
Abstract
There is currently no universally accepted core collection of competencies or medical education material for medical students. Individual medical schools create their own competencies and set of educational material using a variety of approaches.
What has resulted is a medical education system wherein medical students are trained without any burden of proof that they are indeed competent in agreed upon areas of knowledge, skills, attitudes and behaviors befit of a graduating medical student.
In fact, the only uniform assurance a member of the public in the United States can have for a graduating allopathic medical student is that the student has successfully passed USMLE Step 1 and 2 by correctly answering a rumored 55–65% of questions correctly (yes, that is an F) and that they have maintained at least a “C” average or “Pass” equivalent in all of their medical school courses.
This article discusses these inadequacies within the current medical education system, and the need to standardize the competencies and curricula for all medical schools through a narrative disclosing this author's experience with trying to initiate such a movement at his own medical school.
Heavy Appetizers
In the 1980s, Reese's ran an ad where two individuals were walking down perpendicular streets. One was eating a chocolate bar, and the other was carrying a tub of peanut butter. As fate would have it, when they turned their respective corners, the chocolate found its way into the peanut butter, and a surprisingly sweet and tasty product was created.
As a young child, I marveled at the serendipity. Turns out, Milton Hershey had created the product with the help of his dairy farmer and shipping foreman H.B. Reese all the way back in 1928. Why was a concept conceived so long ago, still being discussed? Sometimes, I realized, you need to tell the story again in a different way.
In 2007, in my role as Associate Dean for Medical Education at Marshall University Joan C. Edwards School of Medicine, I proposed to the curriculum committee that we change from a traditional-based to a systems-based curriculum. Simultaneously, I suggested we combine our notes into one set of documents to address the overall content quality and to satisfy Liaison Committee on Medical Education (LCME) requirements such as “gaps and redundancies.”
This idea for me was chocolate, and I couldn't wait for everyone else to have a taste.
My preparation for these proposals was not trivial. I had studied dozens of medical school curricula, read and evaluated scores of curriculum change articles, poured through all existing Association of American Medical Colleges (AAMC) literature on the subject, and worked with several medical educators, namely an administrative and basic science team from the Morsani College of Medicine in South Florida. And as if that were not enough, I used James Kouzes and Barry Posner's Leadership Challenge Workbook as my change guide in order to stay focused on the task at hand.
The initial water cooler reactions, were apparently, not very positive. The plan involved, after all, a formidable request … change. I knew I had to bring something extra special to the table. My passion for this project had to become contagious.
The opening meeting was met with a resounding thud. It was too much, too fast. Undaunted, I pressed forward. Meeting after meeting. Discussion after discussion. Month after month. Persevering through my checklist. And finally, in the fall of 2009, to the credit of our curriculum committee chair, members, and faculty, a hybrid systems-based curriculum was launched (and still survives today).
Some Salad
The integration of our teaching content idea, however, had long since melted on the ground
I brought the issue of integrating our notes together repeatedly at subsequent curriculum committee meetings over the next several years. The issues of territoriality, intellectual property, and academic freedom were prevalent. I was becoming frustrated.
Despite the integration into systems, there would be no integration of content. While some committee members seemed to be leaning towards the concept, the ability to get everyone on board did not seem realistic. However, there was an increase in the amount of cross-talk among disciplines, which in some areas, did vastly improve the degree of integration within the content.
In 2012, with the assistance of Brian Dzwonek, EdD, a greatly needed hire in the medical education office, we began to revitalize the concept of note integration based on Brian's experience at the Duke-NUS program in Singapore. We toyed around with multiple ideas and chose to pilot the concept using iBooks Author. What followed was an unmitigated disaster.
Using two graphic artists, we attempted to convert an incalculable number of existing PowerPoints, word documents, and PDFs into one seamless, integrated document using our existing medical educational material. Imagine inheriting an empty Walmart Supercenter and being told to stock it using items found at local rummage sales.
It was an impossible task. Many items were outdated and needed thrown out. There were several items we had too many of and even more that were missing all together. Numerous items did not seem relevant. Countless items were missing parts. After a few months, we scrapped the process.
And then, finally, the peanut butter came around the corner
I recalled a talk to a group of medical educators given in 2009 by John Prescott, MD, Chief Academic Officer for the AAMC, in which he said, “Sooner or later someone is going to take the curriculum, just like they took a look at the human genome and mapped it. Then the curriculum is going to be sliced and diced and put into discrete packets and delivered in a way that is personalized.” This for me asked the question, “Why do we not have a national medical curriculum?”
A surprisingly sweet and tasty product was about to be created
After a generous invitation from Dr Prescott and his team, we descended on the AAMC headquarters in February 2013. We were finally able to pitch our idea at the national level. The response was polite but reserved. The elephant in the room unfortunately, appeared very similar to the one sitting in on our curriculum committee meetings.
“How would we get all of the medical schools to agree on something like this?” The take home message for me on our ride back to West Virginia was that this idea was too formidable and forceful a proposition to come from the AAMC. They were a medical school support service, and certainly not curriculum dictators.
A few months after the meeting with the AAMC, our new Dean paid me the best visit I have received as a faculty member. We had completed our interim LCME probation visit and were simply waiting on their vote to remove that pejorative status from our school. He suggested I go on sabbatical to pursue the integrated note project. I smiled.
The Main Course
On July 1, 2013, the creation of Universal Notes for Medical Students officially began. We had learned from our earlier experience that using existing medical education materials was beyond problematic. There was no other option but to start from scratch.
The first ingredient, we realized, had to be medical students. If this was not their project as well, it was destined to fail. It was finally time that someone asked the students, “What would you like your medical content to look like?”
Soon after, www.myuniversalnotes.com was launched. The Website directed students to select a prepopulated list of diseases, drugs, and bugs that was created using content outlines, objectives, and competencies garnered from existing national groups such as United States Medical Licensing Exam (USMLE), Group for Research in Pathology Education, and Council on Medical Student Education in Pediatrics (see Table 1).
Sources of objectives.
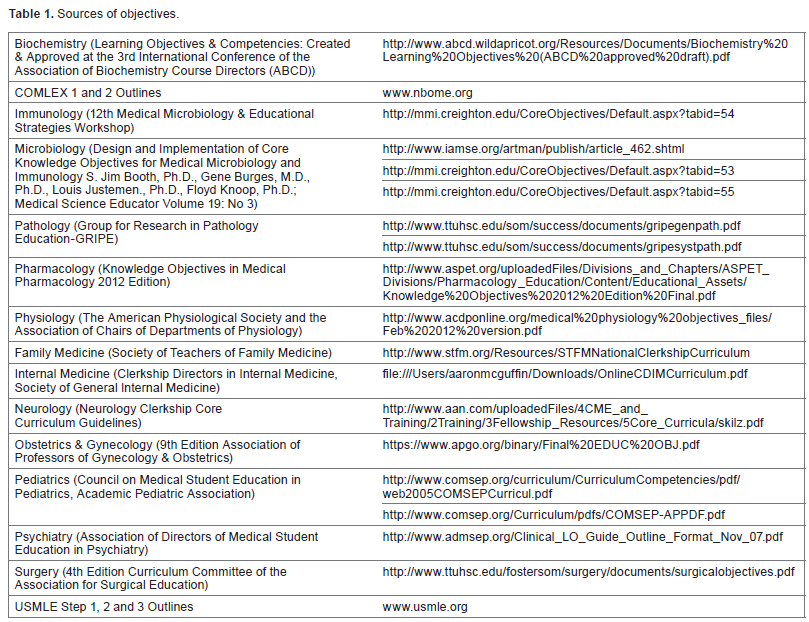
Once the student selected a topic of interest, they would then write the content important to that topic. They were instructed to write each section in a manner in which they as medical students could understand and learn most effectively.
However, we did give them some structure. The diseases and bugs had to be organized according to the following headings: Introduction, History of Present illness, Physical Exam, Labs and Diagnostics, Management Plan, and Discussion. This format helped create uniformity and described the disease or bug from the perspective in which a physician experiences the patient encounter.
Drugs were standardized with: Indications, Mechanism of Action, and Side Effects, the main items a medical student really needs to know.
In addition, students could upload charts, graphs, or images they felt were relevant to understand the material. We would then use those as a template to recreate the best rendition possible, referencing the student's text to the de novo– created schematic.
For the content review process, we cherry-picked some of the best and brightest from the American Medical Association (AMA) student association to serve as student editors. Each student submission was directly e-mailed to the five student editors as well as myself for content review. The editors were marvelously nitpicky and helped mold the submission into a concise but educationally powerful summary of the topic.
Another Reese's cup had been formed
The response from recruitment of the student authors was slow but steady, and over the course of only four months, we had received and edited enough material to call it a book. All told, we had amassed nearly 700 topics using close to 50 medical students from 11 different medical schools, including schools in Canada and the Caribbean.
In addition to the main topics, the book contains full sections on history taking, the physical exam, counseling, preventative health, ethics, biostatistics and epidemiology, the healthcare system, and more, with additional “quasi-medical” topics added every revision.
The feedback from students using the e-book was encouraging. The structure helped them to understand the disease from beginning to end, in ways textbooks and lectures seldom do. In most cases, it was not that Universal Notes had added anything new from a content perspective, but had simply pulled all of the relevant content together in one place to paint a big picture for them. The secret, perhaps, was in the organization of the material.
The content of the e-book is, in many regards, reviewed continuously. With hundreds of students currently using the e-book, their feedback serves as excellent quality control. Medical students are not bashful about demanding quality, and we love that about them.
An important aspect of the content in Universal Notes is that it is in no way designed to be a Wikipedia or an UpTo-Date. It is designed to include all material deemed relevant for
Paying the Bill
So what does all of this really mean? Can an e-book meta-morph itself into an e-curriculum that can be used by medical schools around the world? We certainly think so and are pressing forward each day to do it.
The creation of Universal Notes begs several questions.
Why do we not already have a universal or at least national curriculum?
What would be the advantages and disadvantages?
Could this curriculum serve as a template from which we could overlap the curricula of other health care professions?
How much money do we currently waste with the paper versions of our traditional curricula?
How much time do we waste employing basic scientists and clinicians to teach material that could be self-taught and more effectively learned in a small group setting?
What should be the role of the AMA and AAMC in pursuing such a concept?
What else currently exists?
What would the international community think of such as movement?
These questions will be addressed in Parts II and III of this series on creating a Universal Curriculum.
Author Contributions
Conceived the concepts: AMM. Wrote the first draft of the manuscript: AMM. Made critical revisions: AMM. The author reviewed and approved of the final manuscript.