
Abstract
Lumbago is one of the most prevalent symptoms in patients with osteoporotic vertebral fracture. Roland-Morris Disability Questionnaire (RDQ) is a quality of life (QOL) questionnaire targeted for evaluating lumbago. Although total score is the usual way of analysis, we have tried to make more use of it by subscale analysis. Forty-four osteoporotic patients were evaluated for their QOL using RDQ and SF-8; a widely accepted generic (non disease-specific) QOL questionnaire. Subscales and summary scores of SF-8 were significantly lower than Japanese norm. Patients with fracture had significantly lower scores including RDQ. Multiple regression analysis has shown that total score of RDQ was significantly contributed by bodily pain as well as other subscales of SF-8. Principal component analysis has revealed that RDQ consists of two components representing general, and mental or social aspect of lumbago. Defining the component structure and determining the procedure to obtain the subscales would make the most use of RDQ, and contribute to the better evaluation of patients with lumbago.
Introduction
Osteoporosis is defined as a skeletal disorder characterized by compromised bone strength predisposing a person to an increased risk of fracture such as spinal, hip and wrist fractures. 1 Of these, spinal compression fracture affects the largest number of subjects. 2 Although spinal fracture has not received much attention previously, studies have clarified that it is a fracture of great clinical importance associated with increased mortality, co-morbidity, and compromised ADL (activity of daily living).3–5 Of the various subjective symptoms related to spinal fracture, lumbago is by far the most important one. 6
Lumbago is a symptom which is completely subjective in nature. Thus lumbago can be evaluated only by subjective measures. Of the various measurement scales clinically available, QOL (quality of life) is the only clinical outcome representing the patients' subjective perception of health. 7
Recently, many questionnaires for QOL evaluation have become available. They are classified into two major categories; generic and disease-targeted. 7 Generic ones, by their definition, only consists of questions related to the subjects' general status, and do not include the questions related to the features which are specific to a certain disease. Therefore, they are applicable to such studies as comparing the impact of various diseases on QOL, or even to the evaluation of healthy subjects. In contrast, disease-targeted ones include items specific to a certain disease. They can be more sensitive than the generic ones in detecting the QOL impairment closely related to a certain disease state, but are not applicable to the evaluation of patients with other diseases. The most widely used generic QOL questionnaire would be SF-36 and its shortened form; SF-8.8,9
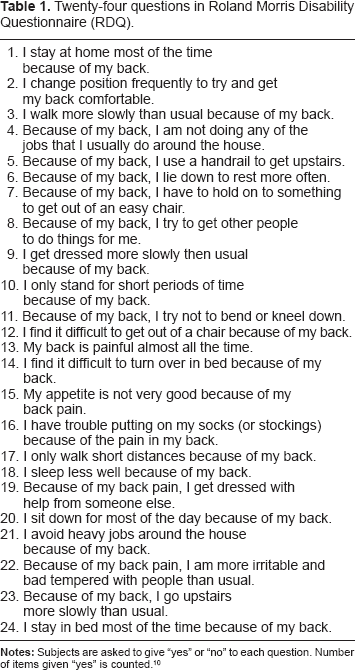
Roland-Morris Disability Questionnaire (RDQ) is rather different from the above-mentioned questionnaires, and unique in that it is specific to a specific symptom; lumbago. 10 It is composed of 24 questions, all of which are related to lumbago (Table 1). The subjects are asked to give “yes” or “no” to each question. Total number of questions given “yes” is calculated. Thus higher number is associated with more severe lumbago. Looking at the 24 items in Table 1, we have noticed that what these items represent is heterogenous. Some of them seem to be related to the physical aspects of QOL, while others are likely to represent other aspects of QOL. Then we have hypothesized that RDQ could be utilized in ways other than obtaining the total count only, and studied the component structure of RDQ by simultaneously employing SF-8 and analyzing the data with multivariate analyses.
Twenty-four questions in Roland Morris Disability Questionnaire (RDQ).
Subjects and Methods
Subjects
The study subjects were 44 women aged 75.8 ± 7.3 years with osteoporosis visiting the Outpatient Clinic, Orthopedic Department Hyogo college of Medicine. The diagnosis of osteoporosis was made based on the Diagnostic Criteria for Primary Osteoporosis in Japan. 11 Based on the X-ray film, the presence or absence of vertebral fracture was determined by one of the authors (Yoh K) before performing the QOL measurement. Vertebral fracture was present and absent in 18 (40.9%), and 26 (59.1%) patients, respectively.
QOL evaluation
QOL was assessed using two questionnaires on the same day between September and December 2008. One is SF-8, which is one of the most commonly used questionnaires worldwide. According to the authorized instruction, the data were transformed to the deviation value adjusted by the Japanese national norms. 9 Eight subscales were obtained; PF (physical function), RP (role physical), BP (bodily pain), GH (general health), VT (vitality), SF (social function), RE (role emotional), and MH (mental health). These scores are further summarized into two summary scores; PCS (physical component summary) and MCS (mental component summary). These subscales and summary scores are interpreted as follows; 50 corresponding to the national norms, and 40 indicating one standard deviation lower than the norm.
With regard to RDQ, total scores were counted. 12 Additionally, data were also analyzed using multivariate analyses, the details of which would be given below.
Data analyses
Data were analyzed using SPSS 17.0J (SPSS Japan, Tokyo). Data in the two independent groups were analyzed with t-test. Data from SF-8 were analyzed with t-test for one sample for comparison with the national norms. The correlation of two independent groups was evaluated with Pearson's correlation. Multiple regression analyses, with stepwise methods, were employed to study the relative contribution of various factors. Principal component analyses were performed to summarize the 24 items of RDQ into the small numbers of components (summary scores).
Results
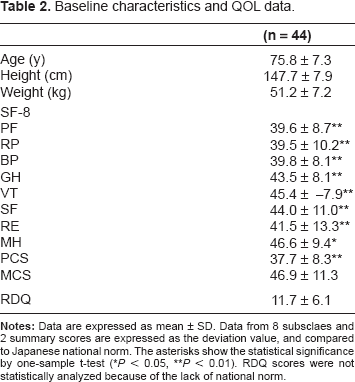
QOL Data: In Table 2 is shown the eight subscales and two summary scores of SF-8, and total scores of RDQ. SF-8 data were compared to the national norms. All eight subscales and PCS were significantly lower than the national norms.
Baseline characteristics and QOL data.
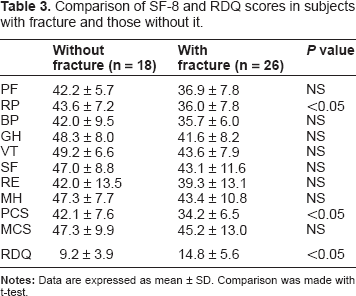
Effects of vertebral fracture on QOL scores: When these data were compared between subjects with vertebral fracture and those without it, RP and PCS were significantly lower, and total score of RDQ was significantly higher; ie, worse in those with fracture (Table 3).
Comparison of SF-8 and RDQ scores in subjects with fracture and those without it.
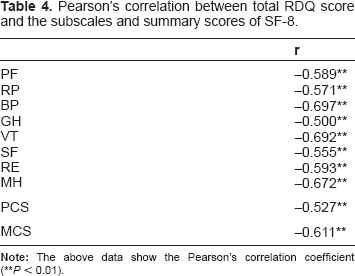
Correlation of total score of RDQ and subsclaes and summary scores of SF-8: Next, the correlation between the total scores of RDQ, and eight subscales and summary scores of SF-8 were studied. As shown in Table 4, the total score of RDQ were significantly correlated with all these scores.
Pearson's correlation between total RDQ score and the subscales and summary scores of SF-8.
Multiple regression analysis for RDQ: In order to elucidate the relative contribution of eight subscales to the total score of RDQ, multiple regression analysis was done (Table 5A). Although it is natural that BP is a significant contributor to the RDQ score, MH was also a significant determinant. As shown in Table 5B, PCS and MCS both contributed to the total scores of RDQ.
Multiple regression analyses for the determination of independent factor for the total score of RDQ.

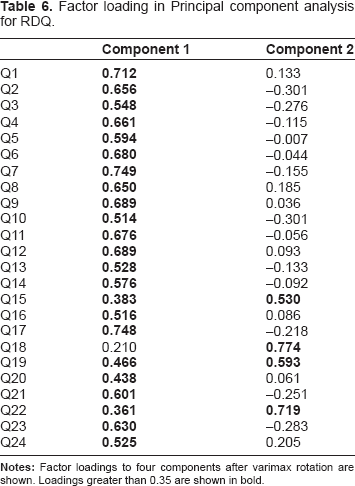
Principal Component Analysis (PCA) for RDQ: The above data that the total scores of RDQ were contributed by MH and MCS strongly suggest that RDQ represents something different from BP in SF-8, or in other words, is heterogenous in its structure. Thus, we have performed principal component analysis (PCA) to study its component structure in more detail. According to the Scree Plot, two components were obtained (Fig. 1). The factor loading by each item to these two components is shown in Table 6. Strong association of component 2 with such items as 18 and 22, suggest that component 2 represents the mental and social aspects of lumbago. In contrast, component 1 was associated with wide range of items, thus considered to represent lumbago in general, probably emphasizing its physical aspects.
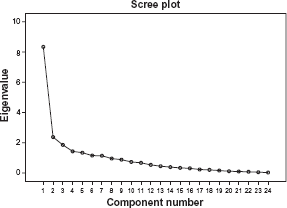
Scree Plot for principal component analysis of RDQ. This figure shows the Scree plot in the principal component analysis for 24 items of RDQ. The curve was considered to be mimicked by two lines. From this plot, summarizing the data into two components was considered appropriate.
Factor loading in Principal component analysis for RDQ.
Multiple regression analysis for two components of RDQ: Finally, multiple regression analyses were done for the above-mentioned two components (Table 7). Component 1 was significantly contributed by BP and VT, whereas component 2 was significantly determined by SF, which suggests the validity of the above interpretation.
Multiple regression analyses for two components of RDQ.

Discussion
In this paper, we have shown that RDQ can be summarized into two components; each representing the general aspects, and mental and social aspects of lumbago. Since its first publication, 10 RDQ has acquired world-wide reputation, and editions under the various languages are currently available. 12 Papers on the basic consideration have also been published. For example, papers are available on the least meaningful score changes in the longitudinal studies.13,14 As far as we know, however, RDQ data have not been analyzed in ways other than calculating the total scores.
Since national norms are available for SF-8, data were compared with them. Practically all of them were significantly lower than the Japanese norms. These scores, as well as the RDQ scores, were worse in fractured subjects. Multiple regression analyses have shown that the total RDQ scores are affected by subscales other than BP or MCS.
PCA is one of the statistical procedures belonging to the multivariate analyses. 15 It is used to summarize the diversity of data into the summary scores. From the raw data, first component is extracted with the highest level of information (eigenvalue), and the second one is extracted from the remaining information. Thus, each component thus obtained is independent of each other. Apparently, the second component thus obtained was associated with the mental or social aspects of lumbago, but not with its physical aspects. Thus, it is quite likely that RDQ could be analyzed as a questionnaire composed of multiple factors or subscales.
We believe that our study yield new insights in the interpretation of RDQ. Calculating only the total score could extract only too small fraction of information from data obtained from questions as much as 24 items. Defining the component structure and determining the procedure to obtain the subscales would make the most use of RDQ, and contribute to the better evaluation of patients with lumbago.
Disclosure
This manuscript has been read and approved by all authors. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The authors and peer reviewers of this paper report no conflicts of interest. The authors confirm that they have permission to reproduce any copyrighted material.