
Abstract
Traditional herbal (Kampo) medicines have been used since ancient times to treat patients with mental disorders. In the present report, we describe four patients with dysthymia successfully treated with Kampo medicines: Kamiuntanto (KUT). These four patients fulfilled the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) criteria for dysthymic disorder with easy fatigability and sleeplessness, but did not fulfill the criteria for major depressive disorder. Treatment with KUT relieved depressive status, fatigue and sleeplessness in these patients. As a result, their QOL (quality of life) was considerably improved. KUT may be useful as an additional or alternative treatment for dysthymia, especially in the field of primary health care.
Introduction
Dysthymic disorder (dysthymia) is a disabling psychiatric disorder characterized by mild but persistent depressive symptoms. In the USA, it is reported that the lifetime prevalence of dysthymia ranges from 3% to 6% in the general population,1,2 and up to 36% in psychiatric outpatient clinics. 3 In Japan, a low lifetime prevalence (1.4%) 4 and a 12-month prevalence of 0.7% 5 for dysthymia have been reported. It has been suggested that the low rate of dysthymia in Japan is due to a lack of familiarity with operational diagnostic criteria, such as the Diagnostic and Statistical Manual of Mental Disorders (DSM). Early diagnosis is of vital important for the successful treatment of dysthymia, especially in primary health care. Additionally, about 25% of patients with dysthymia experience a chronic unchangeable status, and a subset of these patients develop major depressive disorder despite various treatments, such as antidepressants and antianxiety drugs.
In Japan, traditional herbal (Kampo) medicines (THM) are covered by national health insurance and play an important role in primary care, and several kampo formulae have been prescribed for mental disorders.6,7 THM has two points that differ from Western Medicine, i) the Kampo formula is a crude drug, not a purified chemical product; ii) the diagnostic system in Kampo Medicine differs from that of Western medicine. A Kampo formula is generally composed of several herbal components and is generally considered safe. Pseudoaldosteronism due to licorice root is a well known adverse effect of THM. There have also been allergic effects, such as skin eruption and liver injury, induced by crude drugs. Furthermore, it is crucial to understand that the Kampo diagnostic system is constructed from a paradigm that differs from the paradigm underlying Western natural science. When we treat a patient with dysthymia using Kampo Medicine, Kampo diagnosis is required in addition to that of Western Medicine. These characteristics make it difficult to perform controlled clinical trials. Therefore, there is no evidence supporting the use of Kampo formulae for dysthymia although Kampo formulae are often applied for mental disorders in Japan. However, it is a fact that there are responders to THM among patients with dysthimia. In this regard, we prescribed Kamiuntanto (KUT), one of these Kampo formulae, for the treatment of dysthymia with several physical and mental symptoms diagnosed by DSM-4th edition (DSM-IV).
Here, we describe four patients with dysthymia who were successfully treated with KUT.
Case Reports
Treatment of each patient was approved under the comprehensive agreement of Gunma University. Informed consent was obtained from all four cases before treatment with Kampo therapy. Further, each patient was treated before 2008. The authors have received training in performing clinical trials at Gunma University.
Case 1
A 63-year-old male consulted the Department of Japanese Oriental (Kampo) Medicine (DJOM), Gunma University in October 200X requesting traditional herbal medicine (Kampo) for dysthymic disorder with sleeplessness and malaise that had persisted for about 5 years despite treatment with antidepressants (Table 1). He worked at a bakery as a full-regular employee on ordinary days. He was neither a smoker nor a drinker. At the initial examination, there were no remarkable findings in the chest or abdomen, and hepato-renal and thyroid functions appeared normal on both blood analysis and image diagnosis. Additionally, he had not complained of any clinical features indicating the dementia. He had been taking time off work several days a month due to fatigue. Treatment with Kamikihito, one of the kampo formulae, for 4 weeks failed to improve his symptoms. Kamiuntanto (KUT; Table 2) was therefore administered in addition to antidepressants. After KUT therapy for 12 weeks, sleeplessness and malaise improved. The patient was accordingly relieved from dysthymia and estazolam was discontinued, and the patient became able to commute every day. The improvement in social activity has continued for 3 years with KUT. In addition, we evaluated the improvement of depressive symptoms using global assessment of functioning (GAF) scale by DSM-4th ed. Text revision (DSM-IV TR) 8 in all cases. Her GAF scale changed from 70–61 to 90–81.
Clinical features of four patients with dysthymia.
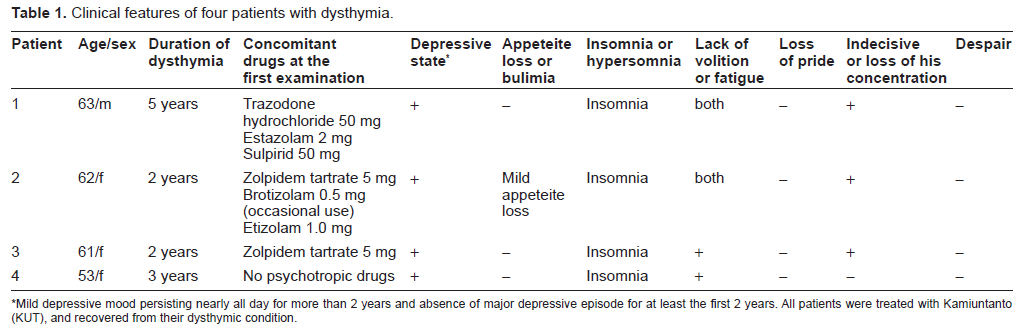
Mild depressive mood persisting nearly all day for more than 2 years and absence of major depressive episode for at least the first 2 years. All patients were treated with Kamiuntanto (KUT), and recovered from their dysthymic condition.
Herbal components of Kamiuntanto (KUT).
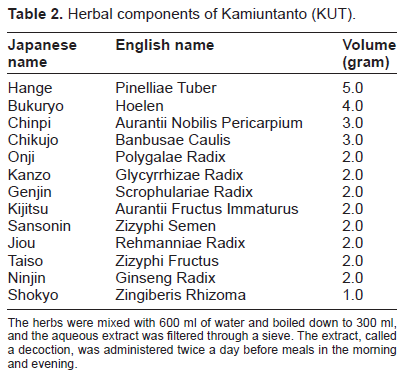
The herbs were mixed with 600 ml of water and boiled down to 300 ml, and the aqueous extract was filtered through a sieve. The extract, called a decoction, was administered twice a day before meals in the morning and evening.
Case 2
A 62-year-old female consulted DJOM requesting Kampo treatment for general malaise and lack of volition that had persisted for 2 years despite conventional Western therapy, which consisted of benzodiazepines. She was not regarded as having senile dementia. She was a housewife and barely able to perform housework. Her status was diagnosed as dysthymic disorder by operational diagnostic criteria; DSM-IV. Saikokeishikankyoto (decoction) therapy in addition to Western medicines for 4 months failed to improve her symptoms. Therefore, we changed the Kampo formula from Saikokeishikankyoto to KUT. Dysthymia, consisting of general malaise and depressive symptoms was reduced by 80% after KUT therapy for about 4 months, along with the occasional use of Kousosan (TJ-70, 2.5 g TSUMURA Co. Ltd Japan) to relieve her anxiety. Relief from dysthymia has continued for about 2 years with KUT treatment. Her GAF scale changed from 70–61 to 90–81.
Case 3
A 61-year-old female developed a feeling of heavy head and sleeplessness in April 200X. She was receiving atorvastatin for hyperlipidemia, and had also received a sleeping drug from a local hospital. However, her symptoms persisted, followed by the development of depressive symptoms and malaise, although she continued to work as a pharmacist. She consulted our hospital requesting Kampo treatment in November 200X + 2. She was diagnosed as having dysthymic disorder based on DSM-IV. Kousosanryo (decoction) therapy for 8 weeks failed to improve dysthymia. Her symptoms relieved by 80% after 4 months of KUT administration, and thereafter she became able to concentrate on work and housekeeping. Improvement of dysthymia has continued for 18 months with KUT treatment. Her GAF scale changed from 80–71 to 100–91.
Case 4
A 53-year-old female (menopause: 51-year-old) came to DJOM requesting Kampo treatment for dysthymic disorder with sleeplessness, malaise and nervousness without vasomotor symptoms, consisting of hot flashes and sweating, which had persisted for about 5 years. She was a housewife and barely performed housework. She had not been taking antidepressant therapy, although she was taking hypotensive drugs for essential hypertension. Depressive symptoms were relieved after 4 months of KUT treatment and the improvement continued for 6 months. However, sleeplessness, easy fatigability and appeteite loss reappeared. Therefore, we changed KUT to another kampo formula (Kamikihito: decoction) and have obtained improvement by 50%. Her GAF scale changed from 70–61 to 90–81.
In all cases, there were no remarkable findings in the chest or abdomen, hepato-renal and thyroid functions appeared normal on both blood analysis and image diagnosis, and dysthymic disorder had been diagnosed by a psychiatrist based on DSM-IV criteria. During the follow-up periods, there were no adverse reaction attributable to Kampo medicines.
Discussion
Dysthymia is defined in DSM-IV as follows: mild depressive mood continued nearly all day for 2 years, and there were no major depressive episodes observed during at least the first 2 years. It has been reported that youth are susceptible to dysthymia, while elderly people demonstrate symptoms closer to major depressive disorder. Three (No. 1.2.3 in Table 1) of our cases were elderly patients, however kampo treatment with KUT resulted in an improvement of depressive mood. However, one of the patients (No. 4 in Table 1.) experienced dysthymic symptoms in the postmenopausal period, and her status was categorized as a climacteric mental disorder. It is well known that depressive symptoms in climacterium are associated with a decrease in estrogen (E2). Although an E2-like action of KUT has not been recognized, it is possible that KUT may also be effective for dysthymia in postmenopausal females.
Although dysthymia is apt to be regarded as a mild depressive disorder by non-psychiatrists, social loss due to dysthymia is serious. Cassano et al have reported that social activity shows greater reduction in patients with dysthymia than in patients with major depressive disorders. 9 The clinical features of dysthymia are characterized by low ADL despite mild depressive symptom. The etiology of low ADL remains unclear, but it is possible that it may be difficult to diagnose dysthymia early because the depressive symptoms are mild. In addition, the physical symptoms such as general malaise as well as emotional symptoms probably contribute to decreasing ADL in dysthymia. The clinical characteristics of each patient in this series are summarized in Table 1. Each patient complained of fatigue and sleeplessness. Furthermore, it is well known that dysthymia in climacterium is characterized by severe malaise. KUT treatment resulted in the improvement of depressive status, as well as easy fatigability and sleeplessness, and so ADL would probably improve. These clinical courses suggest that KUT (Kampo medicine) may be useful as an additional or alternative treatment for dysthymia, especially in the field of primary health care. During this period, we encountered 2 other patients with depressive symptoms, who did not fulfill the criteria for dysthymia because the period of mild depressive symptoms was less than 2 years. Howevere, these patients were also successfully treated with KUT (data not shown). Kampo treatment generally aims not only at improving or regaining physical health, but also taking the patient's psychic and emotional imbalance into account. 10 However, the efficacy is limited among responders to KUT treatement. To confirm this efficacy, further clinical trial such as N of 1 clinical study, 11 will be required.
In Japan, traditional herbal medicines (Kampo) are covered by national health insurance, and are generally used in primary health care. KUT (kamiuntanto) is one of the kampo formulae used for the treatment of mental disorders, such as insomnia or dementia. 12 Kampo formula is administered following traditional diagnosis, in addition to diagnosis by Western medicine. The traditional target group for KUT comprises patients with sleeplessness, anxiety, and malaise after a serious illness as well as depressive status in patients lacking physical strength. 9 Since patients with dysthymia who complain of general malaise are close to the target group for KUT, we therefore treated 4 dysthymia patients with KUT and achieved good outcomes. Further, the traditional target group of Kamikihito (a kampo formula), which was administered in case nos. 1 and 4, comprises patients characterized by appetite loss in addition to other symptoms.
It is still not clear whether KUT improves the status of dysthymia, but several actions of KUT on the nervous system have been demonstrated. It has been reported that KUT potentiates the brain cholinergic system in an aged mouse model and its effect may be attributed to an increase in the activity of choline acetyltranseferase (ChAT). 13 Those effects have also been demonstrated in thiamine-deficient mice that demonstrate impairment of learning and memory. 14 It has been considered that the beneficial effect of KUT on Alzheimer's disease (AD) is due to the potentiation of ChAT, but not inhibition of cholinesterase (ChE). 12 Although an excess of HPA axis was observed in the patients with dysthymia, suppression of the HPA axis by KUT has not been demonstrated. However, recently it has been reported that AD and depression are significant associated in the aging population, and interestingly ChAT polymorphism is significantly associated with depression. 15 Three of our patients were elderly, and KUT might improve dysthymic status through action on ChAT as in dementia. Furthermore, Smith et al have demonstrated that cholinergic neurons were also decreased in the cerebral cortex such as the frontal lobe in postmenopausal females, and estrogen replacement therapy (ERT) suppressed the decrease in cholinergic neurons using SPECT and 123I-iodobenzovesamicol. 16 Therefore, it is possible that KUT treatment may potentiate ChAT in the postmenopausal female. We consider that the dysthymic patient (Pt. no. 4 in Table 1) in climacterium was also successfully treated with KUT due to its effects on ChAT. Thus, it is considered that KUT may be useful for various patients with dysthymia.
Finally, we present 4 patients with dysthymia successfully treated with the Kampo formula: KUT. KUT may be useful and safe as an additional or alternative treatment for dysthymia. These observations encourage us to proceed further with controlled trials to confirm the efficacy of KUT.
Disclosures
This manuscript has been read and approved by all authors. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The authors and peer reviewers of this paper report no conflicts of interest. The authors confirm that they have permission to reproduce any copyrighted material.
Grants
This work was supported by a Grant-in-Aid for Scientific Research from the Japan Society for the Promotion of Science.