of culture and marginalization on health outcomes was an important aim of the program. Students were encouraged to choose their own patient-partners who were from different cultural backgrounds to their own. Although Australia is one of the most multicultural countries in the world and more than one in four Australians are born elsewhere, specific training in working effectively with diversity was not then part of the Sydney Medical School curriculum.
Cultural competence is increasingly included in medical curricula in attempts to counter health inequities experienced by marginalized populations. However, critics of the teachability and assessability of these concepts suggest that the training often risks reinforcing negative stereotypes and positions learners as a homogenous in group learning about a foreign other.2–4
To challenge students’ thinking about the role of both patient and practitioner culture in health outcomes, we developed and evaluated a two-hour interactive workshop on working effectively with cultural diversity. Defining culture broadly, we wanted students to think about their role in effective healthcare communication with diverse populations.
In this paper, we report the results of the evaluation of the student workshop, using a validated quantitative instrument called the Reaction to Diversity Inventory (RTDI) developed by De Meuse and Hostager. 5 With this, we aimed to see if students’ perceptions and attitudes toward diversity changed over time.
Methods
Workshop structure
The workshops consisted of two parts. Part A was a didactic, theoretical component giving an overview of the concept of culture and why it matters in health care. This discussion was based on the cultural humility model of Tervalon and Murray-García, 6 which required students to first consider their own identity and become aware of some of the barriers that identity may create in communicating effectively with others. A range of interactive exercises was used to help students broaden their understanding of their own identity through exploring concepts such as the meaning of diversity and the complexity of personal cultural identity, implicit (or innocuous bias), the role of stereotypes, and the impact of stigma and discrimination (Table 1).
Workshop structure.

In Part B, we borrowed the “forum theater” or “theater of the oppressed” methodology of Brazilian director, Augusto Boal,7,8 and ideas from discussions with Performing Medicine in London. 9
By adding the forum theater component to the workshop activity, we aimed to engage students in learning that was both patient centered and democratic. Boals’ intent for his theater of the oppressed was not simply to provide a forum for the discussion of oppression, but to free the audience from the traditional constraints or oppression of the theater itself and turn them into spect-actors. The pedagogical basis for forum theater is Paulo Freire's model of problem-posing dialog in which a continual exchange occurs between teacher (who also learns) and learners (who also teaches). 8
In our workshop, initial action was played out by the actor and a doctor facilitator (KDI), and students were invited to stop the action, intervene, make, and try suggestions for better communication until a satisfactory communication that identified the patient's priorities and values without making assumptions was reached.
We employed an actor from the Pam McLean Centre trained in simulated medical encounters (https://pammclean-centre.org/) as the patient in a scripted consultation in which a female, sexual minority patient was concerned about possible stigma related to hepatitis C testing. 10 This scenario (Appendix 1) highlighted the potential impact of making assumptions about cultural identity and values on health outcomes. This segment was facilitated by an academic (PD) skilled in Boal's technique.
Attendance at the workshop was compulsory for all students entering Stage 3 (Year 3) of the Sydney Medical Program in January 2012. The workshop was held on both days of the compulsory on-campus orientation session for Stage 3 students. As our cohort was very large (280 students), the cohort was split into four. Two groups of students attended the workshop on day 1 and the remaining two groups on day 2. On each day, one group did Part A followed by Part B, and the other group did Part B followed by Part A.
The evaluation
The evaluation comprised a series of three paper-based surveys and one online survey each incorporating De Meuse and Hostager's validated RTDI 11 and some basic demographic information.
De Meuse and Hostager came from a human resources background and wanted to create a nonthreatening “objective, quantifiable assessment” that would measure an individual's overall orientation toward diversity in the workplace as well as his or her specific emotional, cognitive, and behavioral reactions to it. One advantage of the RTDI compared to more traditional questionnaire-style tools is that it does not force participants to respond to each item but only to select those items that associate with workplace diversity.
De Meuse and Hostager 5 conceptualized diversity in a general way. Their aim was to create a conceptual framework that would capture various aspects of diversity and be useful in tailoring the design and delivery of diversity training to the unique views held by the members of organizations. 11
The RTDI (Table 2) is a list of 70 words, presented in random order, each depicting a positive or negative response to diversity on one of the five dimensions. The five dimensions are as follows:
Emotional reactions: the individual's gut feeling about diversity in general.
Judgments: the individual's beliefs about diversity in principle (eg, whether it is good or bad).
Behavioral reactions: the individual's planned verbal and nonverbal actions in response to workplace diversity.
Personal consequences: the person's views on how diversity affects them directly.
Organizational outcomes: the person's views on how diversity affects the organization as a whole. 5
RTDI word list showing subcategories, after De Meuse and Hostager. 5
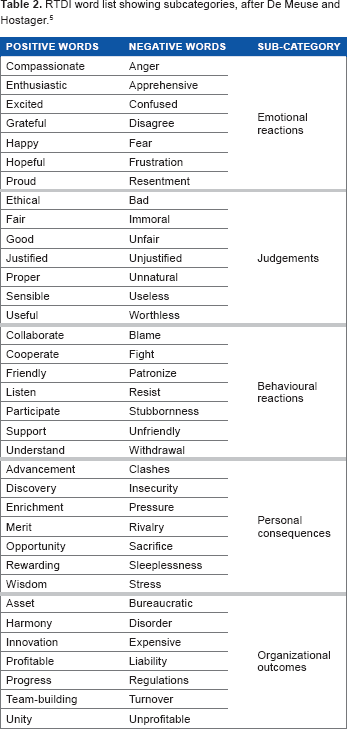
Once the participant has chosen all the words they consider applicable, a summary score identifying their overall orientation to workplace diversity is calculated. All positive words have a value of +1, and all negative words have a value of -1, so individual summary scores can range from -35 to +35. Circling all 70 words resulted in a score of zero. Scoring is repeated in each of the five dimensions, where scores may range from -7 to +7. 5
All students in Stage 3 Year 3 attending the workshop (276) were invited to complete the pre- and postworkshop evaluation (surveys 1 and 2). Students completed surveys before and after the workshop (surveys 1 and 2). All students who completed survey 1 (preworkshop) were subsequently invited to complete surveys 3 and 4 at two subsequent time points over the 18 months of the program, in December 2012 (survey 3) and in June 2013 (survey 4).
Survey 3 was distributed online using LimeSurvey and students were sent a link to the survey. Only 49 (18.1%) students completed this survey. In order to improve the response rate for survey 4, students were again given a paper survey to complete at the time of a compulsory examination. A total of 176 (65.9%) students completed survey 4. Due to the low response rate in survey 3, these data were excluded from the final analysis (Table 3).
Survey response rates over time and percentage of total cohort (n = 270).

In a separate, parallel evaluation of the experience of patient-partners subsequently recruited by this cohort (to be reported elsewhere), patient-partners were sent extensive paper-based surveys at the same time points. These surveys included the questions listed in Table 4 to assess how well the students respected their cultural and religious beliefs in an attempt to gage how well students applied this training in practice.
Excerpted relevant questions from patient-partner evaluation questions.

Statistical analysis
Comparisons were made between survey completers and noncompleters on age using independent samples t-tests and on categorical variables using chi-square analyses (or the Fisher's exact test when cell sizes were small). Changes in RTDI total and subscale scores from baseline to post-training, from post-training to follow-up, and from baseline to follow-up were examined using paired samples t-tests. The subscale scores were not normally distributed. Consequently, the analyses were originally conducted using nonparametric analyses (Wilcoxon signed-rank tests). However, there were instances where the median score did not differ across time points, even though the Wilcoxon signed-rank test indicated a statistically significant difference over time. We repeated the analyses using paired samples t-tests. The results were largely the same, with the paired samples t-tests being slightly more conservative. The paired sample t-tests enabled reporting of means rather than medians, which we felt made it easier for the reader to see the direction of the change in RTDI scores and subscale scores over time. These analyses were repeated, stratified by gender and prior diversity training. All analyses were conducted using SPSS version 22.0, 12 and alpha was set at P < 0.05. This protocol was approved by the University of Sydney Human Research Ethics Committee: Approval number 14341 in accordance with the principles of the Declaration of Helsinki. Participants gave their informed consent to participate in the research.
Results
Demographics
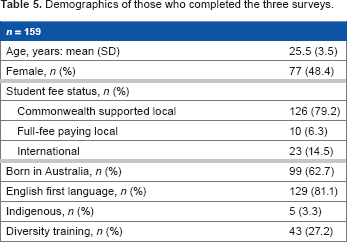
Of the original 270 students attending the workshop, we obtained a total of 159 (59.9%) usable matched RTDIs from students who completed surveys 1, 2, and 4. The mean age of these students was 25.5 years, and the majority were local students with fee support from the Commonwealth Government (79.2%), who were born in Australia (62.7%) and had English as their first language (81.1%). Only 27.2% of this group had had previous diversity training (Table 5).
Demographics of those who completed the three surveys.
We compared the students who completed all three reported surveys with those who did not and found that the completers were more likely to be slightly younger and born in Australia than the overall student cohort (Table 6).
demographics of completers versus noncompleters.

Indigenous here includes aboriginal or non-Australian indigenous.
RTDI scores
The overall RTDI summary scores suggest a significant positive impact (P < 0.001) of the workshop measured by the difference in baseline and postworkshop scores. There was a positive trend in all five subcategories post-training and a significant improvement in two of the subcategories, such as judgments and personal consequences, immediately after the workshop (Table 7).
Mean RTDI summary scores with standard deviations–- whole group.

Significant increase from baseline to post-training.
Significant decrease from post-training to follow-up.
Significant decrease from baseline to follow-up (P = 0.019).
Female students showed more positive shift after the workshop than male students (Table 8). This gender difference also carried through most of the subcategories, with personal judgment and behavioral reaction in particular showing a significant increase compared to male students. However, in the case of personal concern, male students moved significantly more toward positive after the workshop than female students.
Mean RTDI scores by gender (SD).

Significant increase from baseline to post-training.
Significant decrease from post-training to follow-up.
Significant decrease from baseline to follow-up.
A similar pattern emerged between those with no previous exposure to diversity training compared to those who had previously experienced some form of cultural diversity training, with students without previous exposure improving significantly more in total scores after the workshop and improving in all subcategories, but significantly in personal judgment, behavioral reaction, and personal consequences (Table 9).
Mean RTDI scores by prior experience of diversity training (SD).

Significant increase from baseline to post-training.
Significant decrease from post-training to follow-up.
Significant decrease from baseline to follow-up.
This initial improvement was not sustained over time. There was a significant decrease between post-training and follow-up scores for the whole group in the total score, emotional reactions, behavioral reactions, and personal consequences. However, scores at follow-up fell significantly below baseline only in the subcategory of emotional reactions.
A similar pattern emerged again when looking at gender and previous exposure to diversity training. The emotional reactions scores of the female participants and those with no past training also fell below baseline at follow-up.
Discussion
Our data suggest that a short but engaging diversity workshop, based on a cultural humility framework and allowing for student input, can positively influence the perceptions and attitudes of medical students to work with diversity. In particular, the significant improvement in judgments and personal consequences immediately after the workshop suggests that students felt more positive in their belief that diversity was a good thing and that they had a positive role to play in it.
The low scores and steadiness of the organizational outcomes category across the three surveys may suggest that students do not yet feel they are in a professional position in which they have any real sense of the impact of diversity on the operational activities of their healthcare workplace, nor any influence on how that may impact, which this category is meant to reflect.
Although this initial improvement in the student data was not maintained quantitatively over time, in the patient evaluation there was a significant improvement over time to the question with respect to cultural background and beliefs (Personal communication/publication pending). The patient-partners also became increasingly positive about students’ enacted respect for their religious beliefs and cultural backgrounds in their separate evaluation encourages us to suggest that students enacted the workshops’ key message of the link between respect for diversity, professionalism in practice, and health outcomes.
The workshop's focus on exploring the complexity of personal identity and finding points of sameness between people rather than difference through a range of different activities may have contributed to the improvement in overall scores by helping create what Betancourt and Green 13 described as “a culturally competent biosphere”. These authors suggested that a multifaceted educational intervention has the best chance of having an impact on healthcare outcomes if it includes a patient-component and practice-enabling strategies.
This is a key component of the cultural humility framework. Tervalon and Murray-García 6 defined cultural humility as a practice that “incorporates a lifelong commitment to self-evaluation and critique, to redressing the power imbalances in the physician-patient dynamic, and to developing mutually beneficial and non-paternalistic partnerships with communities on behalf of individuals and defined populations.” In order to achieve that, first students must be able to examine their own cultural identities and the culture of biomedicine and critically reflect on the ways in which these influence their behaviors and attitudes. They must also deepen their understanding of culture beyond a set of stereotypes and realize that culture is complex and ever-changing. 14
However, this difficult work of maintaining respect for patients whose cultural beliefs and behaviors are antithetical to one's own is rarely supported by either the formal or the hidden curriculum of the traditional medical school. Wear 15 stated that this process of unlearning one's prejudices is “lifelong, always unfinished work”. Without doubt, this brief exposure to the concepts of cultural humility was, at the time, novel in the whole of the Sydney Medical School curriculum. Subsequently, it has also been introduced as a seminar in the early weeks of the first year. However, this remains a tiny drop in a vast ocean of hard-held beliefs about the roles of doctors and patients and embedded power structures in medical education. It may be that ongoing exposure to this cultural reality also reduced students’ positive reactions to diversity.
Applied theater techniques have been employed in many aspects of medical education16–19 and students have found them to be particularly helpful for learning to “act like a doctor” and to develop a broader awareness of others. 9 Forum theater in particular provides an excellent, interactive framework for the exploration of challenging situations 20 and has been successfully used in the teaching of professionalism. 16 Acting offers creative means to address the complexities of interpersonal relations in modern healthcare workplaces where most communication is unscripted. Actors understand that improvisation is grounded in rules that can be taught. 21
The theatrical debate of forum theater allows participants to observe, comment on, and intervene in scenarios that dramatize oppressive social situations, examining the scope for individual or collective action. In India, forum theater has helped medical students re-humanize and “be what I was, and what I always wanted to be”, despite social hierarchies. 20
Bleakley 22 suggested that “learning is best realised as a dynamic, complex, adaptive system in which high levels of uncertainty must be tolerated within shifting networks of activity.” Certainly, forum theater lends itself well as a technique through which to explore the uncertainties and nuances of working with diversity.
In retrospect, a separate qualitative evaluation of the workshop and particularly the forum theater component may have provided greater insight into how students engaged with various components of the workshop and how they applied what they learned in various settings.
The greater improvement in women over men after this brief intervention is consistent with social identity theory, which suggests that women's historical membership of a [gender] minority should result in a greater tendency for feelings of solidarity with other minorities and consequently should produce more positive perceptions of diversity training. 23 Women also tend to be more focused on procedural justice, which requires rules to be followed impartially and consistently applied in order to generate an unbiased decision. 24
Our data also suggest that exposing medical students with no prior training in working with diversity to diversity training has important consequences to their ability to work with diverse populations in future. Other studies have also confirmed that exposure to cross-cultural skills training is associated with increased preparedness to care for diverse patient populations. 25
A decline in positivity in the period after the workshop may reflect personal and systemic challenges participants experienced in attempting to apply new learning, an example of Maslow et al's cycle of learning in practice. 26
According to Maslow et al's theory, there are four stages of maturation of learner competency. The first stage is unconscious incompetence in which the student does not recognize the knowledge they are lacking. Not until the student has been presented with information that highlights his or her lack of knowledge, does this deficit become obvious and the desire to address the deficiency develop (conscious incompetence). Through continual practice, the students face new challenges that demand further new learning (conscious competence) until the skill becomes second nature (unconscious competence).
This study has several limitations, in particular, the lack of a control group and the smaller number of students who completed all three surveys. Also, those who did complete all three were more likely to be younger and Australian born. It is possible that older students and those from more diverse backgrounds could have different reactions to diversity that are not captured in these data.
Future research could further analyze the RTDI data–- especially the subscores–-to create individual profiles for reactions to diversity in order to develop more targeted curriculum interventions. For example, while a student may believe that diversity is good in principle (a high subscore on the Judgment dimension), he or she may also believe that diversity has a negative effect on individuals and organizations (low subscore on the personal consequences and organizational outcomes dimensions). The summary scores also lend themselves to identifying those who are extremely positive about diversity versus those who are balanced or extremely negative. It could be that those on either extremity have somewhat unrealistic concepts of diversity, and this too could be used to better target curriculum interventions. 12
Conclusion
The workshop we developed demonstrated an immediate quantitative improvement in perceptions and attitudes around working with diversity in our student cohort, especially in women and students with no previous training in diversity. Further analysis of this data or application of the RTDI may provide insights into more targeted curriculum interventions for teaching medical students about cultural diversity.
Author Contributions
Conceived and designed the experiments: KDI and PD. Analyzed the data: KDI and GL. Wrote the first draft of the manuscript: KDI and GL. Contributed to the writing of the manuscript: KDI and GL. Agree with manuscript results and conclusions: KDI, PD and GL. Jointly developed the structure and arguments for the paper: KDI, PD and GL. Made critical revisions and approved final version: KDI, PD and GL. All authors reviewed and approved of the final manuscript.