
Abstract
The aging population in Japan has recently resulted in a rapid increase in elderly individuals. Airway management is thus being required more and more often. Aspiration pneumonia is a life-threatening problem among patients with swallowing problems. Several new surgical methods of laryngeal closure that are easier and safer than previous methods have been developed. Among these new methods, we have performed the Kano method as closure of the larynx using double flaps of the divided craniad vocal folds and the divided caudad vocal folds with partial resection of the thyroid and cricoid cartilages for patients with intractable aspiration. We encountered minor leakage in two patients, but these soon closed spontaneously. This procedure is less invasive than other methods such as total laryngectomy and tracheal separation and has great advantages in terms of low blood loss and short duration of the operation.
Introduction
Tracheostomy is generally used in patients with upper airway obstruction or need for airway management, such as those with high sputum production or recurrent aspiration. In patients not using a respiratory ventilator, cannulation is unnecessary. A cannula and cuff often induces granulation, inflammation, stenosis and tracheoarterial fistula when used for extended periods. For this reason, avoiding long-term use of a cannula is desirable. New methods of laryngeal closure have recently been reported and are becoming widespread in Japan1–5 because of the ease and simplicity of the procedures. We have previously reported on 3 patients who underwent laryngeal closure using the Kano method. 4 Quite recently, another method has been introduced. 6 We compared and discussed these methods.
Surgical Technique of the Kano Method
Closure of the larynx was performed as described by Kano et al. 4 A vertical anterior cervical skin incision was made to expose the anterior aspect of the thyroid cartilage. Strap muscles were divided in the midline laterally. The central portions of the thyroid and cricoid cartilages were removed. The laryngeal lumen was opened widely using a vertical midline mucosal incision. An intralaryngeal circular mucosal incision was made on the vocal folds for division of the arytenoid cartilage. The incision was performed from the anterior to the lateral aspect of the vocal folds, then across the posterior commissure (posterior wall of the glottis) to create superior and inferior flaps. In the posterior commissure, the mucosa of the superior flap was elevated with the divided craniad arytenoid cartilage and the mucosa of inferior flap was elevated with the caudad arytenoid cartilage. The upper vocal fold flaps and the lower vocal fold flaps were closed with sutures. One sternohyoid muscle was divided. The divided muscle pedicles were interposed between both double flaps and anchored to the posterior commissure with sutures to fill in the dead space between flaps. The wound was closed with a drainage tube.
Case Report
Details of the patients are shown in Table 1. All patients presented with intractable aspiration and underwent laryngeal closure using the Kano method. Patient 1 had undergone surgery for oropharyngeal cancer. Primary and cervical lymph nodes were controlled, but lung metastasis was identified. To accomplish his desire to resume transoral intake, we performed laryngeal closure using the Kano method for intractable aspiration as a less-invasive alternative to other methods. Patient 2 had experienced repeated tracheal bleeding events and risk of tracheo-innominate artery fistula was identified on computed tomography (CT). We encountered leakage in Patients 2 and 3. However, leakages were easily controlled within 2–3 weeks using conservative methods such as drainage, disinfection and pressure on the wound.

Discussion
Several surgical options are available for the treatment of intractable aspiration, including total laryngectomy, laryngotracheal separation, and laryngeal closure. Total laryngectomy is a relatively invasive procedure associated with high morbidity rates. Laryngotracheal separation is less invasive, relatively easy to perform and a quite reliable option, particularly in children. 7 However, both total laryngectomy and laryngotracheal separation are associated with high incidences of pharyngo-cutaneous fistula. Furthermore, a tracheo-innominate artery fistula may occur due to the presence of a tracheostomy cannula in a laryngectomized patient. 8 Three new laryngeal closure methods have recently been developed in Japan. Areas of laryngeal cartilage resected in each method are shown in Figure 1. The Sato method uses a double mucosal hinged flap. The anterior part of the thyroid cartilage is partially removed to allow visualization of the larynx lumen. The false vocal fold and vocal fold are sutured bilaterally, and the dead space between high and low hinged flaps is filled with strap muscle. The Kano method uses a double mucosal hinged flap with partial resection of the cricoid and thyroid cartilages. 4 The surgical procedure can be performed with local anesthesia alone under certain circumstances. The Katori method uses an upward single mucosal hinged flap with partial resection of the thyroid cartilage, and total resection of bilateral arytenoid and cricoid cartilages. 6 Due to the wide resection of the laryngeal framework, mucosal sutures are easy and the amount of dead space is decreased. Decreased leakage can be expected with these methods. Even if leakage appears, healing is readily achieved with simple conservative management. Additional cricopharyngeal myotomy can reportedly improve swallowing ability with the Katori method. Which of these methods is best remains unclear, but our experience has shown that the Kano method is simple and reliable, with early wound healing and a low frequency of postoperative leakage. The Katori method might also decrease leakage rates. These new methods of laryngeal closure represent good news for patients with intractable aspiration.
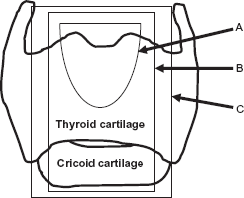
Resection area with each method. (A) Sato method: resection of thyroid cartilage alone in anterosuperior region. (B) Kano method: resection of thyroid cartilage and cricoid cartilage in central region. (C) Katori method: thyroid cartilage and total resection of cricoid and arytenoid cartilages in central region.
Disclosures
Author(s) have provided signed confirmations to the publisher of their compliance with all applicable legal and ethical obligations in respect to declaration of conflicts of interest, funding, authorship and contributorship, and compliance with ethical requirements in respect to treatment of human and animal test subjects. If this article contains identifiable human subject(s) author(s) were required to supply signed patient consent prior to publication. Author(s) have confirmed that the published article is unique and not under consideration nor published by any other publication and that they have consent to reproduce any copyrighted material. The peer reviewers declared no conflicts of interest.