
Abstract
The number of patients with late-onset myasthenia gravis (MG) among patients ≥50 years has been increasing recently. We encountered three patients who developed elderly-onset MG at a particularly advanced age (≥80 years). All were female and positive for anti-acetylcholine receptor antibodies. About 4 years have passed since MG onset in all three patients and symptoms have been controlled without recurrence using a combination of oral low-dose prednisolone and tacrolimus. As many cases of elderly-onset MG do not require strong immunosuppression, we recommend minimum immunosuppressive treatment to avoid adverse events, particularly in patients at an advanced age of ≥80 years.
Introduction
Myasthenia gravis (MG) is more commonly identified in younger individuals, especially women, and is usually associated with thymus disease. In these patients, the symptoms usually recover after undergoing thymectomy. However, elderly-onset MG has been also reported among patients ≥65 years of age.1–4 Thymus abnormalities are usually rare among patients with late-onset MG, aged 50 and above, and clinical presentation is also different from those with early-onset disease, aged less than 50 years old. 5 Differential diagnosis in elderly patients must consider cerebral stroke, motor neuron disease, and Parkinson's disease as the majority present with bulbar symptoms. The treatment options for elderly patients will also differ from those with late- and early-onset MG. We summarize the cases of patients with early-, late-, and elderly-onset MG attending our clinic and detail three cases of elderly-onset MG that occurred in patients at a particularly advanced age (≥80 years of age).
Case Reports
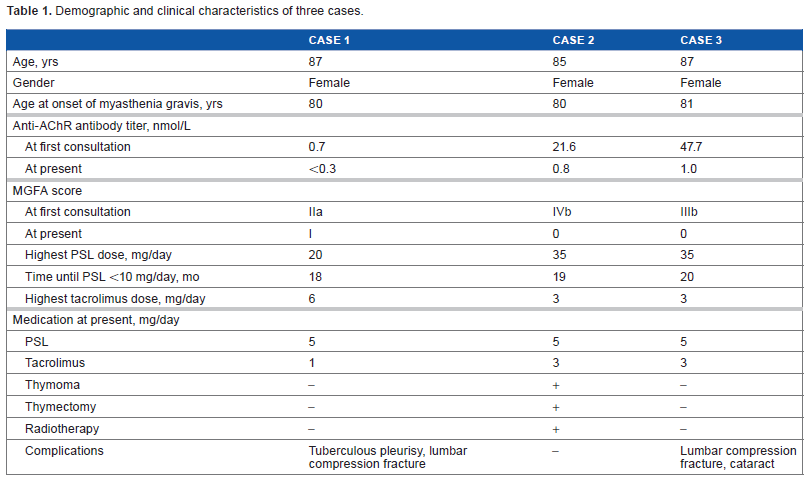
We report three patients with MG who had disease onset at an age of ≥80 years (elderly onset at advanced age), whose characteristics are summarized in Table 1. These three patients are subsequently described in detail.
Demographic and clinical characteristics of three cases.
Case 1
The patient is a Japanese female currently 87 years of age. Ptosis developed at 80 years of age and she received bilateral eyelid lift surgery (blepharoplasty) following a diagnosis of age-related ptosis. However, she visited our hospital after feeling a worsening of weakness and fatigue in all limbs. She had undergone surgery for breast cancer 5 years previously. Ptosis, diplopia, and grade 4 proximal weakness in all limbs were noted; gait was possible using a walker; and Myasthenia Gravis Foundation of America (MGFA) classification was IIa. She recovered from these symptoms temporarily by undergoing edrophonium. Acetylcholine receptor (AChR) antibody level was 0.7 nmol/L. No thymoma was noted on thoracic computed tomography (CT) scanning. Prednisolone (PSL) dose was gradually increased, starting from 5 mg/day to a maximum of 20 mg/day by 5 mg/week gradually, and tacrolimus 3 mg/day was administered together with initial administration of PSL. The tacrolimus dose was increased to 6 mg/day because of low plasma concentrations. Repetitive nerve stimulation performed after the treatment revealed no decrementing response in abductor digiti minimi and upper trapezius.
Tuberculous pleurisy developed 2 years after treatment initiation and the tacrolimus dose was reduced to 2 mg/day. The tuberculous pleurisy improved after administration of anti-tuberculous medication using rifampicin, isoniazid, and pyrazinamide for about 1 year. Osteoporosis-associated lumbar compression fracture occurred 3 years after treatment initiation and the patient temporarily became bedridden but recovered to a condition allowing housework. At 7 years after onset (6 years after treatment initiation), the anti-AChR antibody level was lower than the detection limit under oral treatment with PSL 5 mg/day and tacrolimus 1 mg/day, and there were minimal clinical signs. The patient is independent with respect to activities of daily living (ADL) and she has not been hospitalized for recurrent MG.
Case 2
The patient is a Japanese female currently 85 years of age, who had previously been healthy until developing a swallowing disorder at 80 years of age. Treatment for cerebral infarction was administered by a physician but no improvement was achieved. As her weight loss was marked, she was referred to our department. Muscle weakness in all limbs and easy fatigability were observed, which waned on repetitive stimulation testing. Anti-AChR antibody level was positive at 21.6 nmol/L. Based on these findings, the patient was diagnosed with MG. Two weeks later, the patient was admitted as bulbar palsy symptoms worsened after the development of pneumonia. Ptosis and diplopia were mild. Elevation of the upper limbs was difficult, and standing and gait were impossible. She could not swallow saliva, and thus required nasogastric intubation. MGFA classification was IVb. No respiratory muscle weakness was noted on blood gas analysis or respiratory function testing. An invasive thymoma was observed in the pericardium on thoracic CT scanning. Thymectomy (resection of the thymus, pericardial membrane, and thyroid) was performed as no major abnormality was noted with respect to cardiac or renal function, even though she was elderly. Radiotherapy (total dose 50 Gy) was applied to the region around the thymus after surgery.
PSL dose was gradually increased (5 mg/week) to a maximum of 35 mg/day and then gradually decreased to 5 mg/day. Tacrolimus 3 mg/day was administered concomitantly after surgery when the patient was receiving 20-mg/day dose of PSL. No treatment-related adverse events occurred. Three years after treatment initiation, her anti-AChR antibody level was 0.8 nmol/L under treatment with PSL 5 mg/day and tacrolimus 3 mg/day. No recurrence of thymoma or MG symptoms has occurred subsequently. The patient lives alone, works on a farm, and provides meals for her son living next door, as she had prior to the development of MG.
Case 3
The patient is a Japanese female currently 87 years of age, who had previously been healthy. Bilateral muscle weakness of the hands developed at 81 years of age. Her slippers also came off easily. She visited a physician but no diagnosis could be made. Acute respiratory insufficiency occurred one night. The patient was diagnosed with cardiac asthma and heart failure and was admitted to the cardiovascular department. As her anti-AChR antibody was found to be positive (47.7 nmol/L), she was referred to our department. MGFA classification was IIIb. Ptosis and distal dominant weakness in the muscles of all four limbs were present, tendon reflex was normal, and a swallowing disorder was noted. She ate a low-residue diet and rice gruel. No respiratory disorder was noted. The decremental response to repetitive stimulation was observed.
Surgery was unnecessary as no thymoma was noted on thoracic CT scanning. PSL started at 5 mg/day and increased with 5 mg/week. A maximum PSL dose of 35 mg/day was administered and it was gradually reduced. When the PSL dose was reduced to 30 mg/day, tacrolimus 3 mg/day was started concomitantly. The PSL dose was eventually reduced to 5 mg/day and no recurrence of MG has occurred. Adverse events were compression fracture due to a fall, cataract surgery, and the development of borderline diabetes.
We also assessed different-onset of MG in 43 cases between 2002 and 2013 (Table 2).
Characteristics of myasthenia gravis according to onset-age.
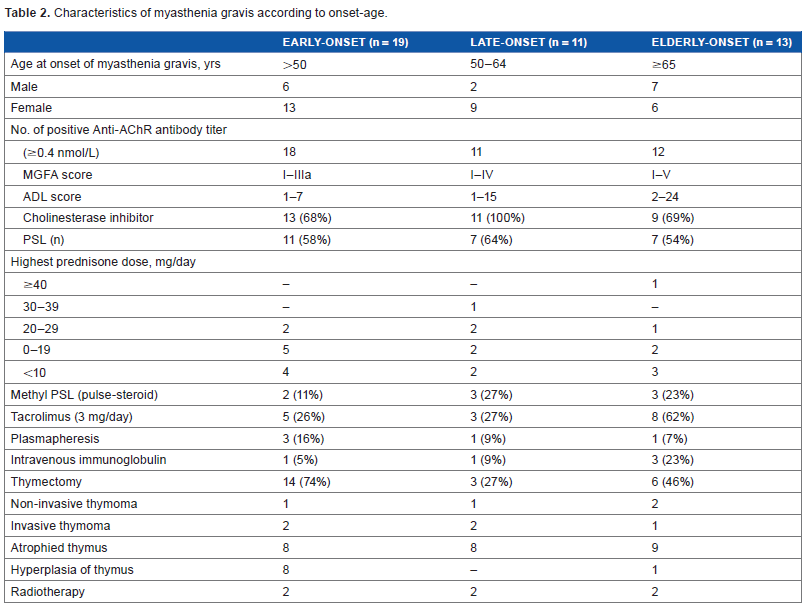
The patients with early-onset MG (13 female, 6 male) were in MGFA class I–IIIa, had an MG-ADL score <8, and had a positive anti-AChR antibody response except one patient. The antibody titer of 0.4 nmol/L and above is set as positive result in our hospital. All the cases started with diplopia and blepharoptosis, and two cases later developed dysphagia and respiratory distress, respectively. Fourteen of 19 (73.7%) underwent thymectomy. Three patients had invasive thymoma and eight patients showed hyperplasia of thymus. Atrophied thymus is found in other patients. More than half of the 19 cases were treated with PSL, and anti-cholinesterase inhibitor, and in addition to these medicines, 5 of the 19 cases were also treated with tacrolimus.
Among the cases with late-onset MG (nine female, two male), three female patients (MGFA class IIa-IIIb, MG-ADL score 1–6) presented with generalized muscle weakness and received thymectomy along with intravenous immunoglobulin, PSL, and tacrolimus. The other cases (MGFA class I–III, MG-ADL score 1–15) initially complained of diplopia and blepharoptosis and were treated with plasmapheresis, methyl PSL 1000 mg/day for 3 days (pulse-steroid therapy), oral PSL, and a cholinesterase inhibitor without undergoing thymectomy. All cases had a positive anti-AChR antibody response.
Of the 13 cases with elderly-onset MG (6 female, 7 male; MGFA class I–V; MG-ADL score 2–24), most initially reported dysphagia, respiratory distress, and/or generalized muscle weakness. One case was seronegative for anti-AChR, muscle-specific kinase, and lipoprotein-related protein 4 antibodies and received treatment with plasmapheresis, pulse-steroid therapy, PSL, and tacrolimus. The others were all anti-AChR antibody positive and were treated with pulse-steroid therapy, PSL, and tacrolimus. In this group, only 6 of the 13 patients (46.2%) with a positive anti-AChR antibody response underwent thymectomy.
Discussion
We report details of three patients with elderly-onset MG at advanced age who were all ≥80 years of age at diagnosis. There is no previous case study done on MG patients with very elderly onset. All were female and positive for anti-AChR antibodies. Other autoimmune diseases were excluded as antibodies toward nuclear, Sjögren's syndrome (SS)-A, Sjögren's syndrome (SS)-B, thyroid peroxidase, and thyroglobulin antigens were all negative. In one patient, invasive thymoma was noted and treated with thymectomy and postoperative irradiation. No thymoma was noted in the other two patients and thymectomy was not necessary. All the patients required the treatment with both oral PSL and tacrolimus in order to control their severe disease conditions. The maximum dose of PSL was 20–35 mg/day, which was maintained ≤2 weeks and then followed by gradual dose reduction. No recurrence occurred while the patients were treated with maintenance PSL 5 mg/day for about 1.5 years.
An increase in the incidence of elderly-onset MG has been reported in publications over recent years,1–4 although development of the disease in patients ≥80 years of age represents a particularly advanced age of onset. The prevalence of MG in patients ≥80 years is unclear but the number of patients being diagnosed suggests an increase in incidence or an improvement in physicians' diagnostic skills or both. Eyelids droop slightly due to age-related skin extension and the muscle strength of all limbs decreases among patients ≥80 years of age even when no specific disease is present. When swallowing function is impaired, cerebral infarction is first suspected, which makes the diagnosis of MG difficult. The anti-AChR antibody level appears to be high in both late- and elderly-onset MG6,7 and this should be actively utilized to assist diagnosis of the disease.
The cholinesterase inhibitor is applied as the first choice of treatment for both ocular and generalized MG. However, immunosuppressive treatment should be supplemented as early as possible in generalized MG including bulbar form. 5 Although steroid therapy can cause major side effects, including diabetes, cataracts, osteoporosis, and infection, it is still considered as the most effective treatment option even in elderly MG patients. 2 All three of our patients responded well to PSL. PSL dose was gradually increased to a moderate level for 2 weeks, which is a relatively short period, and it was then reduced gradually by about 10% every 2 weeks. Tacrolimus was added midcourse, which allowed the total PSL dose to be reduced and thereby minimize its adverse adrenocortical effects. The Pharmaceuticals and Medical Devices Agency of Japan acknowledged tacrolimus and cyclosporine as standard immunosuppressive agents in the treatment of MG, but not mycophenolate and azathioprine. Tacrolimus and cyclosporine are inhibitors of T-cell function through inhibition of calcineurin signaling. However, they may induce increasing susceptible to infection and decreasing glucose tolerance. Cyclosporin may cause nephrotoxicity in the case of long-term treatment. Tacrolimus may have a steroid-sparing effect along and confirmed its safety and tolerability. 8 About 4 years have passed since MG onset in all three patients: symptoms remain controlled on a combination of oral low-dose PSL and tacrolimus without the recurrence of MG. During this period, infection, osteoporosis, compression fracture, and hyperglycemia have occurred; however, all three patients maintain their ADL independence and are able to return to the hospital for follow-up visits by themselves. The indication for thymectomy in late- and elderly-onset MG is less than that for early-onset MG and the combination of corticosteroids with immunosuppressive agents is recommended to reduce corticosteroid doses in late- and elderly-onset MG. 5
Thymectomy for cases of late- and elderly-onset MG is less recommended because they are susceptible to postoperative complications and other possible metabolic diseases, as the chance of lymphoid follicular hyperplasia is low and the thymus is likely to be atrophied in the elderly. Moreover, the patients with late- and elderly-onset MG are less likely to benefit from thymectomy unless they have thymoma. Although therapeutic plasmapheresis is widely used in myasthenic crises, it is not favorable for elderly patients to avoid possible cardiovascular events. In contrast, intravenous immunoglobulin is considered to be a suitable treatment in elderly patients not only in myasthenic crises but also for reducing PSL dose.
Even though elderly-onset MG at advanced age can develop in patients ≥80 years of age, no specific recommendations are needed for their treatment. Serious steroid-related adverse effects are likely to occur in patients of an advanced age and ADL may be impaired due to treatment-associated complications. Minimum necessary treatments are recommended to avoid adverse drug reactions and the general condition of each individual patient should be prioritized.
Author Contributions
Conceived and designed the experiments: NN. Analyzed the data: WTK, HI. Wrote the first draft of the manuscript: NN. Contributed to the writing of the manuscript: WTK. Agree with manuscript results and conclusions: MN. Jointly developed the structure and arguments for the paper: NN, MN, TT, WTK, NT, HI, HY, RA, MN. Made critical revisions and approved final version: MN. All authors reviewed and approved of the final manuscript.