
Abstract
The etiology and pathophysiology of posttraumatic stress disorder (PTSD) remains poorly understood. The nutritional deficiencies associated with the altered metabolic processes of PTSD have not previously been studied in detail. This pilot study measured the reduction in symptoms in 21 military veterans reporting moderate to severe symptoms associated with PTSD. Two amino acid-based medical foods specifically formulated with biogenic amines and other nutrients were administered to study subjects targeting specific neurotransmitter deficiencies resulting from altered metabolic activity associated with PTSD. This study included the Physician Checklist – Military (PCL-M), Short Form General Health Survey (SF-36), and Epworth Sleepiness Scale to measure the change in each subject's score after 30 days of administration. An average decrease of 17 points was seen in the PCL-M, indicating a reduction in PTSD symptoms (P < 0.001). The mental health component of the SF-36 showed an average 57% increase in the subjects’ mental health rating (P < 0.001). The results of this initial study demonstrate that addressing the increased dietary requirements of PTSD can improve symptoms of the disease while eliminating significant side effects. A larger, double-blind, randomized, placebo-controlled trial is warranted.
Introduction
Combat-related illnesses include posttraumatic stress disorder (PTSD), Gulf War Illness (GWI), and other symptoms that fall under the rubric of “postdeployment multisymptom disorder and related syndromes.”1,2 While similar syndromes have been reported since the Civil War, the etiology and pathophysiology of these conditions remain poorly understood.1,3 Thus far, treatments for these syndromes have been insufficient, due to limited efficacy, high cost, and low sustainability.4–7
Recently, attention has been directed to abnormalities of the autonomic nervous system, particularly the parasympathetic autonomic nervous system.8–12 In both PTSD and GWI, there is a blunting of total autonomic activity, marked in particular by a reduction of parasympathetic activity. This imbalance leads to an increase of sympathetic nervous system symptoms including anxiety, rapid heartbeat, panic spells, and amplified sweating. Parasympathetic suppression also manifests as a failure to sleep, abnormal dream patterns, and memory disturbances. 13 There is an emerging consensus that sleep disturbance may be a core feature of PTSD. 14
Alternatives to therapy and psychiatric medication are essential for treating combat personnel. Active service and military veterans are often reluctant to seek treatment for PTSD symptoms because of the perceived stigma associated with a psychiatric diagnosis. Sentra AM® (acetyl L-carnitine HCl, choline bitartrate, L-glutamic acid) and Sentra PM® (acetyl L-carnitine HCl, choline bitartrate, 5-Hydroxytryptophan, L-glutamic acid) are specially formulated medical foods that influence the production and absorption of neurotransmitters essential to autonomic nervous system function.15,16 They may be particularly effective at targeting symptoms of PTSD and GWI. We report the results of a pilot study exploring the use of these medical foods to ameliorate symptoms of PTSD that are strongly influenced by autonomic nervous system function. We will refer to these amino acid formulations by brand name as there is no generic name or version available.
Materials and Methods
This was a single-arm, open-label study, whose aim was to collect pilot data concerning the efficacy and side effect profile of Sentra AM® and Sentra PM®. Subjects were veterans and active duty military personnel, who were recruited via clinician referral and social networking sites between August and December of 2011. Prospective subjects were directed to a secure, Health Insurance Portability and Accountability Act (HIPAA)–compliant Web portal (http://tmedpharma.com/app/survey/ptsd_GWF001) where they completed an initial screening questionnaire that verified military status, deployment locations, current PTSD symptoms, and presence of suicidal ideation. Screening results were reviewed by study doctors, including a psychiatrist with experience in assessing PTSD and suicidal ideation. If significant suicidal ideation was present, as measured by the Columbia-Suicide Severity Rating Scale (C-SSRS), subjects were contacted and directed to seek immediate help from their current clinician or caregiver.
Eligible subjects were men and nonpregnant, nonlactating women, between the ages of 18–75, with a history of military deployment in a combat theatre, and symptoms of PTSD as rated on the Primary Care PTSD Screen (PC-PTSD). The PC-PTSD is a four-item screen that was designed for use in primary care settings and is currently used to screen for PTSD within the United States Department of Veterans Affairs. Subjects were included if they endorsed three or more items. Subjects were excluded if they were pregnant, breastfeeding, or had significant suicidal ideation as measured by the C-SSRS. Once subjects were accepted into the study, informed consent was obtained via ground mail or electronically through the HIPAA-compliant Web Portal. The study protocol was published on www.clinicaltrials.gov in compliance with Federal registration regulations. All elements of the study protocol were approved by Aspire IRB, an independent institutional review board. The research was conducted in accordance with the principles of the Declaration of Helsinki.
After reviewing and completing the informed consent document, subjects completed baseline questionnaires including the Physician Checklist-Military (PCL-M),17–19 Short Form General Health Survey (SF-36),20–23 Epworth Sleepiness Scale (ESS),24,25 and Cognitive Emotion Regulation Questionnaire Short (CERQ-short). 26 The PCL is used for diagnosing PTSD, screening individuals for PTSD, and monitoring symptom change during and after treatment. The PCL-M asks about symptoms in response to “stressful military experiences.” It is often used with active service members and Veterans. The SF-36, a widely used general health profile questionnaire with established reliability and validity, assesses health-related quality of life. 27 The SF-36 has demonstrated sensitivity to health differences in the general population within various scales. These scales include (1) limitations in physical functioning activities because of health, (2) limitations in social functioning activities because of physical or emotional problems, (3) limitations in role activities because of physical health problems, (4) limitations in role activities because of emotional problems, (5) bodily pain, (6) general mental health, (7) vitality, and (8) general health perceptions. The SF-36 is frequently used to assess the status of military patients with PTSD. The ESS is a seven-question patient-derived sleep questionnaire that looks at the quality and quantity of sleep. It is utilized to determine the level of daytime sleepiness. A score of 10 or more is considered sleepy. This ESS score is frequently used to assess sleep disorders in patients with PTSD. The CERQ was developed to fulfill an omnipresent need for a questionnaire in order to identify cognitive coping strategies someone uses after experiencing negative incidents or situations.
Subjects then received the medical foods consisting of one bottle (60 capsules) of Sentra AM® and one bottle (60 capsules) of Sentra PM® with all relevant instructions pertaining to use and warnings via overnight mail. The medical foods used in the study were prescribed under the supervision of the study physicians, who reviewed the medical history forms of all the subjects and were on call to answer any questions or address any concerns either before beginning treatment or during treatment. Subjects were instructed to take two capsules (950 mg) of Sentra AM® in the morning and two capsules (961 mg) of Sentra PM® at bedtime for 30 days. At the completion of the 30-day period, subjects were asked to complete posttreatment measures, including the PCL-M, the SF-36, CERQ-short, and ESS. Data were collected using a HIPAA-complaint Web-based portal linked to an SQL database. The screening, pretreatment, and posttreatment self-report measures were automatically entered into the database as subjects completed them.
The primary endpoint was the PCL-M, as a measure of PTSD symptoms. Secondary outcomes were daytime grogginess as measured on the ESS, cognitive and emotive function using CERQ-short, and the mental health score on the SF–36. All comparison of before and after deltas were examined using paired Student's t-tests. The comparisons were made assuming unequal variance.
A total of 87 individuals were screened, of whom 74 screened positive and were sent informed consent documents. Of these, 33 individuals completed and returned the informed consent document and the baseline questionnaires. Three subjects did not begin the study medical food due to new and unrelated occurrence of a more serious health issue. Of the 30 subjects who initiated taking the medical food, 21 completed the treatment and posttreatment questionnaires through the HIPAA-compliant Web-based portal.
Results
PTSD and GWI symptoms include fatigue, cognitive dysfunction predominately affecting immediate and short-term memory, sleep disturbance, alteration of dreams, depression, anxiety, and panic attacks. There was improvement in these symptoms overall, as measured by the PCL-M, SF-36 mental component, and ESS questionnaires. All tests were scored based on normal distributions. Normal distribution was verified with an f-test comparing the variances at baseline and day 30. The PCL-M pretreatment mean score was 64.91 with a standard deviation of 9.55, while the posttreatment mean score was 47.19 with a standard deviation of 12.51. The paired t-test gave a value of 6.39 indicating a substantial correlation with a P-value of less than 0.001 (Fig. 1). A post hoc analysis looking at the questions on the PCL-M showed a statistically significant improvement in sleep parameters. The SF-36 pretreatment mental component mean score was 24.41 with a standard deviation of 10.42, while the posttreatment mental component mean score was 38.51 with a standard deviation of 10.88. The paired t-test gave a value of 5.12 indicating a significant correlation with a P-value of less than 0.001 (Fig. 2). The ESS pretreatment mean score was 10.71 with a standard deviation of 6.26, while the posttreatment mean score was 8.10 with a standard deviation of 5.74. The paired t-test gave a value of 3.32 indicating a significant correlation with a P-value of less than 0.001 (Fig. 3). The SF-36 physical pretreatment mean score was 38.24 with a standard deviation of 7.51, while the posttreatment mean score was 39.65 with a standard deviation of 9.24. The paired t-test gave a value of 1.13, which did not meet the level of significance according to the P-value set at 0.05 (Fig. 4). The CERQ-short pretreatment mean score was 47.28 with a standard deviation of 9.40, while the posttreatment mean score was 46.19 with a standard deviation of 5.85. The paired t-test gave a value of 0.56, which did not meet the level of significance according to the P-value set at 0.05 (Fig. 5). There have been no prior SF-36, PCL-M sleep items, or ESS reports with improvement of this magnitude in patients with deployment-related PTSD. The precise components of the products used in this study are listed in Table 1.

Baseline and Day 30 mean PCL-M scores.

Baseline and Day 30 mean SF-36 mental component scores.

Baseline and Day 30 mean ESS scores.

The percent change from baseline to day 30 based on mean CERQ-short scores. The P-value did not meet the level of significance.
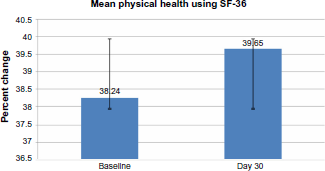
The percent change from baseline to day 30 based on mean SF-36 physical component scores. The P-value did not meet the level of significance.
Table describing the precise components of Sentra AM and Sentra PM.

Discussion
We found that a nutritional intervention using a proprietary medical food formulation significantly reduced PTSD symptoms among combat veterans with self-reported PTSD symptoms and distress. The observed reduction in the primary endpoint was clinically relevant, with an average decrease of 17 points. In particular, we observed clinically relevant improvements in measures of sleep quality, an outcome of particular relevance for treating PTSD. Other pharmacological treatments show only partial improvement in PCL-M scores, and sleep disturbance in PTSD is a prominent source of distress and impairment. 28
We hypothesize that the mechanism of action for this nutritional intervention is via its effect on the autonomic nervous system. There is significant evidence supporting the role of a dysfunction in autonomic nervous system activity in patients diagnosed with PTSD, with the parasympathetic autonomic nervous system showing suppression resulting in disturbed and augmented sympathetic reactivity. The suppression of the parasympathetic system, particularly during sleeping hours, is also closely associated with sleep disorders. 29 Failure to activate parasympathetic activity leads to an inability to initiate sleep, maintain sleep, activate REM sleep, and reach delta sleep. This constellation of events is associated with residual daytime grogginess and exacerbation of mood disorders. Consistent with our hypothesis, we observed improvement in daytime grogginess and improvement in sleep quality.
The predominant neurotransmitter involved in regulating parasympathetic autonomic nervous system activity is acetylcholine.27,28,30–33 Acetylcholine is intimately involved in REM sleep, deep delta sleep, and sleep maintenance.29,34 Serotonin, another neurotransmitter, initiates sleep and maintains sleep. Previous work has shown that providing the neurotransmitter precursors for acetylcholine and serotonin can improve sleep architecture. 28 While we recognize that each of these neurotransmitters could be impacted on a higher central nervous system level, the nutrient management of sleep and other autonomic functions is a promising approach to the management of the signs and symptoms of postdeployment autonomic irregularities.
Nutritional management of disease has been fundamental since the advent of therapeutic medicine. Tepaske et al. 35 administered an arginine-based preparation to patients prior to cardiac surgery. Postoperative creatinine clearance and immune function were improved. Tepaske et al. 35 and Kalantar-Zadeh et al. 36 demonstrated that administration of amino acid neurotransmitter precursors in patients with congestive heart failure improved clinical outcomes. These two examples demonstrate the potential of the nutrient management of diseaes.
Serotonin and acetylcholine initiate sleep, elicit REM sleep, and promote delta sleep. Sentra PM® provides amino acid precursors 5-hydroxytryptophan and choline that should augment the production of neurotransmitters implicated in sleep disorders.37–39 The precursor 5-hydroxytryptophan is converted to serotonin; choline is converted to acetylcholine, bursts of which are essential for REM sleep. Sentra AM® provides amino acid precursors glutamate and acetylcholine that should augment the production of neurotransmitters implicated in initiating and propagating normal cognitive processes and general muscle function.
Medical foods are a class of Food and Drug Administration (FDA)–regulated products indicated for the dietary management of specific disease states. Medical foods are required to be provided under the supervision of a prescribing physician and are composed of ingredients that are generally recognized as safe. The FDA has published extensive reviews of the safety of amino acids in both nutrient and pharmacologic doses and did not find any pharmacokinetic interaction between amino acids and pharmaceuticals.
In this study, Sentra AM® and Sentra PM® were associated with the improvement of PCL-M, SF-36, and ESS. The data were highly statistically significant, and there was a nearly uniform positive response. The uniformity of response allowed for demonstration of statistical significance with a relatively small cohort of patients. There were no side effects reported during the course of this study. This could reflect that the active ingredients are amino acid based or could reflect that we did not systematically assess for side effects.
This was a pilot study to explore the response to specific nutritional deficiencies associated with autonomic dysfunction among combat veterans with PTSD symptoms Limitations to this study include the small sample size, and the possibility of a placebo effect as this was a single-arm, open-label study. This will be explored through a multicenter, double-blind, placebo-controlled trial to follow.
Author Contributions
Conceived and designed the experiment: WES, MC, DSS. Analyzed the data: WES, DSS. Wrote first draft: WES, MC, SP, AC, DSS. Contributed to the writing of the manuscript: WES, MC, MB, SP, AC, LM, DSS. Agree with manuscript results and conclusion: WES, MC, MB, SP, AC, LM, DSS. Jointly developed the structure and arguments for the paper: WES, MC, AC, DSS. Made critical revisions and approved final version: WES, MB, AC, DSS. All authors reviewed and approved of the final manuscript.