
Abstract
Objectives
The purpose of this prospective, randomized study was to evaluate the effects of a diet containing eicosapentaenoic acid (EPA), docosahexaenoic acid (DHA), gamma-linolenic acid (GLA), and antioxidants in head and neck cancer surgery patients with free-flap reconstruction.
METHODS
In this randomized, prospective study, 62 patients with head and neck cancers were assigned to receive a general control diet (Ensure® H; Abbott Japan, Tokyo, Japan) or the study diet (Oxepa®; Abbott Japan) containing EPA, DHA, GLA, and antioxidants (eg vitamins A, E, and C). The primary assessment item was the degree of postoperative inflammation, as assessed by measuring maximum body temperature and levels of C-reactive protein (CRP) and procalcitonin from the day of surgery to postoperative day 8. Secondary assessment items were lengths of stays in the intensive care unit (ICU) and hospital.
Results
The control diet group (n = 32) and study diet group (n = 30) showed no significant difference in energy administered through diet. No significant differences in the parameters of the primary assessment item were noted. Length of stay in the ICU was significantly shorter for the control diet group than for the study diet group (P = 0.011). No significant difference in duration of hospitalization was seen between groups.
CONCLUSION
No usefulness of a diet containing EPA, DHA, GLA, and antioxidants was demonstrated.
Keywords
Introduction
Some nutrients exert influences on immunity and inflammatory reactions in humans. However, the extent to which nutrients affect the clinical course in seriously ill patients remains unclear. Effects are considered to vary with the type of intervention and patient characteristics. 1 Fatty acids (FAs) and antioxidants are representative pharmaconutrients exerting influences on inflammatory reactions. Omega-3 (O-3) FAs and omega-6 (O-6) FAs possess a common metabolic pathway, and their anti-inflammatory actions are regulated by the proportions of O-3 FAs and O-6 FAs. Eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) are representative O-3 FAs and gamma-linolenic acid (GLA) is a representative O-6 FAs. 2 Examples of antioxidant substances include vitamins C and E, 3 selenium, zinc, manganese, and iron. 4 While immunoenhancing diets, such as those including EPA, GLA, and antioxidants, have been suggested to potentially reduce inflammatory reactions, their actual clinical utility has remained controversial in reports of surgery for cancer, with some reporting their usefulness5,6 and some showing no efficacy.7–9 In 2009, Stableforth et al reported a meta-analysis of 10 trials investigating immunonutrition with head and neck cancer surgery. Little evidence of heterogeneity was seen. Pooled estimates showed a reduction in the length of hospital stay by 3.5 days, and no reduction in clinical complications. 10 In addition, immunoenhancing diets are more expensive than standard diets.
Published data have shown the benefits of postoperative enteral feeding. 11 Leading scientific societies such as the American Society for Parenteral and Enteral Nutrition (ASPEN) and the European Society for Clinical Nutrition and Metabolism (ESPEN) currently agree that enteral nutrition should be used as the method of choice in perioperative treatment.12,13 For advanced head and neck cancers, reconstruction with free flaps is necessary following lesion resection. Such operations are long and highly invasive. Also, since no resection of internal organ tissue is performed, as in the case of laparotomy or thoracotomy, patients who undergo such procedures are good candidates for postoperative tube feeding. The purpose of this prospective, randomized study was to investigate the efficacy of a diet containing EPA, DHA, GLA, and antioxidants for head and neck cancer surgery patients scheduled to undergo free-flap reconstruction.
Patients and Methods
Patients and treatment
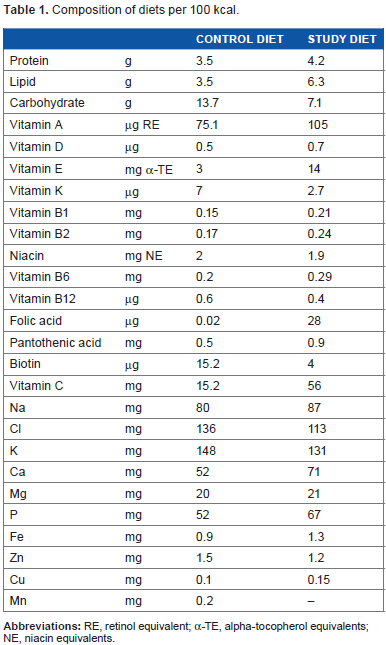
This study was carried out in the Department of Head and Neck Surgery and the Department of Otolaryngology at Tokyo Medical University Hachioji Medical Center between January 2010 and April 2013. Subjects comprised 62 of 69 patients diagnosed with head and neck cancers who had undergone free-flap reconstruction, excluding those who underwent reconstruction using a free jejunal flap. After obtaining informed consent to participate in the study, patients were randomly assigned to a control diet group (Ensure® H; Abbott Japan, Tokyo, Japan) or a study diet group (Oxepa®; Abbott Japan). Random assignment was performed using a sealed envelope system with numbers from a code table created from a random number table. The first author, Tsukahara K, generated the random allocation sequence and assigned participants to interventions. The mechanism used to implement the random allocation sequence was concealed until interventions were assigned. Ingredients in the control and study diets are listed in Table 1, and fat compositions are provided in Table 2. At 150 kcal/100 mL, energy concentrations were the same for both diets.
Composition of diets per 100 kcal.
FA information.
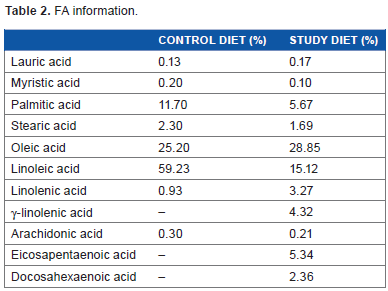
The fat source for the control diet was corn oil alone, which naturally delivers 59% linoleic acid and 25.2% oleic acid. Corn oil was selected because of the rich content of essential FAs. For the study diet, fish oil, canola oil, and borage oil were blended to deliver EPA, DHA, and GLA to the target levels that have been shown to improve the pulmonary failure ratio in patients with acute lung injury (ALI) and acute respiratory distress syndrome (ARDS). This fat blend was determined based on various in vivo and vitro studies.14–17 The study diet was selected for this study because EPA and GLA are known to control inflammation reactions in stressed patients. Linoleic acid is known to be proinflammatory, and the differences in the characteristics of these FAs were also within the scope of the study to compare the study and control diets. As yet, no reports have described adverse events in which either formula evoked inflammation in patients. Oleic acid is known to be stable against oxidation and appropriate as a fat source for enteral nutrition. Both blends are commercial formulas without any specific modification added for this study, although the control diet is a pharmaceutical formula for prescription use. Addition of selenium to food formulas is not permitted in Japan. The control diet did not include selenium, as the formula was developed for postoperative nutritional support to deliver generally required nutrients without fortification of specific nutrients. Supplementation with vitamins A, E, and C is easily achieved with individualized injections or oral formulations. Although, representing only fortification of two- to four-fold, these fortified levels are higher than in most commercially available enteral formulas. These levels of fortification were thought to be sufficient to compensate for the oxidative stress arising from ventilation in ALI and ARDS patients that was the original target of the study diet.17–19 Vitamin K functions as an integral part of the coagulation system and may not be appropriate for intensive care unit (ICU) patients. Vitamin K can also generally be synthesized in the necessary amounts in the human body, so fortification in the study formula was considered unnecessary. The control diet was a pharmaceutical formula developed for general postoperative patients and as such included vitamin K to satisfy general nutrition needs. We did not consider that the low vitamin K level in the study formula would affect the study outcomes. The study diet was developed as an upgraded version of a formula for chronic obstructive pulmonary disease (COPD) with the major fat source as canola oil, a source of oleic acid in the formula. The fat source for the study formula was changed to fish oil and borage oil to increase the amounts of EPA and GLA as well as antioxidant vitamins for ALI and ARDS patients to improve outcomes.16,19
We calculated a standard weight from the height for a body mass index of 22. Basal metabolic rate was determined as follows: standard weight x 30 kcal/kg/day. The target amount of energy administered was calculated as follows: basal metabolic rate x activity index (1.1). Administration of the diet via nasogastric tube was commenced within 24 hours of completing surgery, starting at 20–50 mL/hour or 30–75 kcal/hour and then adjusted as appropriate. After commencing administration, adjustment was made to achieve 75% of calculated calorie requirement within 72 hours.
The period of administration for both the control and study diet was determined as a minimum of 4 days, including day 1 of administration. The target daily water intake, including water content of the diet, was set at weight x 30 mL or administered energy amount x 1 mL, whichever was greater, and was administered as a flush, before and after administration of the diet, and at the time of giving medications. During the administration period of the control or study diet, no other enteral nutrients or fat emulsions were administered. Depending on the overall condition of the patient, based on the judgment of a doctor, fluid replenishment was conducted as appropriate and antibiotics or other drugs were administered. Rehabilitation of swallowing was started from postoperative days 7–10. Administration of the diet via nasogastric tube was used until sufficient oral food intake was resumed. Discharge from the hospital was determined once the wound, general condition, and oral food intake had stabilized.
The present study was approved by the Ethics Committee of Tokyo Medical University (IRB number 1201) and conducted in accordance with the Declaration of Helsinki. The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional guidelines on human experimentation and with the 1975 Declaration of Helsinki, as revised in 2008. We obtained written informed consent from all participants prior to enrollment. The study was registered at University Hospital Medical Information Network Center (UMIN; http://www.umin.ac.jp: ID000013158). The authors confirm that all ongoing and related trials for this drug/intervention are registered.
Participation criteria
Inclusion criteria
Patients were required to be Japanese, ≥20 years old, and to have undergone head/neck cancer surgery using a free flap (excepting jejunum surgery cases, no laparotomy). Patients had to have the possibility of nutritional supplementation via enteral nutrition beginning within 24 hours of surgery, for at least 5 days. In addition, patients or a suitable family member/relative had to provide voluntary, written, informed consent for participation.
Exclusion criteria
Patients meeting any of the following criteria were excluded: pregnancy or lactation; very short vital prognosis (expectation of survival <28 days); recent stroke or subarachnoid hemorrhage; non-functioning ileus or intestinal tract; significant immunosuppression (leukocytes <1000 cells/mm3); infection with human immunodeficiency virus; hyperlipidemia (triglycerides >500 mg/dL; total cholesterol >300 mg/dL); unsuitability for enteral nutrition; recent gastrointestinal hemorrhage; poorly controlled diarrhea; congenital metabolism disorder; milk protein intolerance; acute nephritis, nephrosis, or end-stage renal disease requiring strict limitation of protein and electrolytes; cardiac failure accompanied by nausea, vomiting, or diarrhea; participation in another trial within 30 days prior to registration for this present trial; or other reasons to be judged unsuitable by the principal investigator or sub-investigator.
Assessments
The primary assessment item was degree of postoperative inflammation, as assessed by maximum body temperature and levels of C-reactive protein (CRP) and procalcitonin from the day following surgery to postoperative day 8. Secondary assessment items were lengths of stays in the ICU and hospital.
Statistical analysis
We determined power with reference to the study by Ryan et al, 20 and calculated that 60 patients would be required. Enrollment for the present study was stopped at 62 patients, as the target for patients able to be analyzed had been reached. SAS version 9.3 software (SAS Institute, Cary, NC, USA) was used for all analyses. Two-way repeated-measures analysis of variance was utilized to determine factors affecting therapeutic efficacy and their 95% confidence intervals. Values of P < 0.05 were taken as statistically significant. All analyses were performed according to intention to treat and were conducted on the population of qualified subjects in whom part or all of the protocol had been conducted. All values are indicated as mean ± standard deviation.
Results
Patient characteristics
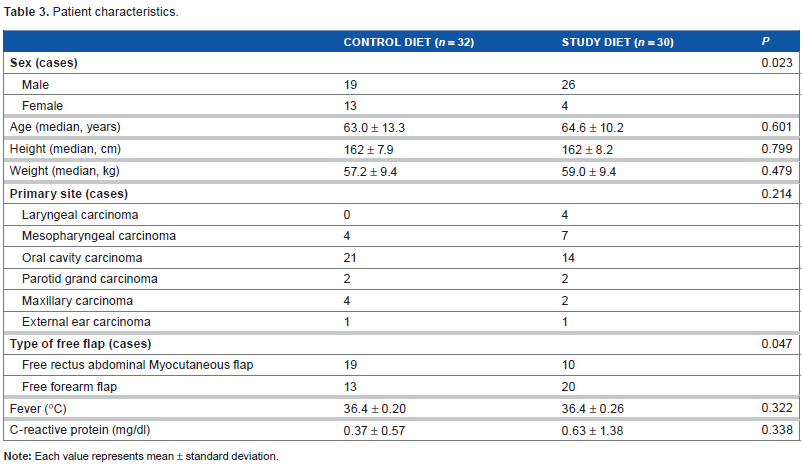
Thirty-two subjects were allocated to the control diet group and 30 to the study diet group (Fig. 1). Patient characteristics are shown in Table 3. The control diet group included 19 men and 13 women, with a mean age of 63.0 ± 13.3 years, median height of 162 ± 7.9 cm, and median weight of 57.2 ± 9.4 kg. The study diet group comprised 26 men and 4 women, with a mean age of 64.6 ± 10.2 years, median height of 162 ± 8.2 cm, and median weight of 59.0 ± 9.4 kg. No significant differences in age, weight, or height were evident between groups. Underlying diseases in the control diet group were mesopharyngeal carcinoma in 4 cases, oral cavity carcinoma in 21 cases, parotid gland carcinoma in 2 cases, maxillary carcinoma in 4 cases, and external ear carcinoma in 1 case. Reconstruction was conducted using a free rectus myocutaneous flap (free RAM flap) in 19 patients and free forearm flap (free FA flap) in 13 patients. Underlying diseases in the study diet group were laryngeal carcinoma in 4 cases, mesopharyngeal carcinoma in 7 cases, oral cavity carcinoma in 14 cases, parotid gland carcinoma in 2 cases, maxillary carcinoma in 2 cases, and external ear carcinoma in 1 case. Reconstruction was conducted using a free RAM flap in 10 patients and free FA flap in 20 patients. Preoperative body temperature was 36.4 ± 0.26°C in the control diet group and 36.4 ± 0.20°C in the study diet group. Preoperative CRP levels were 0.63 ± 1.38 mg/dL in the control diet group and 0.37 ± 0.57 mg/dL in the study diet group. No significant differences between groups were identified for any item.
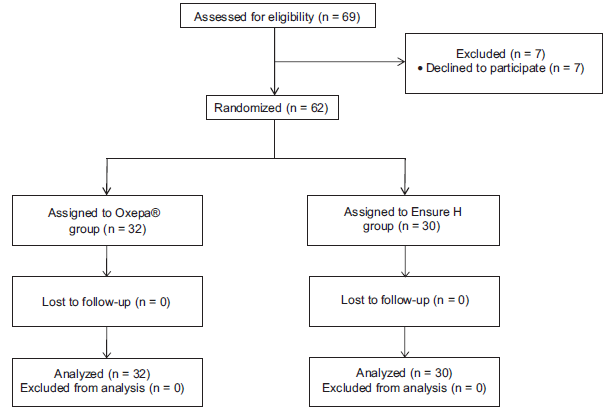
Consolidated standards of reporting trials (CONSORT) diagram.
Patient characteristics.
Administered energy of diets
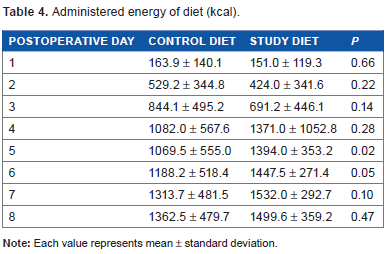
All patients were fed via the nasogastric tube for at least 8 days. Administered energy amounts for diets are shown in Table 4. In day 5, energy intake was significantly larger in study group. Excluding day 5, no significant differences were evident between groups. The result of analysis of variance for continuous measurements was P < 0.001, indicating no significant difference between groups.
Administered energy of diet (kcal).
Serum biochemistry (maximum body temperature, CRP, procalcitonin)
Serum biochemistry data are shown in Table 5 and Figure 2.
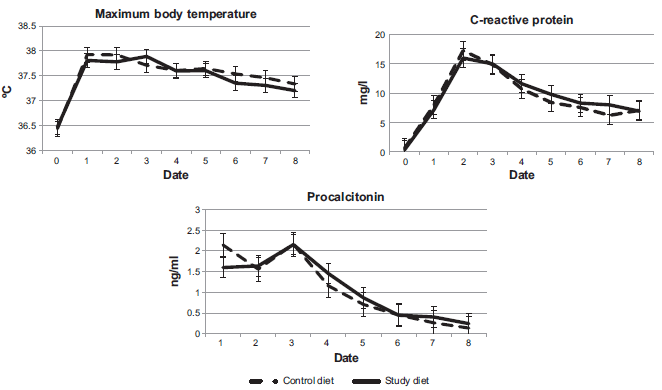
Serum biochemistry.
Serum biochemistry.
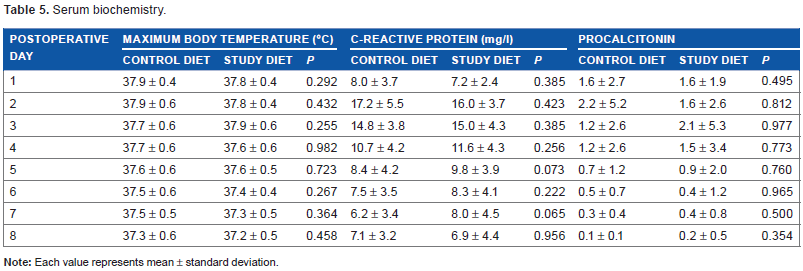
Again, no significant differences between groups were seen for any of the measured parameters (maximum body temperature, leukocyte count, CRP, and procalcitonin) on any of the days.
The result of analysis of variance for continuous measurements was P < 0.001, indicating no significant difference between groups.
Lengths of stays in the ICU and hospital
The length of stay in the ICU was significantly shorter for the control diet group (2.87 ± 0.43 days) than for the study diet group (3.24 ± 0.64 days; P = 0.011).
The length of stay in the hospital did not differ significantly between the control diet group (64.4 ± 39.5 days) and the study diet group (63.4 ± 32.7 days; P = 0.508).
Discussion
In the present study, no usefulness of a diet containing EPA, GLA, and antioxidants was demonstrated for postoperative head and neck cancer patients with free-flap reconstruction. No significant differences were observed for any of the primary assessment parameters of maximum body temperature, CRP or calcitonin, or for the duration of hospitalization. However, the length of stay in the ICU was significantly shorter for the control diet group. In addition, energy intake was larger in the study group on days 4–8, for unknown reasons. Oxepa®, which was used as the study diet, is an immunoenhancing diet that contains the O-3 FAs, EPH and DHA, and the O-6 FAs, GLA, along with an enhanced antioxidant content. In contrast, the control diet of Ensure® H is a standard, non-immunoenhancing enteral nutrition diet with low antioxidant content. The safety of both diets has been demonstrated in clinical trials conducted worldwide. 7 Because no studies of Oxepa® versus Ensure® H in the field of head and neck cancer have been conducted to date, we conducted the present randomized controlled trial study in which intention-to-treat analysis was conducted.
An immunoenhancing diet has been found to modulate both the hyperinflammatory and compensatory phases. 21 On the other hand, a meta-analysis that included 22 randomized trials of immunonutrition in postoperative and critically ill patients did imply a significant reduction in infective complications, but showed no improvement in mortality. 1 Another meta-analysis of 21 randomized trials involving major gastrointestinal surgery concluded that immunonutrition decreased morbidity and hospital stay, but not mortality rates. 22 The wide disparity in results from more than 30 randomized trials aimed at assessing the clinical significance of immunonutrition over the past two decades limits the ability to draw firm conclusions. In addition, results in the field of cancer surgery have been mixed and controversial.5–9 Infective complication rates have been shown to be reduced in cancer patients receiving immunoenhancing diet,23,24 but the data in those studies were not analyzed on an intention-to-treat basis. 7 Another prospective, randomized, controlled, double-blind study failed to demonstrate any reduction in infective complications with a perioperative immunoenhancing diet in upper gastrointestinal cancer patients. 25 A further prospective randomized study showed no benefit from an immunoenhancing diet administered postoperatively in patients with upper gastrointestinal malignancies. 26 In 2009, Stableforth et al reported a meta-analysis of 10 immunonutrition trials in head and neck cancer surgery. Little evidence of heterogeneity was identified. Pooled estimates showed a reduction in the length of hospital stay of 3.5 days, and no reduction in clinical complications. 10 Stableforth et al stated that the reasons for the reduction in postoperative hospital stay without improvement of other outcomes were “unclear.” 10 Similarly, we are uncertain why the length of stay in the ICU was significantly shorter for the control diet group than for the study diet group in the present study. Klek et al studied perioperative immunonutrition in 776 patients undergoing gastric or pancreatic resections and concluded that the type of postoperative nutrition was of no importance in well-nourished patients, whereas enteral immunonutrition helped to improve treatment outcomes in malnourished patients. 27 When initially examined, 30–50% of head and neck cancer patients were found to be in a poor state of nutrition.28,29 In the present study, given the initial heights of control and study diet group subjects of 162 ± 7.9 cm and 162 ± 8.2 cm, respectively, and body weights of control and study diet group subjects of 57.2 ± 9.4 kg and 59.0 ± 9.4 kg, respectively, we consider that patients were not in a poor state of nutrition preoperatively. One possible contributor to the study results was that our patients were well nourished preoperatively. This study was performed in a single institute, Tokyo Medical University Hachioji Medical Center. A multicenter study of preoperative nourishment with a larger sample size might be required.
Expression of human leukocyte antigen (HLA)-DR is crucial in the specific immune response to infection, and HLA-DR expression is reduced on the T lymphocytes of patients who develop postoperative infections. 30 When administering Oxepa®, the same diet used in the present study, to esophagogastric cancer patients for 7 days before and after surgery, Sultan et al 7 observed that immunonutrition with O-3 FAs did not affect overall HLA-DR expression on leukocytes, despite a significant increase in plasma concentrations of O-3 FA. Furthermore, Sorensen et al 8 administered O-3 FAs (EPA and DHA) to patients undergoing elective surgery for colorectal cancer for 7 days prior to surgery and conducted a granulocyte FA analysis on the day of operation. From the results, they concluded that preoperative oral supplementation with O-3 FAs for 1 week can change the FA composition of granulocyte membranes. However, postoperative changes in the FA composition of granulocyte membranes were not studied. Osland et al reported a systematic review and meta-analysis regarding the clinical effects of the timing of immunonutrition administration to 2005 patients. 31 Significant reductions in infectious complications and length of hospital stay were found with peri- and postoperative administration, while preoperative immunonutrition provided no clear advantage over standard nutrition. In our study, administration of immunonutrition was performed peri- and postoperatively. We therefore consider that the methods applied in this study were appropriate.
Immunoenhancing diets are more expensive than standard diets: Oxepa® costs 799 Ƀ/can, while Ensure® H costs 270 Ƀ/can. If the clinical effects of standard diets are the same as immunoenhancing diets, this represents a meaningful finding in terms of medical economics. The present study did not demonstrate any usefulness for a diet containing EPA, GLA, and antioxidants among postoperative head and neck cancer patients with free-flap reconstruction. We hope that this study will contribute to the controversial discussion about providing an immunoenhancing diet for cancer patients treated by surgery.
Author Contributions
Conceived and designed the experiments: KT, RM, KN. Analyzed the data: KT, YU. Wrote the first draft of the manuscript: KT. Contributed to the writing of the manuscript: KT, RM, KN. Agree with manuscript results and conclusions: KT, RM, HS, ME, YU, KN. Jointly developed the structure and arguments for the paper: KT, YU. Made critical revisions and approved final version: KT, RM, HS, ME, KN. All authors reviewed and approved of the final manuscript.
Footnotes
Acknowledgment
The authors are indebted to Prof. Mamoru Suzuki (Department of Otolaryngology, Tokyo Medical University, Tokyo, Japan) for his critical comments on this manuscript.