
Abstract
The reported success rate of uterine artery embolization (UAE) for obstetrical hemorrhage is more than 90%. We experienced a case of failed UAE for postpartum hemorrhage, although an embolic particle was found pathologically in the uterine vessels without coagulation. A 42-year-old woman (gravida 7, para 2) with placenta previa had genital bleeding at 35 weeks of gestation, and cesarean section was performed. We immediately added UAE aiming to reduce massive bleeding after the cesarean section, successful embolization of the bilateral uterine arteries and internal iliac arteries were confirmed by angiography regardless the vital sign was recovered with an appropriate amount of transfusion; the massive bleeding recurred after 1 hour of UAE. Hysterectomy was performed and pathological findings of the uterus showed that there was no coagulation in the vessels, which was supposed to be observed by the effect of gelatin sponge. In addition, despite the fact that no coagulation was found, only one gelatin sponge was found in 16 slices of the uterine wall specimens. We speculate that thrombotic materials were caught in vasoconstricted vessels triggered by hypovolemic shock due to acute blood loss, and then the gelatin sponge could be washed out after recovering to normalized circulation status leading to recurrent massive hemorrhage.
Case Report
A 42-year-old woman (gravida 7, para 2) visited our hospital at the 14th gestational week and was diagnosed as placenta previa in the posterior wall of the uterus by ultrasonography at 28 weeks of gestation. Her pregnant course was uneventful until she had massive bleeding amounting 700g with uterine contractions at 35 + 6 weeks of gestation. Cesarean section was performed under general anesthesia, and a healthy female infant weighing 2520 g was delivered with Apgar score of 8 in 1 minute and 9 in 5 minutes. The placenta was completely removed without any difficulty. Blood loss during the operation was 2730 mL and six units of red cell concentrates and ten units of fresh frozen plasma were administered.
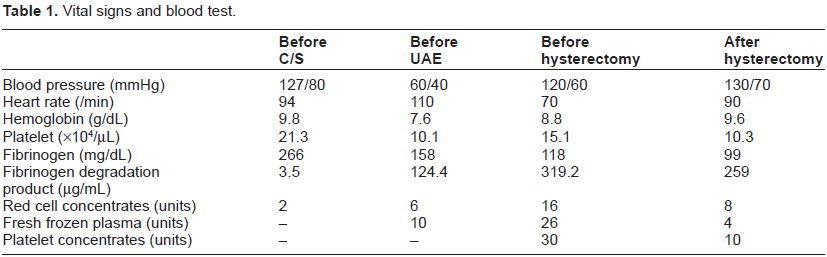
As continuous bleeding from the uterine cavity was recognized after the operation, and since atony of uterus might have accelerated external hemorrhage, we decided to perform uterine artery embolization (UAE). The vital signs, blood tests, and amount of transfusion at each occasion are shown in Table 1. After giving the appropriate amount of transfusion to maintain maternal circulatory status, UAE was safely completed, hemostat was confirmed by the angiography and also vaginal inspection (Fig. 1). Despite the normalized vital signs, bleeding was recognized after 1 hour of UAE, leading us to decide to perform hysterectomy. The patient recovered smoothly after the hysterectomy, and she left the hospital on the 17th day. Although we observed only one gelatin sponge particle in 16 slices of uncoagulated uterus, there was no thrombotic reaction around the particle (Fig. 2).
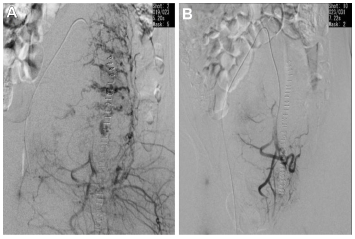
(A) Before embolization of the uterine artery. Contrast extravasation was seen. (B) Angiogram after embolization of bilateral uterine and internal iliac arteries showed complete occlusion.
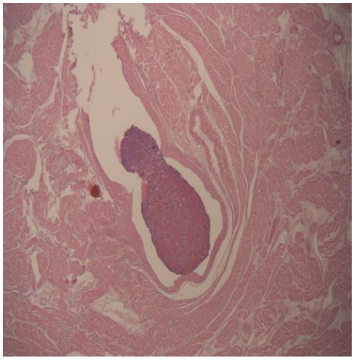
Pathological specimens obtained from the uterine myometrium.
Vital signs and blood test.
Discussion
This report has shown the pathological findings in a case of failed UAE for placenta previa complicating hypovolemic shock with disseminated intravascular coagulation (DIC). Success rates of UAE for postpartum bleeding have been reported to be over 90%.1–6 However, some reports have shown lower success rates of UAE in cases of abnormal placentation, uterine myometrial injury due to placenta accreta and delayed catheterization. 5
Despite the fact that we easily and completely separated the placenta and performed UAE immediately, continuous effect of hemostatic embolization was not observed. Hypovolemic shock caused by postpartum hemorrhage immediately induces vasoconstriction in peripheral vessels. 7 Moreover, one of the vascular characteristics observed during interventional radiology is arterial spasm caused by insertion of the catheter. 4 These circumstances might strongly affect the behavior of the uterine arteries and disturb the visualization of contrast extravasation by angiography, suggesting shortening of the arterial diameter. From this point of view, gelatin sponge might be easily caught in the uterine vasospastic vessels (Fig. 1). The presence of DIC would interfere with coagulant effects of gelatin sponge in this case. In addition, normalization of the vital signs owing to transiently effective transfusion would result in dilation of the arterial diameter, leading to washout of the gelatin sponge to the uterine cavity.
It is reported that particles would be found in almost all uterine tissue specimens of post-UAE cases. 8 Our speculation would be supported by the fact that almost no gelatin sponge was found in the removed uterine specimen. In severe coagulopathic condition where we should refrain from adding more stress such as hysterectomy, N-butyl cyanoacrylate (NBCA) may be one management strategy option, if the patient does not wish further pregnancy. NBCA acts as permanent embolic material and has immediate self-coagulant effects without interference of DIC.9,10
In conclusion, this case strongly supports the mechanisms that might interfere with the hemostatic process in the effect of gelatin sponge in cases complicated with vital shock and disseminated intravascular coagulation.
Author Contributions
Wrote the first draft of the manuscript: NW. Contributed to the writing of the manuscript: DT. Agree with manuscript results and conclusions: KN, HT, AN, TS, OI. Jointly developed the structure and arguments for the paper: NN. Made critical revisions and approved final version: MK. All authors reviewed and approved of the final manuscript.
Funding
Author(s) disclose no funding sources.
Competing Interests
Author(s) disclose no potential conflicts of interest.
Disclosures and Ethics
As a requirement of publication author(s) have provided to the publisher signed confirmation of compliance with legal and ethical obligations including but not limited to the following: authorship and contributorship, conflicts of interest, privacy and confidentiality. The authors have read and confirmed their agreement with the ICMJE authorship and conflict of interest criteria. The authors have also confirmed that this article is unique and not under consideration or published in any other publication, and that they have permission from rights holders to reproduce any copyrighted material. Any disclosures are made in this section. The external blind peer reviewers report no conflicts of interest.