
Abstract
Introduction
Recently, Henoch–Schönlein purpura (HSP) has been observed in elderly people, although it was believed to be uncommon in these subjects. The increased risks of developing end-stage renal disease (ESRD) in adults in comparison with children were highlighted by different studies; however, limited data are available on the treatment of HSP nephritis in adults.
Methods
Between 2002 and 2008, five elderly Japanese patients (>65 years old) (mean age, 68 years, ranging from 65 to 72) with severe forms of HSP nephritis were entered into a prospective study to evaluate prednisolone therapy on the outcome of nephropathy in terms of clinical symptoms and histopathological changes. The patients were considered at risk of developing chronic renal failure when they presented with a nephrotic syndrome and crescentic glomeruli.
Results
At the last follow-up, 4–10 years after initiation of the therapy, four patients had clinically recovered and one died of lung cancer. No patients developed ESRD. The clinical outcome seemed to be correlated with glomerular activity (massive proteinuria and crescent formation). In spite of a relatively large dose of prednisolone, a few adverse effects, such as insomnia and skin lesions, were observed.
Discussion
Our preliminary small study suggests that renal outcome as well as survival of elderly patients with severe forms of HSP might be altered by aggressive prednisolone therapy.
Introduction
The increase in elderly population is becoming a challenge in the nephrology field as well as in general medicine. Indeed, because the kidney undergoes important age-related changes in function and structure, the aging of the population is reflected in changes in the prevalence of kidney diseases. 1 Among them, Henoch-Schönlein purpura (HSP), which is the most frequent vasculitis in childhood, occurs in adults with low frequency. Although previously HSP was considered to be uncommon in elderly subjects, recently HSP has been observed among them. The increased risks of developing end-stage renal disease (ESRD) in adults in comparison with children have been reported by different works.2–5 Several clinicopathological studies in children have shown that patients who present with minimal urinary abnormalities have an excellent prognosis and that only those patients who present with marked proteinuria with or without nephrotic syndrome and/or impaired renal function are at risk of developing chronic renal failure.6–8
Up to now, limited data have been available on the treatment of HSP nephritis in adults, 9 although there is only one report of eight elderly subjects with HSP. 10 In the controlled prospective study of Pillebout et al, 11 no significant effect of addition of cyclophosphamide to steroid therapy on the development of severe renal insufficiency was demonstrated. In the present preliminary prospective study, we examined the effects of early high-dose prednisolone on renal function in elderly patients with severe forms of HSP with nephrotic syndrome as well as on patient survival.
Patients and Methods
Between 2000 and 2014, five elderly patients with HSP nephritis were entered into a prospective study. This research was exempt from the requirement of ethics committee approval, because the research was observational and patients all received standard treatment. Patients gave their written, informed consent for observation and treatment. HSP was defined as documented leukocytoclastic vasculitis on skin biopsy with histopathologic evidence of IgA deposition by immunofluorescence. Inclusion criteria were clinical severity of the renal disease, based on the presence of a nephrotic syndrome (defined by heavy proteinuria, >3.0 g), and the severity of the histopathology, based on the presence of crescent glomeruli on renal biopsy. The patients' age ranged from 65 years to 72 years (average: 67.7 ± 2.7).
A renal biopsy was obtained in all patients before entry into the study. All biopsies were stained with hematoxylin and eosin (H&E), periodic acid Schiff (PAS), and methenamine silver and were analyzed. Endo- and extra-capillary glomerulonephritis was defined by the presence of segmental and crescents in a variable proportion of glomeruli superimposed on diffuse mesangial hypercellularity. Patients were subdivided into two groups: those showing <50% glomeruli with crescent formation (four patients) and those showing ≥50% glomeruli with crescent formation (one patient).
The treatment consisted of methyl-PSL at a dose of 500 mg/1.73 m2 given intravenously for three days as an initial therapy. Then the patients were given oral prednisone, 30 mg per day for one month; finally, daily doses were reduced by 5 mg every two weeks until the daily dose became 10 mg per day. Thereafter, daily doses were reduced by 1 mg every two weeks to reach the final dose of 0 mg.
At the latest follow-up, the patients were considered to have recovered if their proteinuria was <300 mg daily and if they did not show progression of renal function based on the values of serum creatinine at renal biopsy.
Results
In Table 1, the basic characteristics of elderly patients with HSP nephritis are shown.
Basic characteristics of five elderly patients with severe forms of HSP nephritis.
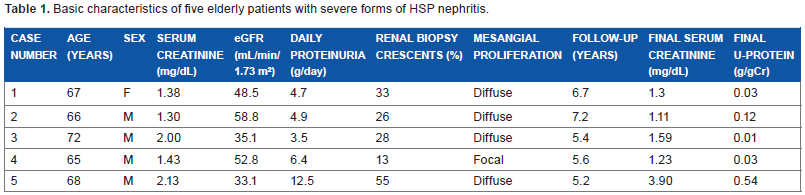
Proteinuria varied between 3.5 and 12.5 g per day. The levels of serum creatinine were between 1.30 and 2.13 mg/dL. Two patients were hypertensive prior to the treatment. The mean duration of follow-up, excluding one patient who died of adenocarcinoma of the lung, was 6.22 ± 0.86 years with a range of 5.6–7.2 years. At the latest follow-up, four patients had clinically recovered. No progression of renal function or side effects of the treatment was observed in four patients.
Discussion
The present study, although uncontrolled, strongly suggests that prednisolone semi-pulse therapy followed by gradual reduction of the doses of prednisolone may be beneficial in elderly patients with severe forms of HSP nephritis.
Up to now, there have been no decisive studies demonstrating the beneficial effects of methyl-PSL on renal function in elderly patients with HSP. In the pediatric field, Niaudet and Habib 12 reported the efficacy of methyl-PSL for patients with severe forms of HSP, such as nephrotic and/or nephritic syndrome. Also, some studies, although noncontrolled and nonrandomized, showed a favorable effect of initial high doses of steroid.13–15
Pillebout et al 16 have clearly demonstrated that the degree of proteinuria is a significant prognostic factor in adult patients with HSP. As far as we know, no other studies have demonstrated the baseline renal function. Some authors 17 have shown that the presence of a high percentage of crescents has an unfavorable effect, but this was not confirmed by others.18,19
Schaier et al 20 demonstrated that the clinical presentation of HSP is more severe in older patients and that renal prognosis for HSP nephritis in elderly is poor compared with what is observed in children. At diagnosis, progressive hypertension is an important factor, and elderly patients show significantly more hypertension than younger adults (<60 years).
In the present study, two patients had a previous history of hypertension at the time of diagnosis and were treated with antihypertensive agents of renin-angiotensin inhibitors; therefore, it is difficult to discuss the effects of simultaneous appearance of hypertension on the prognosis of severe forms of HSP.
Compared with the prognostic values of clinical manifestations, the importance of histopathological findings still remains controversial.
Recently, Pillebout et al 11 reported that no single class of glomerular lesions has a prognostic value by multivariate analysis. Among the acute lesions considered, the only histologic variable with an independent prognostic factor was the presence of glomerular fibrinoid necrosis.
On the other hand, Schaier et al 20 reported that the presence of crescents in the first biopsy did not seem to predict the outcome of HSP nephritis in adults, also supported by other studies.19,21 Similarly, Davin 9 proposed that the study of crescent pathophysiology might provide useful information for therapeutic strategy because the presence of crescents is a prominent histologic feature of HSP, representing an important prognostic factor and the basis for the International Study Group of Kidney Disease in childhood pathology classification. 22 As already mentioned, crescents are more often observed in HSP than in IgA nephropathy, and their number is related to the severity of clinical signs and to the prognosis of HSP in most children.23,24 In addition, Szeto et al 25 also reported that cellular crescents were detected in 31% of the cases and, when present, there were indications of poor prognosis. Moreover, of the acute glomerular lesions examined, only necrosis and cellular crescent were found to carry a prognostic significance and to correlate with an adverse renal outcome. Therefore, it is possible that therapy may have altered such glomerular lesions and thus the clinical course or disease progression, but no prospective studies have yet been reported to confirm such possibilities. By contrast, some studies demonstrated that chronicity factors, such as the percentage of interstitial fibrosis and global sclerotic glomeruli, are unfavorable risk factors. These variables are usually described in other glomerulonephritis, particularly IgA nephropathy.26,27
Moreover, Nickavar et al 28 demonstrated that there was a significant correlation between the severity of renal involvement and of proteinuria, which leads to ESRD. Szeto et al 25 proposed that the detection of acute lesions, such as glomerular necrosis and cellular crescent, combined with nephrotic syndrome will need treatment to prevent or to reduce the risk of ESRD.19,29
In line with these studies, our present small study examining the efficacy of early aggressive PSL therapy may provide some clinical hint for treatment of elderly patients with severe form of HSP.
Until now, there has been only one report discussing the cause of death in elderly patients with HSP. Pillebout et al 16 reported that the most frequent cause of death was neoplasia in 17 patients (27% of deaths), involving lung in 9 patients and upper respiratory and digestive tracts in 5. In all, 11 of the 17 patients dying of cancer never received any immunosuppressive treatment, 4 had been treated by corticosteroids alone, and 2 by corticosteroids associated with cyclophosphamide. Thus, they did not differ significantly from the remaining patients with regard to the treatment.
According to Pillebout et al's study, in the present series, one of five patients died of lung cancer, although no clear explanation of this frequent cause of death in patients with HSP is known.
In conclusion, our preliminary study, although small in number, suggests that renal outcome as well as survival of elderly patients with severe forms of HSP might be altered by aggressive prednisolone therapy. This was a single-center cohort study conducted in accordance with the Declaration of Helsinki.
Author Contributions
SK-O collected the data. HS followed up the patients and wrote the manuscript. TI analyzed the data. TK followed up the patients. HO supervised. All authors reviewed and approved of the final manuscript.