
Abstract
Background
The aim of this study was to identify the unique molecular characteristics of biliary tract cancer (BTC) for the development of novel molecular-targeted therapies.
Materials and Methods
We performed mutational analysis of KRAS, BRAF, PIK3CA, and FBXW7 and immunohistochemical analysis of EGFR and TP53 in 63 Japanese patients with BTC and retrospectively evaluated the association between the molecular characteristics and clinicopathological features of BTC.
Results
KRAS mutations were identified in 9 (14%) of the 63 BTC patients; no mutations were detected within the analyzed regions of BRAF, PIK3CA, and FBXW7. EGFR overexpression was observed in 5 (8%) of the 63 tumors, while TP53 overexpression was observed in 48% (30/63) of the patients. Overall survival of patients with KRAS mutation was significantly shorter than that of patients with the wild-type KRAS gene (P = 0.005). By multivariate analysis incorporating molecular and clinicopathological features, KRAS mutations and lymph node metastasis were identified to be independently associated with shorter overall survival (KRAS, P = 0.004; lymph node metastasis, P = 0.015).
Conclusions
Our data suggest that KRAS mutation is a poor prognosis predictive biomarker for the survival in BTC patients.
Introduction
Biliary tract cancer (BTC) is characterized by significant geographic variation; it is rarely detected in Europe and North America but has a high incidence rate in some areas of Latin America and Asia. 1 BTC comprises aggressive tumors and has extremely poor prognosis; the five-year survival rates are 30%–50% for resectable tumors and less than 5% for unresectable cases. 2 Although surgical resection currently remains the only potentially curative treatment, most patients are already at the advanced unresectable stage of the disease at the time of diagnosis. Systemic chemotherapy based on the combination of 5-fluorouracil with cisplatin and gemcitabine can improve the quality of life; however, the impact on survival is minimal. 3 Therefore, new therapeutic modalities, including molecular targeting therapy, need to be explored for advanced BTC patients to improve treatment outcomes.
To date, several studies have assessed the incidence of molecular abnormalities in BTC, but the results are inconsistent.4,5 For example, the incidence of mutations of KRAS, BRAF, and PIK3CA genes in BTC patients varies between 0% and 60%, 0% and 22%, and 0% and 12.5%, respectively. In recent data of TCGA (the cancer genome atlas and c-bioportal), the frequencies of mutation of KRAS, BR AF, PIK3CA, and FBXW7 in cholangiocarcinoma are reported to be 5.7%, 2.9%, 5.7%, and 2.9%, respectively. Overexpression of EGFR and TP53 has been detected in ∼10% and 6%–35%, respectively.6,7 In addition, different carcinogenic mechanisms involving molecular abnormalities have been reported among each subdivision.8,9 However, previous studies analyzing aberrations of oncogenes or tumor suppressor genes in BTC have been conducted on relatively small patient populations, probably because of low BTC prevalence in Western countries. Therefore, unlike other major solid tumors, the molecular mechanisms underlying BTC development remain poorly understood, and their clinical significance remains elusive.
In the present study, we examined the mutation and expression of several molecules that have been reportedly associated with the development of BTCs and analyzed their correlation with patients' clinical features. The main purpose of this study was to identify the molecular characteristics of BTC that could help developing novel molecular-targeted therapies for BTC.
Materials and Methods
Subjects
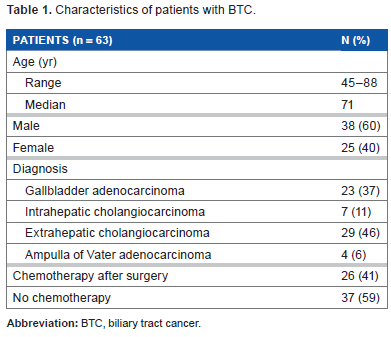
A total of 63 BTC patients who had undergone tumor resection and had been histologically diagnosed for adenocarcinoma of the bile duct or gall bladder at the Kyorin University Hospital between January 2005 and December 2011 were enrolled in the present study. According to the anatomical location of original tumors, BTC is subdivided into gall bladder adenocarcinoma (GBC), intrahepatic cholangiocarcinoma (IHCC), extrahepatic cholangiocarcinoma (EHCC), and ampulla of Vater adenocarcinoma (AC). Among the BTC patients enrolled in this study, 23 (37%) patients had GBCs, 7 (11%) patients had IHCCs, 29 (46%) patients had EHCCs, and 4 (6%) patients had ACs. Patients' clinicopathological characteristics including gender, age, lymph node metastasis, tumor differentiation, location, pTNM pathological classification according to the Union for International Cancer Control, 10 and long-term outcome by 2014 were retrieved from medical records. The patient population included 38 (60%) males and 25 (40%) females, with a median age of 71 years (Table 1). Although BTC treatment was heterogeneous, no patient had been administered molecular-targeted drugs. This retrospective study was approved by the Ethics Committee of the Kyorin University School of Medicine. Our research complied with the principles of the Declaration of Helsinki.
Characteristics of patients with BTC.
Mutational analysis of KRAS, BRAF, PIK3CA, and FBXW7.
Paraffin-embedded tissues were sectioned to 10-µm thicknesses and mounted as three separate slides per tissue. The resulting slides were treated three times with xylene and washed with ethanol. To minimize contamination by normal DNA, areas where at least 70% of the cells exhibited disease-specific pathology were dissected under a binocular microscope and used for DNA extraction with the DNeasy Blood & Tissue Kit (QIAGEN). We obtained polymerase chain reaction products by using Veriti® Thermal Cycler (Applied Biosystems), and they were then purified by QIAamp DNA FFPE Tissue Kit (QIAGEN). Regions of the KRAS, BRAF, PIK3CA, and FBXW7 genes were amplified using gene-specific primers and subjected to direct DNA sequencing as previously described.11–13 KRAS point mutations were screened for codons 12 and 13 within exon 2, two hot spots that cumulatively include >95% of this gene's mutations. 12 BRAF was screened for V600E mutation within exon 15, where >95% of point mutations occur.14,15 PIK3CA mutations were screened within exons 9 and 20 where >80% of point mutations occur.11,16,17 FBXW7 mutations were screened within exons 8, 11, and 12, since most of the FBXW7 mutations (eg, R465C, R465H, R505C, and Y519C) occur within these regions. 18
Immunohistochemistry of EGFR and TP53
The overexpression of EGFR and TP53 was examined by immunohistochemistry. Based on the HercepTest™ (Dako) criteria, EGFR signals were defined in terms of staining intensity of the cancer cell membrane: 0, between 0% and 10% stained cells; 1+, faint and/or partial staining in >10% cells; 2+, moderate staining in >10% cells and strong and complete staining in 10%–30% cells; 3+, strong and complete staining in >30% cells. 19 For the cases showing mixed intensities, predominant signal was selected as the final score. The samples with the final score of 2+ or 3+ were considered positive for EGFR overexpression (Fig. 1A-1). TP53 staining was classified according to previous reports 20 as follows: (grade 1) absent; (grade 2) present in a minority of the cells (below 10%); (grade 3) present in approximately 10%–75% of the cells; or (grade 4) present in virtually all the cells (Fig. 1B-1). Only the tumor cells with dense nuclear staining were graded as positive. Tumors with TP53 expression in the majority of the cells (grades 3 and 4) were classified as exhibiting TP53 overexpression.

Representative immunohistochemical analyses and HE results of EGFR and TP53: (A-1) 2+ immunoreactivity for EGFR, (A-2) HE, (B-1) positive immunoreactivity for TP53, and (B-2) HE.
The EGFR and TP53 staining intensities were evaluated by a surgeon (MY) and a pathologist (YO) independently.
Statistical analysis
Associations between molecular factors and clinicopathological parameters were assessed by χ 2 test or Fisher's exact test. Overall survival (OS) after surgery was calculated using the Kaplan–Meier method; the log-rank test was performed to compare survival curves. To identify independent predictive biomarkers for survival, multivariate analyses were performed using the Cox regression model (a log-rank test) for OS. Two-tailed P values of <0.05 were considered significant. All analyses were performed using the SPSS software (SPSS for Macintosh Version 21; IBM Corporation).
Results
KRAS, BRAF, PIK3CA, and FBXW7 mutations in BTC
KRAS mutations were identified in 9 (14%) of the 63 BTC patients: 2 of 23 GBC cases (9%) and 7 of 29 EHCCs (24%). The G12V mutation was detected in 3 BTC patients, G12D in 5 BTC patients, and G12S in 1 BTC patient (Table 2). OS of KRAS mutation-bearing patients was significantly worse than that of the patients with the wild-type KRAS gene (Fig. 2A; P = 0.005 by log-rank test). In addition, patients with lymph node metastasis showed higher rate of KRAS mutation than those without metastasis, although the difference was statistically only marginal (P = 0.066).
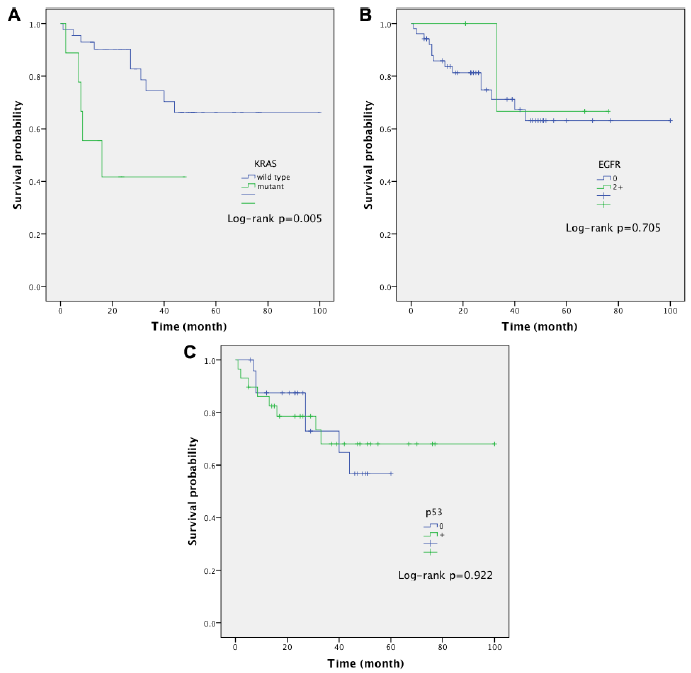
OS according to molecular features by Kaplan–Meier analysis. (A) OS of BTC patients classified according to the presence of KRAS mutations. (B) OS of BTC patients classified according to the presence of EGFR overexpression. (C) OS of BTC patients classified according to the presence of TP53 overexpression.
Molecular features of patients with BTC.
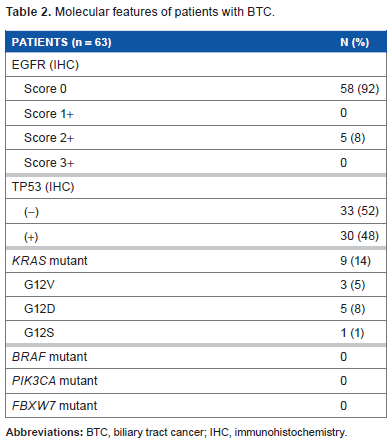
No mutations were identified within the analyzed regions of the BRAF (exon 15), PIK3CA (exons 9 and 20), and FBXW7 genes (exons 8, 11, and 12) in BTC patients.
EGFR overexpression
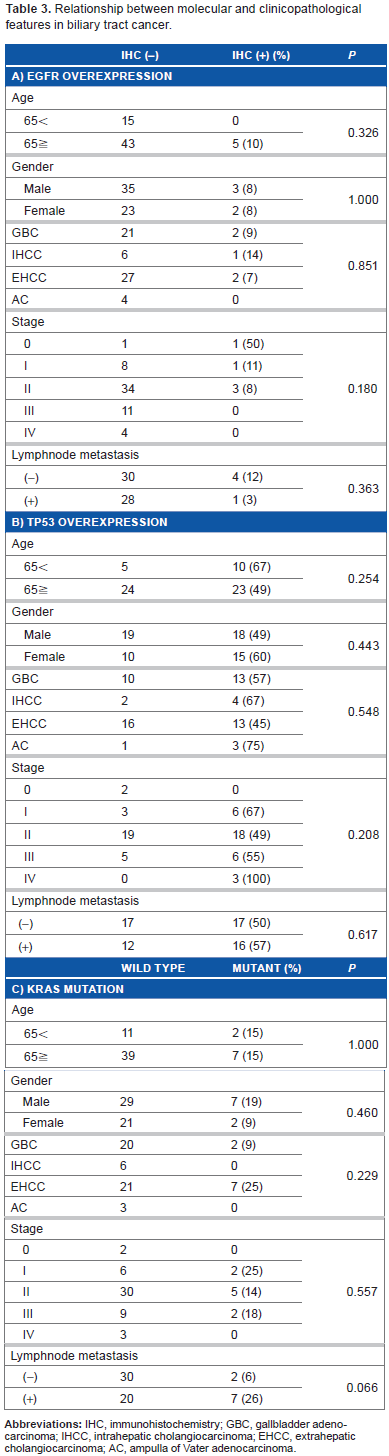
EGFR expression was absent in 58 of the 63 tumors (92%). The remaining 5 (8%) samples were scored as 2+ and considered positive for EGFR overexpression; no samples showed scores of 1+ or 3+ (Table 2). There was no statistically significant difference in clinicopathological features between the patients with and without EGFR overexpression (Table 3a and Fig. 2B).
TP53 overexpression
TP53 overexpression was found in 30 of the 63 patients (48%; Table 2). However, there was no statistically significant difference in clinicopathological features between the patients positive and negative for TP53 overexpression (Table 3b). Similarly, no association between TP53 overexpression and OS was detected (Fig. 2C).
Relationship between molecular and clinicopathological features in biliary tract cancer.
Multivariate analysis for OS
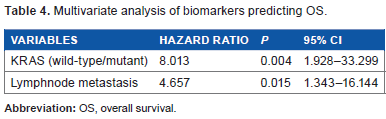
Multivariate analysis of the molecular and clinicopathological parameters of BTC (listed in Tables 1 and 2) identified KRAS mutation (P = 0.004) and lymph node metastasis (P = 0.015) as independent factors for shorter OS (Table 4).
Multivariate analysis of biomarkers predicting OS.
Discussion
To the best of our knowledge, this is the first study to reveal the prognostic significance of molecular abnormalities in BTC. In the present study, KRAS mutations were detected in 14% of BTC patients, which is within the 0%–60% range reported by other studies including TCGA.4,5,21,22 Most strikingly, the treatment outcome of KRAS mutation-positive patients was significantly worse than that of KRAS wild-type patients. To date, no studies have demonstrated the prognostic impact of KRAS genetic alterations in BTC, although KRAS has been reported as one of the most frequently mutated genes in this type of cancer. Our present data suggest that mutations in the KRAS gene can be used as a prognostic biomarker for BTC patients. In addition, KRAS may be associated with the efficacy of molecular-based therapeutic approaches to treat BTC. Currently, no approved KRAS-targeting molecular drugs have been established. However, KRAS mutational status is crucial for the application of anti-EGFR antibody drugs, because KRAS mutations usually confer resistance to these drugs in colon or lung cancers.23,24 In BTC, relationship between KRAS status and efficacy of anti-EGFR antibody drugs remains uncertain. Future studies are required to investigate the efficacy of anti-EGFR antibody-based therapy for BTC patients with KRAS mutations.
BRAF belongs to the mitogen-activated protein kinase signaling pathways, which mediate cellular response to growth factors, including EGF. BRAF mutations have been reported as a relatively common event (22%) in IHCC but not in EHCC, in the Anglo-Saxon population; 25 on the other hand, they were not observed in Chinese patients with IHCC. 26 Our present findings are consistent with the latter report, suggesting ethnic variations in the frequency of BRAF mutations in BTC. These results suggest that BRAF inhibitors that are effective only in the patients with BRAF mutation, such as vemurafenib, may not be effective in Asian patients with BTC.
PIK3CA encodes the catalytic subunit of PI3K that activates a downstream Akt kinase upon stimulation with various growth factors. The response rate to PI3K/Akt/mTOR pathway inhibitors has been found to be significantly higher in patients with PIK3CA mutations than in those with the wild-type gene.16,27 In addition, PIK3CA mutations in colorectal cancer have been associated with clinical resistance to anti-EGFR monoclonal antibodies.28,29 Our present study did not identify mutations in PIK3CA in Japanese patients with BTC, suggesting that the efficacy of PIK3CA inhibitors may be minimal in this ethnic group. However, anti-EGFR antibody-based therapy may be effective in the Japanese BTC population, provided that PIK3CA in BTC plays a similar role as in colorectal cancer.
Consistent with the previous report, EGFR overexpression was not detected in most BTC tumors (92%). 30 Unlike tyrosine kinase inhibitors, cetuximab is effective in colorectal cancer patients with EGFR-negative tumors. 31 If such is the case in BTC, cetuximab therapy may be applicable for BTC even if most cases are negative for EGFR expression. Future studies treating BTC patients with low EGFR expression by cetuximab will be necessary to address this issue.
TP53 is one of the major tumor suppressor genes involved in cell cycle, DNA repair, and apoptosis. In contrast to the previous reports, we found that the incidence of TP53 overexpression was similar between GBC and other BTC categories. In addition, no clinicopathological features were associated with TP53 overexpression. Our results suggest that TP53 overexpression may have little clinical relevance in Japanese patients with BTC.
FBXW7 is a member of the F-box family of proteins, which function as substrate recognition components of the multisubunit ubiquitin ligase SCF. 16 FBXW7-inactivating mutations have been detected in diverse human cancers with an overall frequency of approximately 6%; 16 the highest mutation incidence has been reported for cholangiocarcinomas in Sweden (35%). 16 However, we did not detect FBXW7 mutations in Japanese BTC patients. The reason for this discrepancy remains unknown; however, differences in ethnicities and the prevalence of histological subtypes could be involved. In our study, IHCC represented only 11% of all BTCs, which is consistent with previous reports of BTC histological classification in Japan. 32 In contrast, IHCC is the dominant BTC category in Western countries. 33 IHCC may harbor FBXW7 mutations more frequently than other BTC subtypes. Of note, recent TCGA data show that the mutation rate of FBXW7 in cholangiocarcinoma is relatively low (2.9%), which is consistent with our result. Future studies recruiting a larger number of patients with diverse ethnic background are necessary to elucidate this issue.
This study had some limitations. It was performed retrospectively in a relatively small, heterogeneously treated population; insufficient sample size may contribute to the lack of statistical significance in some analyses. The discrepancy observed between the results of univariate and multivariate analyses may have been caused by these factors. Our findings, therefore, should be validated in subsequent prospective studies on a large number of patients before application in clinical practice.
Conclusions
The present study identified KRAS mutations as a poor prognostic marker for BTC patients. These findings warrant future prospective studies for elucidating the efficacy of molecular-targeting drugs and its association with predictive biomarkers in BTC.
Author Contributions
Conceived and designed the experiments: MY, HO, KO, TW, JF, and MS. Analyzed the data: MY, HO, and KO. Helped with the experiment: SM. Supported pathological diagnosis: MY, YO. Write the first draft of the manuscript: HO. Contributed to the writing of the manuscript: MY, HO, and TM. All authors reviewed and approved of the final manuscript.
Footnotes
Acknowledgment
The authors acknowledge the previous publication of “Molecular analysis of BTCs identified KRAS mutation as a potential prognostic biomarker” 34 , a summary in Japanese of the work presented fully here.