
Abstract
Purpose
We examined the cross-sectional association between lung function and metabolic syndrome (MetS), independent of fasting immunoreactive insulin (F-IRI).
Methods
A total of 3,072 middle-aged, apparently healthy subjects who participated in a general health check-up were included. Lung function, which was expressed as forced vital capacity (%FVC predicted) or forced expiratory volume in 1 second (FEV1% predicted) was examined. Multivariable logistic regression analysis was performed to assess the association between lung function and MetS.
Results
Men with the lowest quartile of FVC% predicted, or those with the lowest quartile of FEV1% predicted, had a 3.5-fold or 2.6-fold increased risk of MetS, respectively, compared with those with the highest quartile of FVC% predicted or FEV1% predicted. F-IRI had a positive, significant, and independent association with MetS in both sexes.
Conclusion
Impaired lung function increased the risk of MetS, independent of F-IRI and smoking in men, but not in women.
Keywords
Introduction
Metabolic syndrome (MetS) is a condition clustered with abdominal obesity, elevated glucose and blood pressure, and dyslipidemia. It is closely associated with the development of type 2 diabetes and cardiovascular disease (CVD).1,2 However, the mechanisms involved in the pathways of MetS have not yet been completely clarified. There are controversies surrounding whether obesity or insulin resistance causes MetS, or whether all of these are consequences of inflammation.3,4
On the other hand, reduced lung function is independently associated with MetS, 5 and impaired lung function exists before the development of MetS. 6 So, reduced lung function and MetS may share the common pathophysiological grounds. However, to our knowledge, no studies have examined the association between lung function and MetS while taking into account insulin concentrations. This study has investigated the cross-sectional association between lung function and MetS, independent of fasting insulin concentrations, among apparently healthy Japanese men and women.
Materials and Methods
Subjects
The Kurihashi Lifestyle Cohort Study comprises a total of 7,363 subjects enrolled in a general health examination program at Saitama-ken Saiseikai Kurihashi Hospital (Saitama, Japan) from October 2006 to September 2007. For the current analysis, the following criteria were used for excluding individuals: missing data on spirometry (n = 4,677) or fasting insulin concentrations (n = 3,780); having cancer, endocrine, respiratory, or congestive heart disease (n = 172); a diagnosis of diabetes (n = 39); currently under pharmacological treatments for hypertension (n = 421) or dyslipidemia (n = 90); and missing data on relevant covariates (n = 40). Because pharmacological treatments for hypertension, dyslipidemia, and diabetes probably influence insulin sensitivity, the patients who had been treated by medications for hypertension, dyslipidemia, and diabetes were excluded, and the remaining 2,020 men and 1,052 women were used for the current data analysis.
Methods
The health check examination of this study includes self-administrated questionnaires regarding smoking (never = 0; otherwise, pack-years of cigarettes in ever-smokers were determined) and alcohol intake (never, occasionally, and regularly); physical activity during leisure time (sedentary, occasionally, active); a family history of diabetes (yes or no); as well as physical examinations, biochemical tests, chest X-rays, and electrocardiograms.
Venous blood samples were collected in the morning after an overnight fasting state for more than 10 hours. Fasting plasma glucose (FPG) (glucose oxidase method), fasting immunoreactive insulin (F-IRI) (enzyme immunoassay method), triglycerides (TG) (enzymatic method), and high-density lipoprotein cholesterol (HDL-C) (direct method) were measured in the commercial laboratory. The intraassay coefficient of variation for FPG, F-IRI, TG, and HDL at values of 5.33 mmol/L, 7.6 µ/mL, 0.44 mmol/L, and 0.90 mmol/L was 2.0%, 3.4%, 1.3%, and 1.1%, respectively. The corresponding values for the interassay coefficient of variation was 0.0%, 2.1%, 0.3%, and 0.4%, respectively.
Systolic blood pressures (sBP) and diastolic blood pressures (dBP) were measured with patients in the sitting position after a 5-minute rest using an automated device (OMRON, Kyoto, Japan). Waist circumference (Wc) was measured at the level of umbilicus at the end of the expiration of a normal breath, and with the subject in a standing position.
The International Diabetes Federation's definition of MetS (IDF-MetS) 7 was modified and used to identify subjects with MetS in the current study: those with central obesity (defined as Wc ≥90 cm for men and ≥80 cm for women in Japan); and those with any two of the following four factors - 1) raised TG: ≥1.7 mmol/L; 2) reduced HDL: <1.03 mmol/L in men and <1.29 mmol/L in women; 3) raised BP: sBP ≥ 130 mmHg or dBP ≥ 85 mmHg; and 4) raised FPG ≥ 5.6 mmol/L.
The pack-years of cigarettes were calculated using the Brinkman index, which is defined as the number of cigarettes smoked · day−1 X number of years smoked (to convert to pack-years, divide by 20).
Lung function
Lung function tests were carried out in every participant by an experienced technician using a spirometer (HI-701; CHEST, Tokyo, Japan). The crude data on forced vital capacity (FVC) or forced expiratory volume in 1 second (FEV1) were divided by predicted FVC or predicted FEV1, respectively, to yield FVC% predicted and FEV1% predicted. The predicted FVC or predicted FEV1 for men were calculated by the formula designed for Japanese individuals by the Japanese Respiratory Society 8 :

and for women

The FVC% predicted and FEV1% predicted were stratified by quartiles in men and women, respectively, and they were used in the logistic regression analysis described in the following section.
Statistical analysis
Statistical analyses were performed and reported separately for men and women. The chi-squared test was used to compare proportions, and Student's t-test was used to compare means between independent two groups.
The potential relationship between lung function (FVC% predicted, FEV1% predicted) and F-IRI, as well as variables defining modified IDF-MetS (FPG, BPs [sBP, dBP], lipids [TG, HDL-C]) was investigated by univariate linear regression analysis. As for TG or F-IRI, log transformed values were used to obtain the values that follow a normal distribution. Next, variables independently associated with lung function were analyzed by multivariable linear regression analysis. The independent variables used in the analysis included pack-years of cigarettes and menopause status (only for women). Further additional adjustment for F-IRI was performed to assess whether the association between lung function and identified variables was independent from the F-IRI concentrations.
The logistic regression analysis was performed to assess what factors, including lung function, related to the presence of the modified IDF-MetS. The variables that were identified as significant in the univariate model were included in the multivariable logistic regression model. The independent variables used in the analysis included age (continuous), pack-years of cigarettes (continuous), physical activity during leisure time (categorical), alcohol habits (categorical), F-IRI (continuous), FVC% predicted (continuous), FEV1% predicted (continuous), and (in women only) menopause status (categorical). The unadjusted and adjusted odds ratios (ORs) and their 95% confidence intervals (CIs) for the presence of modified IDF-MetS were calculated and reported.
The Kurihashi Lifestyle Cohort Study was approved by the Institutional Review Board of Saitama-ken Saiseikai Kurihashi Hospital (Saitma, Japan), as well as Tokyo Women's Medical University (Tokyo, Japan), and written informed consent was obtained from the participants.
Data were analyzed with the SPSS statistical package for Windows version 21.0 (IBM Corporation, Armonk, NY, USA). P-values were based on two-sided tests, and the cut-off point for statistical significance was P < 0.05.
Results
Characteristics of study subjects
The participants’ mean age was 50 ± 8 years and the mean body mass index was 23.2 ± 3.1 kg/m2. The mean FVC% predicted and FEV1% predicted were 108% ± 14% and 100% ± 14%, respectively (Table 1). Men had significantly worse cardiovascular risk profiles and lower FVC% predicted or FEV1% predicted than women (Table 1). The proportion of men and women with the modified IDF-MetS was 12.9% and 10.6%, respectively.
Characteristics of men and women analyzed for the study.
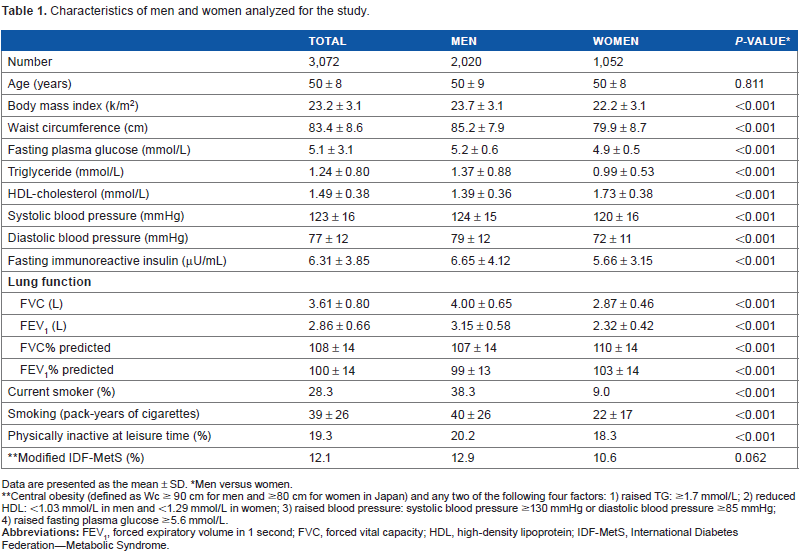
Data are presented as the mean ± SD.
Men versus women.
Central obesity (defined as Wc ≥ 90 cm for men and ≥80 cm for women in Japan) and any two of the following four factors: 1) raised TG: ≥1.7 mmol/L; 2) reduced HDL: <1.03 mmol/L in men and <1.29 mmol/L in women; 3) raised blood pressure: systolic blood pressure ≥130 mmHg or diastolic blood pressure ≥85 mmHg; 4) raised fasting plasma glucose ≥5.6 mmol/L.
Lung function and variables related to modified IDF-MetS
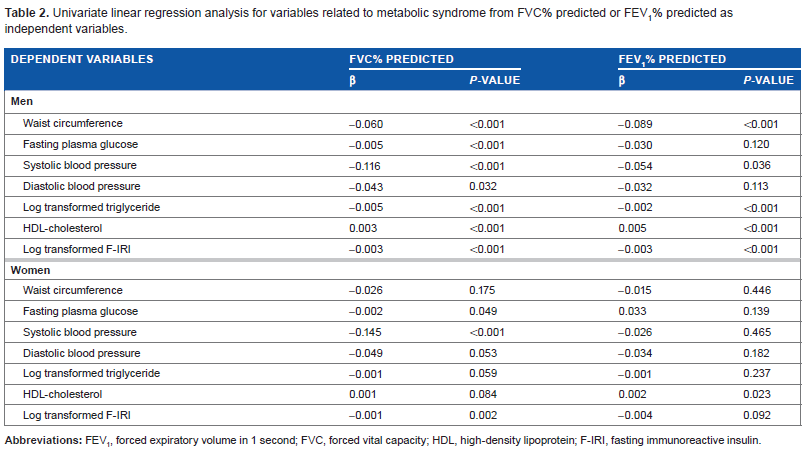
The univariate linear regression analysis showed a significant effect of lung function either on the components of modified IDF-MetS and on F-IRI in men (Table 2). The components of the modified IDF-MetS deteriorated and F-IRI increased with declining lung function (Table 2). In women, the significant association was shown between FVC% predicted and FPG, sBP, and F-IRI, and between FEV1% predicted and HDL-C (Table 2).
Univariate linear regression analysis for variables related to metabolic syndrome from FVC% predicted or FEV1% predicted as independent variables.
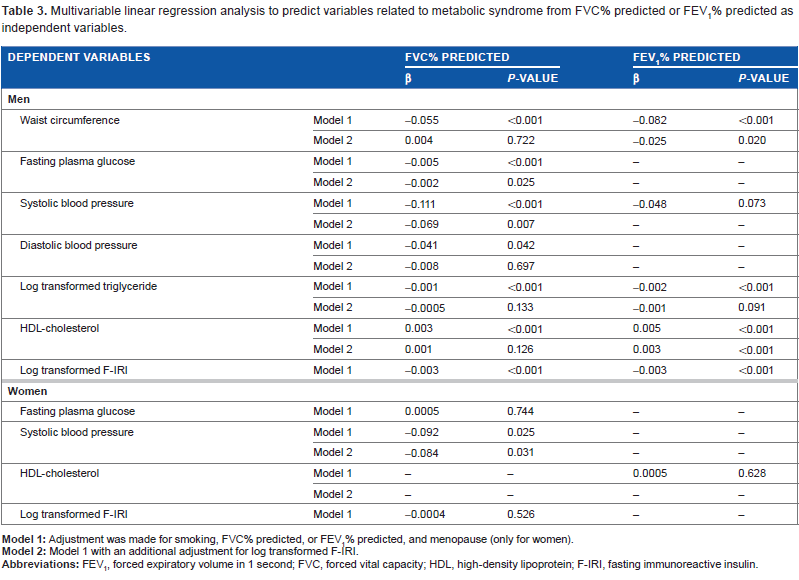
The multivariable linear regression analysis showed that the relationship between FVC% predicted and the components of modified IDF-MetS remained significant after adjusting for smoking (pack years of cigarettes) in men (Table 3). However, this significant association remained only for FPG and sBP, after making an additional adjustment for F-IRI. The relationship between FEV1% predicted and Wc or HDL-C remained significant after additional adjustment for smoking (pack-years of cigarettes) and F-IRI in men (Table 3). In women, the association between FEV1% predicted and sBP remained as significant after adjusting for smoking (pack-years of cigarettes), menopause, and F-IRI (Table 3).
Multivariable linear regression analysis to predict variables related to metabolic syndrome from FVC% predicted or FEV1% predicted as independent variables.
Lung function and the modified IDF-MetS
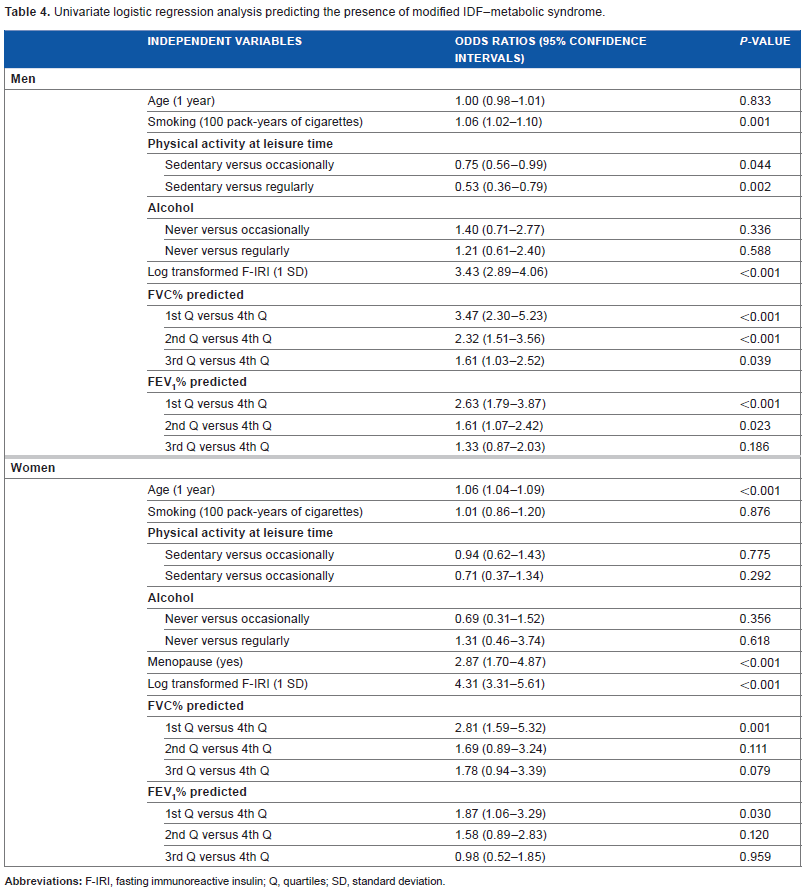
The univariate logistic regression analysis showed that smoking (pack-years of cigarettes), physical activity at leisure time, F-IRI, and lung function (FVC% predicted and FEV1% predicted) had significant association with the presence of the modified IDF-MetS in men (Table 4). In women, age, menopause, F-IRI, FVC% predicted, and FEV1% predicted had a significant association with modified IDF-MetS (Table 4).
Univariate logistic regression analysis predicting the presence of modified IDF–metabolic syndrome.
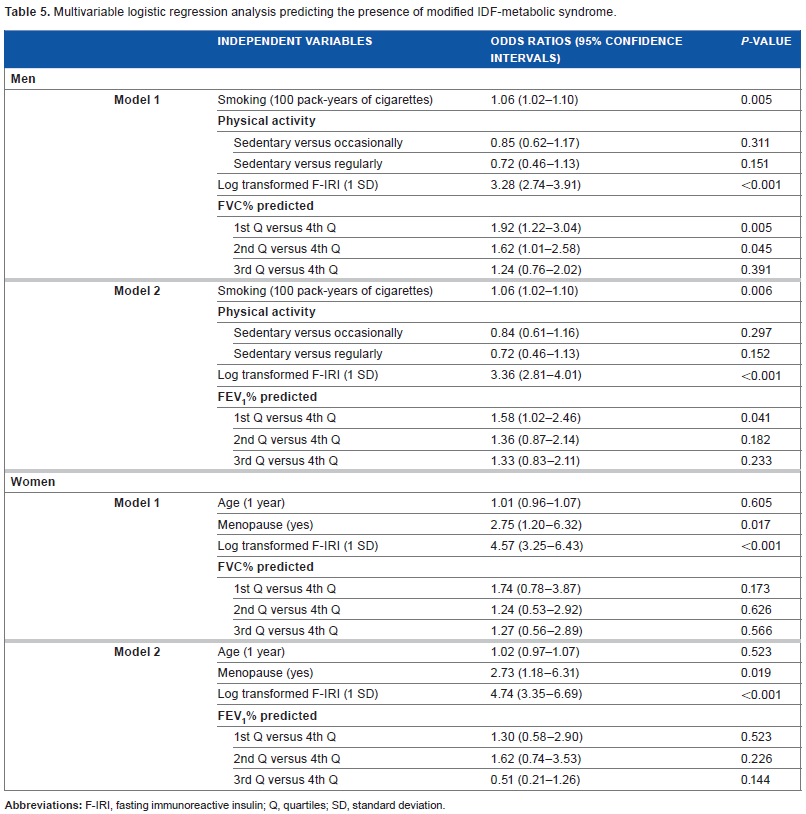
The multivariable logistic regression analysis showed that smoking (pack-years of cigarettes), F-IRI, and FVC% predicted or FEV1% predicted had a significant and independent association with the presence of the modified IDF-MetS in men (Table 5). Men with the lowest quartiles of FVC% predicted or of FEV1% predicted had a 1.92-fold or 1.58-fold increased risk of modified IDF-MetS compared with those with the highest quartiles of FVC% predicted or of FEV1% predicted (Table 5). In women, menopause and F-IRI had a positive and independent association with the presence of the modified IDF-MetS. However, either FVC% predicted or FEV1% predicted did not have a statistically significant association with the presence of the modified IDF-MetS (Table 5).
Multivariable logistic regression analysis predicting the presence of modified IDF-metabolic syndrome.
Discussion
The cross-sectional association between lung function and MetS has been previously reported in men and women.5,9–12 However, it was unknown whether this association occurred independently of F-IRI concentrations. In the current study, the risk of modified IDF-MetS increased with the reduction of lung function, independently of F-IRI and smoking in apparently healthy Japanese men, but not in women.
MetS had an association with lung dysfunction9–12 in a particularly restrictive pattern, exhibiting an FVC < 80% of the predicted value and an FEV1-to-FVC ratio >0.7. Due to a very small number of cases with serious lung impairments (the proportion of people with an FVC < 80% was 8.4% and that with an FEV1-to-FVC ratio <0.7 was 6.8%), we could not analyze our data in the same manner as was conducted in previous studies.9–12 Nevertheless, lung dysfunction with restrictive, rather than obstructive, patterns seemed to have stronger associations with modified IDF-MetS in our study, although the reason for this was not known.
Lung dysfunction has also been reported as a risk factor for developing diabetes, 13 hypertension, 14 and CVD 15 in prospective studies. These associations may be partly explained by the adverse effect associated with lung volumes and compliance due to obesity,5,9,10 systemic inflammation,16,17 insulin resistance, 18 and adverse early-life exposures. 19 Leone et al 20 have reported that the association between lung dysfunction and MetS based on the definition according to the American Heart Association/National Heart, Lung, and Blood Institute (in which abdominal obesity accounts for three of five components of MetS) was predominantly due to abdominal obesity. 21 In the current study, abdominal obesity, which is the essential component of IDF-MetS, was independently associated with lung function, and lung function was independently associated with modified IDF-MetS in men. These findings might be a reflection of the fact that obesity leads to a decrease in chest wall compliance and an increase in peripheral airway resistance. Systemic inflammation markers such as C-reactive protein (CRP), leukocytes, and fibrinogen were associated with lung dysfunction,16,22,23 while biomarkers of inflammation and endothelial dysfunction have been associated with MetS.22,23 Moreover, elevated serum leptin levels are reported in subjects of normal body weight with impaired lung function, 24 and this would promote inflammation. Alternatively, the decreased skeletal muscle strength leads to a decline in lung function and an increase in insulin resistance, because skeletal muscles play an important role in insulin-mediated glucose disposal. 25
In contrast to Japanese men, almost no association was shown between lung function and the components of MetS, including Wc, in Japanese women. There may be a difference in the way that the distribution of fat affects the thoracic mechanics in men when compared to women. 26 Women develop peripheral adiposity more often, whereas men are more prone to central obesity. 27 Visceral fat is an important source of free fatty acids and inflammatory mediators that affect hepatic glucose and fat metabolism, and it likely contributes to the development of hepatic insulin resistance. 28 In women, body fat distribution shift to a more male pattern following menopause. Since both pre- and postmenopause women were included in our study, women with various patterns of adiposity were included, and this may have influenced our results. Moreover, the sex hormone, estrogen, may influence the association between lung function and MetS in women.
The strength of the study is that the association between lung function and MetS together with F-IRI was evaluated in both men and women, separately. In addition, we used predicted FVC% and FEV1% with the formula defined by the Japan Respiratory Society. 8 Since we repeated the same analysis using the international formula for the predicted FVC as well as for the FEV1, according to Baldwin et al 29 and Berglund et al, 30 our results did not change. There are several limitations. First, there was selection bias since not all participants had data pertaining to lung function and F-IRI. As shown in Table 6, the individuals analyzed in the study were older but had healthier CVD risk profiles than those who were not analyzed in the study. Thus, our results should be carefully generalized to the broader population. Second, as discussed above, elevated CRP (as a marker of inflammation) is associated with lung dysfunction, insulin resistance, and MetS.22,23 However, we were unable to assess this relationship due to a lack of data for CRP in our study. Third, although the hyperinsulinemic–euglycemic clamp is the standard technique that is used to measure insulin sensitivity, we used the F-IRI concentration as a surrogate measure of insulin resistance. Given that our subjects were participants in general health check-ups, it was impossible to perform such expensive, invasive, and long-term examinations. F-IRI reflects hepatic insulin resistance; however, it has a 70% correlation with peripheral insulin resistance. 31 Fourth, the questionnaire of physical activity, alcohol consumption, and smoking status was based on self-reported data, it was customized, and it had had not been validated prior to the study. Fifth, our study is based on the health examination data regarding biological markers and lung function, which was obtained at a single time, and this might have led to the misclassification of individuals.
Comparison of characteristics between individuals who were analyzed and not analyzed in the study.
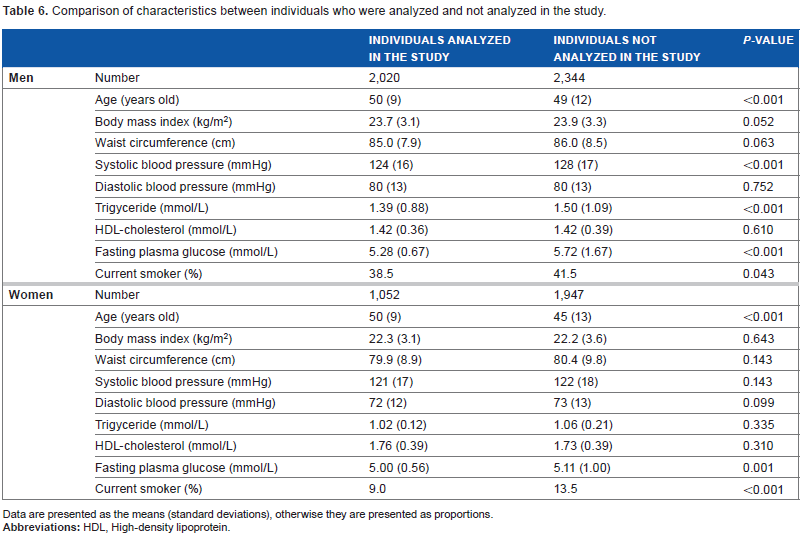
Data are presented as the means (standard deviations), otherwise they are presented as proportions.
In conclusion, impaired lung function increased the risk of modified IDF-MetS independent of smoking and F-IRI concentrations in Japanese men, but not in women.
Author Contributions
Conceived and designed the experiments: TN. Analyzed the data: JO, TN, YY. Wrote the first draft of the manuscript: YY, JO. Contributed to the writing of the manuscript: YY, JO, TN. Agree with manuscript results and conclusions: YY, JO, TN, YU. Jointly developed the structure and arguments for the paper: YY, JO, TN, YU. Made critical revisions and approved final version: YY, JO, TN, YU. All authors reviewed and approved of the final manuscript.
Disclosures and Ethics
As a requirement of publication the authors have provided signed confirmation of their compliance with ethical and legal obligations including but not limited to compliance with ICMJE authorship and competing interests guidelines, that the article is neither under consideration for publication nor published elsewhere, of their compliance with legal and ethical guidelines concerning human and animal research participants (if applicable), and that permission has been obtained for reproduction of any copyrighted material. This article was subject to blind, independent, expert peer review. The reviewers reported no competing interests.
Footnotes
Acknowledgements
We thank Dr Naoyuki Kamatani, MD, PhD, a specialist in medical statistics at StaGen Co. Ltd., for his advice concerning the statistical analyses used in the present manuscript.