
Abstract
Fetal intestinal volvulus without malrotation is a rare, life-threatening disease. Left untreated, hemorrhage from necrotic bowel tissue will lead to severe fetal anemia and even intrauterine death. We encountered a case of fetal intestinal volvulus causing severe anemia, which was diagnosed postnatally and successfully treated with surgical intervention.
Introduction
Fetal intestinal volvulus is a very rare life-threatening condition, although prenatal diagnosis is difficult.1,2 We report herein a case of fetal intestinal volvulus without malrotation in which non-reassuring fetal status resulted from fetal anemia caused by hemorrhage from the small bowel, requiring resection of necrotic intestine and ileoileostomy.
Case Report
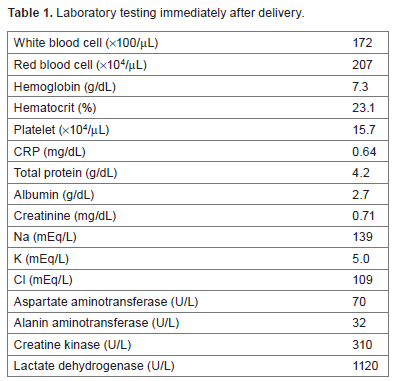
A 38-year-old multiparous woman presented to a referral hospital at 34 weeks and 4 days of gestation with a 2-day history of reduced fetal movement without abdominal pain. Cardiotocography (CTG) revealed non-reassuring fetal status and she was transferred to our hospital. Although precise ultrasonography was difficult because of maternal obesity (BMI, 39 kg/m2), no fetal movement was recorded and peak systolic flow velocity in the middle cerebral artery showed a high speed of 1.78 MoM, suggesting fetal anemia. CTG at our hospital, 5 hours after the first CTG, again showed non-reassuring fetal status, so we performed cesarean section and a female infant weighing 2494 g was delivered with Apgar scores of 6 at 1 minute and 8 at 5 minutes. Umbilical artery pH was 7.3 and base excess was -16. The infant showed a markedly distended abdomen with dark discoloration of the skin (Fig. 1) and laboratory testing revealed severe anemia (Table 1). Postnatal supine x-ray of the abdomen showed diffuse abdominal distension without gas passage through the stomach and bowel (Fig. 2) and contrast enema showed suspected stenosis of the terminal ileum (Fig. 3). In consideration of fetal diseases such as intussusception of the intestine, intestinal volvulus, and hemorrhagic tumor accompanying intestinal obstruction, exploratory surgery was performed immediately. Upon laparotomy, necrotic intestine easily tore and released a large amount of dark bloody fluid. Hence, intestinal volvulus was recognized (Fig. 4). The small bowel was resected from 40 cm distal to the ligament of Treitz to 2 cm proximal to the ileocecal valve. No intestinal atresia was identified. Transfusion of 80 mL of red cell concentrates and 30 mL of fresh frozen plasma was performed intraoperatively. Oral feeding was started from postoperative day 6 and the infant was discharged on postoperative day 26.
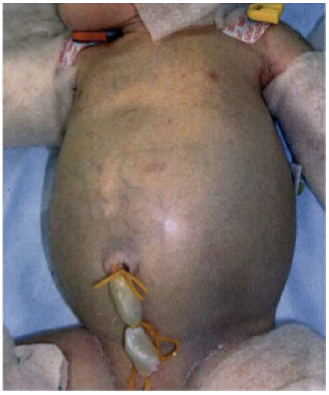
Markedly distended abdomen of the neonate with dark discoloration of the skin.

Postnatal supine x-ray of the abdomen showing diffuse abdominal distension without gas passage through the stomach or bowel.

Contrast enema showing suspected stenosis of the terminal ileum.
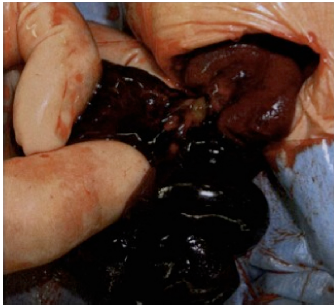
Necrotic intestine and intestinal volvulus easily tore, releasing a large amount of dark, bloody fluid.
Laboratory testing immediately after delivery.
Discussion
Congenital volvulus represents a twisting of loops of small bowel or a proximal part of the colon around the mesenteric artery or its branches, resulting in ileus and necrosis of the intestinal wall.3–5 As the condition worsens, the necrotic bowel perforates and causes hemorrhagic fetal ascites. At this stage, the mother may notice reduced fetal movements resulting from fetal anemia and CTG depicts non-reassuring fetal status.
Prenatal diagnosis of small intestinal volvulus is difficult due to the lack of typical signs, whereas midgut volvulus often displays a whirlpool sign on ultrasonography.1,2,6 In addition, differentiation from other diseases such as intestinal atresia and meconium peritonitis seems crucial, because of the major differences in subsequent management. Intestinal atresia shows a distended bowel proximal to the point of atresia and hypoplasia or a highly echogenic region distal. This condition can further develop to intestinal perforation, recognized as meconium peritonitis. 1 Although precise diagnosis is very difficult, key factors for management including decisions on whether to deliver the affected fetus might be gestational age at the time of diagnosis and signs of fetal anemia. If the gestational age is term or near-term without signs of fetal anemia, induction of labor might be one of the options to prevent possible ominous outcomes associated with further expectant management. On the other hand, urgent delivery should be taken into consideration in cases of suspected fetal anemia. With increased peak flow velocity in the middle cerebral artery in combination with non-reassuring fetal status on CTG, fetal anemia can be assumed.6,7 Our case required immediate delivery based on the findings of CTG and Doppler ultrasonography, necessitating surgical treatment and transfusion.
Affected fetuses with signs of anemia require careful attention to the differential diagnoses, including diseases requiring surgical intervention such as fetal volvulus.
Author Contributions
Provided patient care: KK, YS, YM, SN, MS. Analyzed the data: YK. Wrote the first draft of the manuscript: TN, DT. Contributed to the writing of the manuscript: DT. Agree with manuscript results and conclusions: HT, MK. Jointly developed the structure and arguments for the paper: MK. Made critical revisions and approved final version: MK. All authors reviewed and approved of the final manuscript.