
Abstract
Low protein diet (LPD) plays an important role in preventing the progression of diabetic nephropathy. However, it is a great burden to the patients. In this paper, we have studied the quality of life (QOL) in such patients.
The study subjects were 59 patients (male 38, female 21) with type 2 diabetes. The patients were classified into tertiles based on their protein intake (g/kg BW). Scores from the diet-related QOL questionnaire were summarized by principal component analysis into four components; mental health, less burden, satisfaction and merit, and less social restriction.
Higher protein intake was associated with less burden and less social restriction. In multiple regression analysis, the significant predictors for the “less burden” component were higher protein intake/BW and estimated glomerular filtration rate (eGFR).
In summary, registered dietitians and clinicians must keep in mind that LPD is a serious burden to the patients and efforts must be made to minimize their burden in order to avoid discontinuation.
Introduction
Diabetes mellitus is associated with many chronic complications, most of which are vascular ones. They are further subdivided into macro- and micro-vascular complications. The former includes ischemic heart disease, cerebrovascular accident, and gangrene. Retinopathy, nephropathy, and neuropathy are the examples of the latter. The treatment goal for diabetes is the prevention of such complications through adequate treatment.
Of these complications, diabetic nephropathy is of great clinical and societal importance, since it is by far the most common underlying disease to necessitate hemodialysis due to chronic renal failure (CRF) in Japan. 1 Additionally, the intimate association between renal dysfunction and cardiovascular diseases is increasingly recognized.2,3 Thus it is essential to prevent or slow the progression of diabetic nephropathy, for which nutritional therapy plays an important role.4,5
In the dietary therapy for diabetic nephropathy, protein restriction is of pivotal importance,4,5 for which, however, some controversy exist.6–8 As will be detailed in the Discussion section, low protein diet (LPD) is likely to be effective in patients with good compliance for dietary therapy.9,10 Compared to drug treatment, dietary therapy is characterized by patients being required to be much more actively involved in the treatment. This would especially hold true in the LPD, which is a great burden for the patients. This burden can greatly impair their quality of life (QOL) and lead to the discontinuation of the therapy. To prevent discontinuation and to encourage the patients, registered dietitians (RD) and physicians must acknowledge the problems associated with the dietary therapy from the patients’ perspectives. In this paper, we have studied the burden associated with the dietary therapy in diabetic patients with or without protein restriction.
Subjects and Methods
Subjects
The study subjects were 59 patients (male 38, female 21) with type 2 diabetes with or without protein restriction, who visited our department for dietary consultation. Subjects who had at least three consecutive dietary advices were included in the study. The study protocol was approved by the ethical committee of Kyoto Women's University, and written consent was obtained from the subjects.
Anthropometric and laboratory data
Height and weight were measured and body mass index (BMI) was calculated. General blood tests such as liver function, kidney function, lipid profiles, electrolyte, plasma glucose, and HbA1c were done. The estimated glomerular filtration rate (eGFR) was calculated according to the officially suggested equation. 11
In the current study, the patients’ renal function was classified based on eGFR, since data on the albumin excretion rate (ACR) was not necessarily obtained in all the subjects. 12 The subjects were subdivided into two groups; (1) those with eGFR less than 60 mL/minute/1.73 m2 and (2) those with eGFR equal to or higher than it, based on the definition that chronic kidney disease (CKD) refers to, a state with an abnormal finding indicating renal damage such as proteinuria or eGFR less than 60 minute/mL/1.73 m2. 11
Food intake
The RDs (KS, HT, KW) have evaluated the energy and nutrients intake based on the patient records, which were fortified by interviews with the patients.
QOL questionnaire
QOL evaluation was done by self report using a QOL questionnaire regarding the diet developed by Sato et al. 13 The following subscales were obtained according to the published reference; satisfaction with diet, less physical burden of diet therapy, less mental burden of diet therapy, perceived merits of diet therapy, general perception of diet, less restriction of social functions, mental health, and vitality. We have added the word “less” for clarity, since each score is expressed as a higher score representing a better QOL status.
Statistical Analysis
Data were analyzed with SPSS 20.0 for Windows. Comparison was done with Student's t-test for the two independent groups, and analysis of variance (ANOVA) for the three independent groups. Principal component analysis was performed to summarize the data. Multiple regression analysis was done to evaluate the relative importance of the determinants for the four components obtained as above. Data were considered statistically significant at P < 0.05.
Results
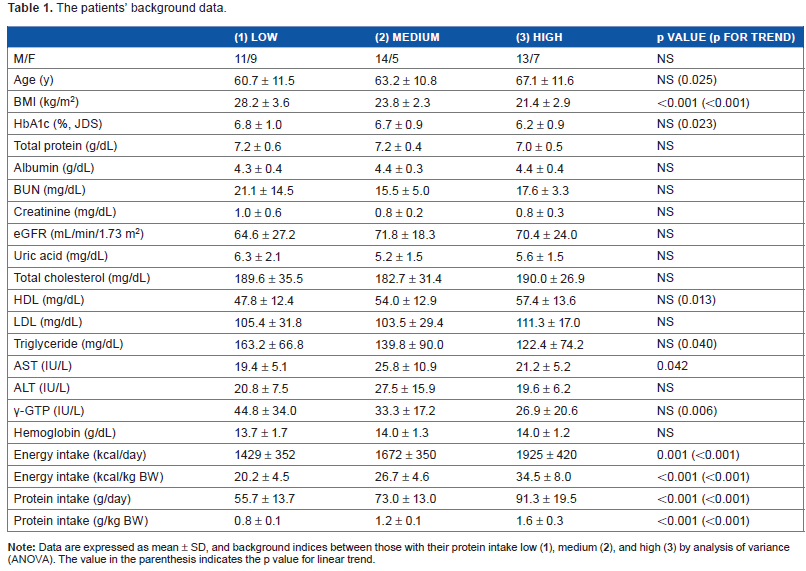
The subjects were classified into three groups by the tertiles of their protein intake (g/BW). Table 1 shows the patients’ background data in these three groups. Patients with higher protein intake/BW had lower BMI, lower blood levels of HbA1c, γ-GTP, and triglyceride, higher age, and higher serum HDL level. Higher protein intake (g/BW) was associated with higher energy intake (kcal/BW). With regard to the adherence, the percentage of subjects whose actual protein intake did not exceed the amount advised by the RD was 38% as a whole, and 80, 28, and 15% in those in the low, medium, and high tertile, respectively (data not shown).
The patients’ background data.
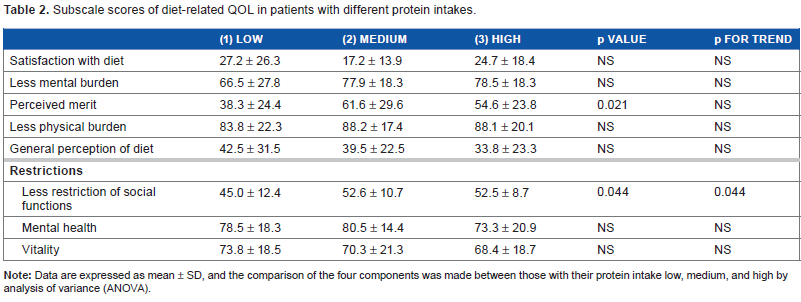
The subscale QOL scores were compared in these three groups. As shown in Table 2, there were no statistically significant differences in these groups except that higher protein intake was associated with less restriction of social functions. Perceived merit was significantly different among the three groups.
Subscale scores of diet-related QOL in patients with different protein intakes.
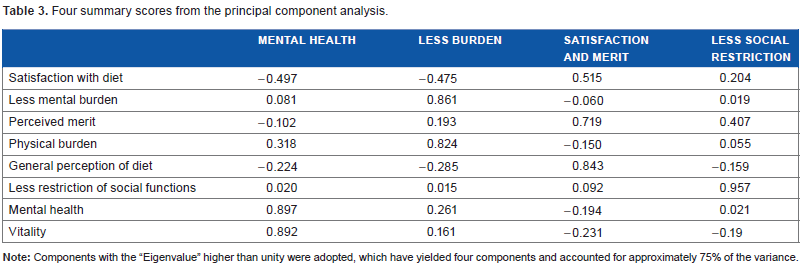
Then, principal component analysis was performed for these subscales (Table 3). Four components with the “Eigenvalue” higher than unity were adopted, which accounted for approximately 75% of the variance. The first component, with its association with mental health and vitality, was named “mental health”. The second component was associated with less mental and physical burden, and named “less burden”. The third component was named “satisfaction and merit” based on its association with satisfaction with diet, perceived merits of diet therapy, and general perception of diet. The fourth component was associated with less restriction of social functions, and named “less social restriction”. As in the case of the subscales, in these summary scores also, a higher value indicates a better QOL status.
Four summary scores from the principal component analysis.
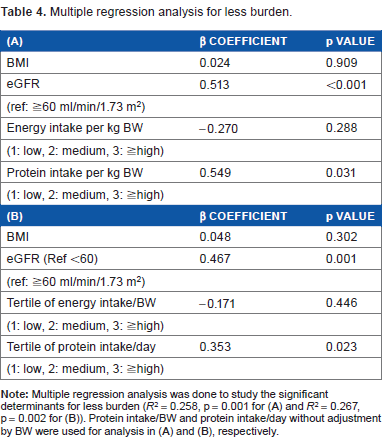
Multiple regression analysis was done to evaluate the relative importance of determinants for the four components. Independent variables employed included BMI, eGFR, protein intake per BW, and energy intake per BW (Table 4A). Significant contributors for less burden, listed in descending order were protein per BW and eGFR (adjusted R 2 = 0.258, P = 0.001). Multicollinearity was not observed. Significant contributors were not identified for the other three components. Another multiple regression analysis using the protein intake/day instead of protein intake per BW has yielded similar results (Table 4B).
Multiple regression analysis for less burden.
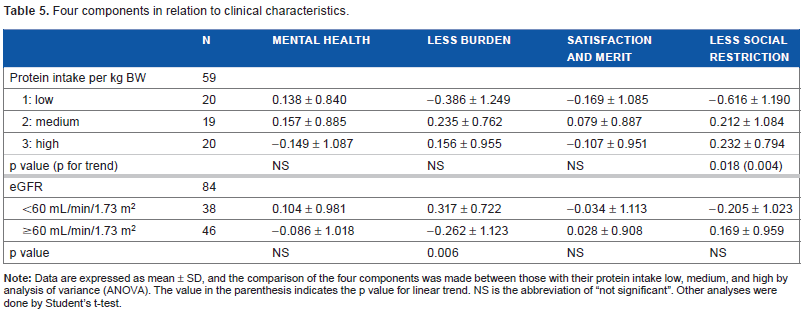
These four components were compared with relation to significant predictors described above (Table 5). First, they were compared among the three groups depending on the patients’ protein intake (g/kg BW). Higher protein intake was significantly associated with less social restriction and less burden, the latter not reaching statistical significance. Comparison of the four components was made between those with eGFR less than 60 mL/minute/1.73 m2 and those with eGFR equal to or higher than that. Paradoxically, less burden was associated more with those with eGFR equal to or higher than 60 mL/minute/1.73 m2 than those with eGFR less than 60 mL/minute/1.73 m2. The other three components were not significantly different between the two groups.
Four components in relation to clinical characteristics.
Discussion
In the current study, the patients were first divided into tertiles based on their protein intake. The extremely restricted protein intake advocated by some authors such as 0.5–0.6 g/g BW was not employed in our hospital.14,15 Patients belonging to the lowest tertile of protein intake had significantly lower energy intake/BW. Although there is no clear explanation for it at present, one of the possibilities would be as follows. Patients with advanced stage of diabetic nephropathy and under protein intake restriction are advised to take enough energy. However, when they are advised to reduce their protein intake, they seem to reduce the energy intake concomitantly. Diabetic patients have long been under energy control, and they do not seem to be able to easily accept the new concept of dietary therapy to assure adequate intake of energy.
No significant differences in subscale scores of diet-related QOL were observed among these groups except for less restriction of social functions and perceived merit. The data were analyzed after principal component analysis yielding four components; mental health, less burden, satisfaction and merit, and less social restriction. Higher protein intake was significantly associated with less social restriction and less burden, the latter not reaching statistical significance. From these results, dietary protein restriction is likely to be a burden for the patients and poses social restriction. Multiple regression analysis has shown that the significant contributors for the less burden were protein intake per BW, and eGFR. These results suggest that protein restriction is a significant determinant of the patients’ QOL especially with relation to the burden to the patients. Restricted protein intake is more likely to affect the patients’ QOL than the restricted energy intake, for which, however, further studies are indicated.
There has been some controversy regarding the daily protein intake adequate for the patients with diabetic nephropathy. Some reports support the positive effects of LPD in preventing the progression of diabetic nephropathy, 6 while papers arguing against such effects have also been published, including meta-analyses. 7 8 Another recently published meta-analysis has shown that LPD was associated with a protective effect on the decline in GFR only in patients with good compliance to diet therapy. 9 Kanazawa et al has shown that the decline in renal function test results such as GFR was significantly lower in patients with good compliance. 10 The previous meta-analyses are to be interpreted with caution, since some problematic papers are included in the analyses. For example, in two of the six papers included in a meta-analysis, 8 actual protein intake was as high as 1.10 g/kg BW despite the prescription of 0.8 g/kg BW, which is not different from that in the normal-protein diet group. Thus, the patients’ compliance is likely to be an important determinant of the effectiveness of the LPD.
Paradoxically, less burden was associated more with patients who had eGFR equal to or higher than 60 mL/minute/1.73 m2 than those with eGFR less than 60 ml/minute/1.73 m2. Although we do not have a clear explanation for this paradoxical result, it may be related to the methodological limitation of this study. First, the number of study subjects was modest. Additionally, although eGFR has recently been widely used as the simple measure to represent the renal function, it is not a specific index for diabetic nephropathy, and could be affected by extra-renal factors such as muscle volume. 11 Owing to the unavailability of ACR in the current study subjects, eGFR was used in this paper, which is a serious limitation of the current study.
Then the next issue to be studied would be the way to minimize the burden on the patients to avoid discontinuation. At present, we cannot answer the question based on robust data, but we believe that individualization plays an important role. Nutrition therapy recommendations recently launched by the American Diabetes Association state that individuals who have diabetes should receive individualized medical nutritional therapy (MNT) as needed to achieve treatment goals, preferably by an RD familiar with the components of diabetes MNT. 16 We are of the opinion that the RD should try to provide the patients with individualized advice by obtaining information such as their lifestyle or dietary preference in addition to their dietary intake. Such efforts would be of value in reducing the patients’ burden. Effective dietary advice to minimize the patients’ burden is to be studied.
In summary, we have shown that protein restriction is a serious burden to the patients. Dietitians and clinicians must keep this fact in mind and efforts must be made to minimize their burden to avoid discontinuation.
Author Contributions
Conceived and designed the experiments: KS, YT, AN, HT, KW. Analyzed the data: KS, AK, KT. Wrote the first draft of the manuscript: KS, KT. Contributed to the writing of the manuscript: KS, AK, KT. Agree with manuscript results and conclusions: KS, YT, AN, HT, KW, AK, KT, NI. Jointly developed the structure and arguments for the paper: KS, AK, KT. Made critical revisions and approved final version: NI. All authors reviewed and approved of the final manuscript.
Disclosures and Ethics
As a requirement of publication the authors have provided signed confirmation of their compliance with ethical and legal obligations including but not limited to compliance with ICMJE authorship and competing interests guidelines, that the article is neither under consideration for publication nor published elsewhere, of their compliance with legal and ethical guidelines concerning human and animal research participants (if applicable), and that permission has been obtained for reproduction of any copyrighted material. This article was subject to blind, independent, expert peer review. The reviewers reported no competing interests.