
Abstract
The Great East Japan Earthquake inflicted immense damage over a wide area of eastern Japan with the consequent tsunami. Department of Traditional Asian Medicine, Tohoku University, started providing medical assistance to the disaster-stricken regions mainly employing traditional Asian therapies.
We visited seven evacuation centers in Miyagi and Fukushima Prefecture and provided acupuncture/massage therapy. While massage therapy was performed manually, filiform needles and press tack needles were used to administer acupuncture. In total, 553 people were treated (mean age, 54.0 years; 206 men, 347 women). Assessment by interview showed that the most common complaint was shoulder/back stiffness. The rate of therapy satisfaction was 92.3%. Many people answered that they experienced not only physical but also psychological relief.
At the time of the disaster, acupuncture/massage therapy, which has both mental and physical soothing effects, may be a therapeutic approach that can be effectively used in combination with Western medical practices.
Introduction
At 14:46 on March 11, 2011, a strong earthquake of magnitude 9.0 struck off the Pacific coast of Tohoku, and the resulting massive tsunami inflicted immense damage on eastern Japan. After the Great East Japan Earthquake, Tohoku University Hospital, located in a disaster-stricken region, immediately started emergency rescue operations and concurrently received patients from other hospitals in the region. Furthermore, medical teams were sent to the disaster-stricken regions to conduct relief operations at disaster base hospitals and evacuation centers. As part of the disaster relief operations of Tohoku University Hospital, the Department of Traditional Asian Medicine at Tohoku University also conducted medical operations immediately after the earthquake disaster, mainly employing traditional Asian medical practices, in Onagawa Town and Ishinomaki City in Miyagi Prefecture and Aizu-Bange Town in Fukushima Prefecture. Because there was a rise in people suffering from chronic pain and neck/shoulder stiffness approximately 1 month after the earthquake, we provided acupuncture/massage therapy along with traditional Asian medical treatments at the request of physicians. We herein report the details of our disaster relief operations with acupuncture/massage therapy.
Methods
During the first three months after the Great East Japan Earthquake, we participated in the disaster medical operations of the Department of Traditional Asian Medicine at Tohoku University and provided a total of 17 sessions of voluntary acupuncture/massage therapy at seven evacuation centers in Miyagi and Fukushima Prefectures. The scenes of the therapy sessions are shown in Figures 1 and 2. We used the data from medical records on the therapy performed at five evacuation centers set up in elementary and junior high schools in Ishinomaki City. The data extraction period was two months from April through May (total of five operations). While massage therapy was performed manually, acupuncture therapy was performed mainly with filiform needles (diameter of 0.16 mm and length of 30 mm; Seirin Corporation, Shizuoka, Japan) and press tack needles (PYONEX®, diameter of 0.2 mm and length of 0.6 mm; Seirin Corporation, Shizuoka, Japan). We did not conduct research, such as asking people to fill out questionnaires, in order to avoid burdening the evacuees. Only the data from the medical records are presented in this report. We examined patient background factors, chief complaints at the time of therapy. Because medical records have many lack of data of symptoms and affected sites in the situation of disaster, we used medical records of 128 patients that include enough data. The data corrected from medical records were so varied, therefore we could not perform statistical analysis.

Scene of massage therapy in the treatment room.

Scene of massage therapy in the living quarters of an evacuation center.
Results
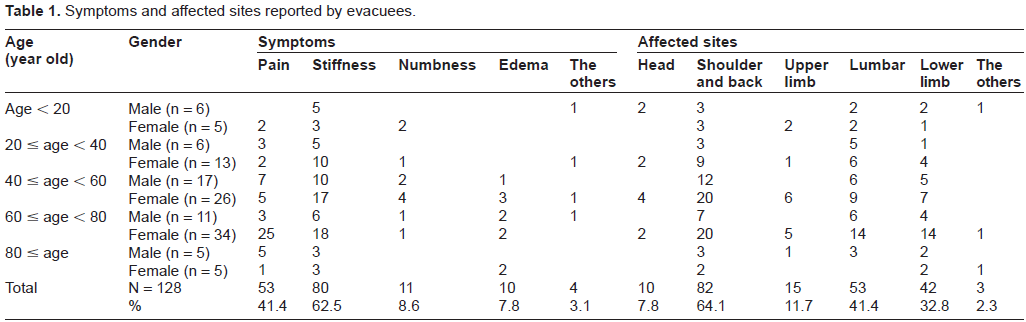
In total, 553 people (206 men and 347 women) were treated. The mean age was 54.0 years. A dedicated treatment room was set up only in one evacuation center. At the other four centers, evacuees were treated in their living quarters. Table 1 shows the information about age, gender, symptoms, and affected sites of 128 patients who received acupuncture/massage therapy. The common complaints were pain (total 41.4%) and stiffness (total 62.5%), and common sites were the shoulder and back (total 64.1%) and lumber (total 41.4%) (Table 1).
Symptoms and affected sites reported by evacuees.
Discussion
After the Great East Japan Earthquake, the Department of Traditional Asian Medicine at Tohoku University conducted medical operations, mainly providing traditional Asian treatments, in the extensively damaged coastal regions of Miyagi and Fukushima Prefecture. Because Western medical treatment was also limited at the evacuation centers, there were some evacuees with prolonged symptoms of the common cold, gastroenteritis, allergic reactions, insomnia, etc. Through these medical operations, we realised that traditional Asian treatments can alleviate various symptoms when given in combination with Western medical practices even under such difficult circumstances as those encountered after the disaster. 1 Moreover, the characteristic symptoms were stiffness and pain that started to increase approximately 1 month after the earthquake. It is said that chronic pain often occurs based on not only systemic changes but also with a psychological background. 2 In the early period after the Great East Japan Earthquake, at least 50,000 people were evacuated in Miyagi Prefecture alone. 3 We speculate that those complaining of pain affecting various parts of the body increased due to the unaccustomed stay at an evacuation center, as well as lying down in a space too small to roll over, contents of meals, environmental problems, psychological shock, stress, etc. In addition to relief of pain and stiffness, acupuncture/massage therapy can contribute to early detection of other problems that evacuees might be prone to develop because long therapy sessions allow practitioners to listen attentively to evacuees. The therapy satisfaction rate of 92.3% may reflect not only simple effects of physical treatment but also relaxing effects derived from the inherent sense of trust and safety generated by the warmth of manual treatment and conversation during the therapy sessions.
In early April, when voluntary acupuncture/ massage therapy was started, running water had not yet been restored at any evacuation center. Under the sanitary conditions at the time, evacuees could not bathe or even wash their hands properly. During this period, we performed only massage therapy in consideration of infection risks and gave consideration to performing acupuncture therapy after the evacuees were again able to bathe. Under such conditions of inadequate sanitation, the use of contact needles that noninvasively stimulate the skin may be an option. Moreover, the circumstances for setting up a treatment room varied among the evacuation centers. A dedicated treatment room was set up in only one center. When acupuncture/massage therapy is performed, a dedicated treatment room may be necessary to protect the safety and privacy of evacuees. We also consider it to be necessary, if no treatment room is available, that a dedicated space be set up with tents, drapes, etc., because acupuncture/massage therapy often requires exposure of the skin. Acquiring a dedicated space has the merit of facilitating hygiene and risk management in addition to protecting privacy. In conversation with treated evacuees, some told us that being able to lie down alone, even if only during a therapy session, was valuable because there is no solitude while staying at an evacuation center. We also considered it to be necessary to provide time and space to relax for those experiencing the stress of living in an evacuation center.
Interestingly, history-taking before treatment revealed many evacuees to be taking oral antiplatelet or anticoagulant drugs. The incidences of haemorrhage and haematoma formation due to acupuncture therapy are low but these complications have been reported. 4 In order to predict the occurrence of these adverse events, it is essential to determine medication usage, blood pressure, pulse, etc., beforehand by sufficiently interviewing evacuees. While questioning patients about the history of infection as thoroughly as possible, practitioners should ensure the use of gloves, proper management of disposable needles, etc., for infection control. Furthermore, possible responses of the body to acupuncture/massage therapy, such as lassitude, internal haemorrhage and discomfort, should be sufficiently explained before treatment. Especially in volunteer operations that are likely to provide one-time treatment, consideration must be given to reducing the amount of stimulation because evacuees cannot be followed up. Ideally, practitioners should repeatedly visit the same evacuation centers and monitor treatment progress.
The medical teams of Tohoku University Hospital accompanied us in our operations, and physicians performed history-taking whenever possible. Acupuncture/massage therapy at the time of the disaster was widely requested by medical professionals. There were also rescue medical teams that performed physiotherapy or musculoskeletal manipulation of their own accord. In the medical operations of the Primary Care for All Team of Japan Primary Care Association, 5 the Association of Medical Doctors of Asia, 6 the Disaster Victim Assistance Project Team, 7 etc., practitioners of acupuncture and massage accompanied the medical teams and performed therapy at their request. In operations conducted at the time of disaster, collecting various forms of information and making decisions are often left to individual practitioners. However, conducting medical operations with medical staff assures the adequacy of history-taking, questioning patients about medication usage, and risk management. Thus, acupuncture/massage therapy can be provided effectively.
At present, there are nearly 90,000 nationally certified acupuncturists, moxacauterists, and masseuses in Japan. 8 It is expected that many would want to participate in volunteer disaster-relief operations. However, these practitioners may have to abandon this desire because no route for participating in such operations has yet been established. Thus, we hope that organisations, such as academic societies, will develop strategies and programmes for recruiting volunteers, possibly via websites and so on, before the next great need arises.
Conclusion
Requests for acupuncture/massage therapy are increasing not only from evacuees but also from medical professionals. Acupuncture/massage therapy, which can be performed based on physical findings, may be among the effective medical treatments offered at the time of a major disaster. However, there is a possibility that the emotional status of the survivors were affected and comforted by the attention and treatment offered to them at this point in time.
Author Contributions
Conceived and designed the experiments: All authors. Analysed the data: TK, ST. Wrote the first draft of the manuscript: ST, TK. Contributed to the writing of the manuscript: MW, HK. Agree with manuscript results and conclusions: All authors. Jointly developed the structure and arguments for the paper: All authors. Made critical revisions and approved final version: All authors. All authors reviewed and approved of the final manuscript.
Disclosures and Ethics
As a requirement of publication author(s) have provided to the publisher signed confirmation of compliance with legal and ethical obligations including but not limited to the following: authorship and contributorship, conflicts of interest, privacy and confidentiality and (where applicable) protection of human and animal research subjects. The authors have read and confirmed their agreement with the ICMJE authorship and conflict of interest criteria. The authors have also confirmed that this article is unique and not under consideration or published in any other publication, and that they have permission from rights holders to reproduce any copyrighted material. Any disclosures are made in this section. The external blind peer reviewers report no conflicts of interest.
Footnotes
Acknowledgment
We sincerely appreciate all those who participated in our volunteer operations and who offered generous assistance from all over Japan and the rest of the world. Moreover, the needles that we used were provided for disaster medical operations by Seirin Corporation. We appreciate its cooperation despite the difficulties encountered in the distribution of materials.
At last, we express our heartfelt condolences to the victims of the Great East Japan Earthquake and sincerely pray for the earliest possible recovery and reconstruction.