
Abstract
Sickle cell disease (SCD) is the most common genetic disease in African-Americans, characterized by recurrent painful vaso-occlusive crises. Medical therapies for controlling or preventing crises are limited because of efficacy and/or toxicity. This is a randomized, controlled, single-crossover protocol of hypnosis for managing pain in SCD patients. Participants receive hypnosis from a trained hypnosis therapist followed by six weeks of self-hypnosis using digital media. Those in the control arm receive SCD education followed by a six-week waiting period before crossing over to the hypnosis arm of the study. Outcome measures include assessments of pain (frequency, intensity and quality), anxiety, coping strategies, sleep, depression, and health care utilization. To date, there are no published randomized, controlled trials evaluating the efficacy of hypnosis on SCD pain modulation in adults. Self-hypnosis for pain management may be helpful in modulating chronic pain, improving sleep quality, and decreasing use of narcotics in patients with SCD. TRIAL REGISTRATION: ClinicalTrials.gov: NCT00393250
Background
Sickle cell disease (SCD) is the most common genetic disease in African-Americans, characterized by recurrent painful vaso-occlusive crises. The disease is caused by a mutated form of hemoglobin that results in red blood cell (RBC) rigidity during low oxygen states. The most common types of SCD are sickle cell anemia (Hb SS), sickle cell hemoglobin SC (Hb SC), and sickle beta thalassemia (Hb Sβthal). When the defective hemoglobin gives up its oxygen, it is prone to polymerize, causing RBC rigidity and accelerated RBC lysis. These phenomena lead to recurrent vaso-occlusive “crises” that are usually accompanied by disabling pain. The pain episodes are commonly termed “crises” as they are unpredictable, frequent, and debilitating. 1 The severity and frequency of the crises presents a significant impact on self-determination, independent living, and overall quality of life. 2 The symptomatology that drives the SCD patient to medical care falls into three major categories: anemia, pain, and infection. 3
The management of SCD in the past was predominantly palliative in nature, using symptomatic and preventative approaches. The standard of care for SCD patients during vaso-occlusive crisis is pharmacologic analgesia, typically with opioids. While this approach is effective for some patients, many are inadequately treated because of high dosage requirements that are difficult to meet over time, and this approach does little to prevent pain crises from occurring. Patients with SCD have a range of frequencies and intensities of painful vaso-occlusive episodes. Acute episodes often require the individual to be hospitalized for aggressive pain management. Characteristically, the management regime involves narcotic administration. Estimates of pain frequency, based on medical records in hospitals, emergency rooms, and sickle cell clinics, indicate that 10–20% of SCD patients have frequent pain, while 40–50% have some pain, and 30–40% have no pain.4,5 Yet, it remains unclear how many pain episodes associated with SCD may not involve hospitalization and are managed with a variety of opioid and non-opioid medications at home.6,7 Previous studies show that discharge follow-up was often deficient and ineffective with the patient going home without any pain medication at all. Pain coping strategies were rarely taught. 8
Impact of Chronic Pain in SCD
Pain in SCD is not limited to acute pain; SCD pain can also be classified as chronic pain or a mixture of both chronic and acute pain. 9 Chronic pain is not merely the continuation of the acute vaso-occlusive pain; it is often a result of vascular necrosis of bone particularly at the hips, shoulders, and ankles. SCD patients with more frequent or severe pain often have similar pain patterns throughout the lifespan. Pain has also been shown to be associated with sleep deprivation, poor school or work attendance, and decreased daytime functioning.7,10 Ideally, SCD patients with pain should learn to cope with the pain, with as little negative impact on daily function as a result of the pain or its treatment as possible. Evidence focuses on the frequency of pain resulting in emergency department use and number of hospitalizations because of pain crisis in SCD patients; however, few studies focus on these pain manifestations outside the typical health-care delivery system or how patients manage their pain apart from their physician. Furthermore, it is unclear what percentage of patients are able to self-manage their crises at home without accessing health-care professionals. 11
Smith and colleagues 11 have conducted The Pain in Sickle Cell Epidemiology Study (PiSCES), a longitudinal, etiologic study of pain with an emphasis on non-biologic variables. These investigators vividly describe the frustrations and barriers for both providers and patients related to pain assessment and relief in SCD. Chief among these barriers is that “red cell vaso-occlusion has no observable clinical correlates to validate subjective descriptions of painful crises, which results in physician skepticism and patient dissatisfaction.” 11 In addition to measuring psychosocial variables such as stress, mental health status, coping and social support, Smith and colleagues have developed a conceptual explanatory model of pain and utilization in SCD, which examines the relationship of individual demographics, disease-related variables, psychosocial variables, and readiness variables and their effects on distress disability, health care utilization, and pain. We used this conceptual model (Fig. 1) to guide us in the selection of measures evaluating the process and outcome variables of interest.
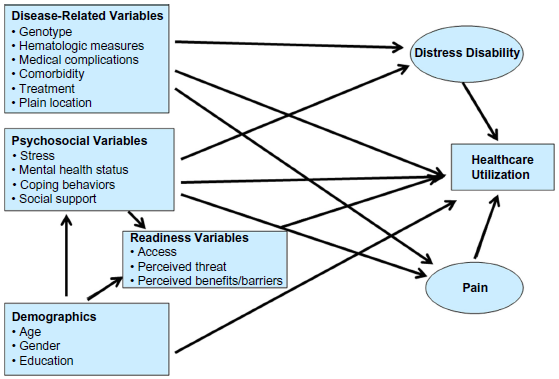
Explanatory model of pain and utilization in SCD. Conceptual explanatory model of pain and utilization over time in sickle cell disease. 11
Therapeutic Hypnosis as an Intervention
A published review summarized trials of psychosocial interventions as adjuncts to treating SCD. 12 These interventions included cognitive-behavioral techniques, hypnosis, and social support procedures wherein self-empowerment and education are strong facets of the supportive care approach. The effects of these techniques on pain control, quality of life, and health care utilization were inconsistent, perhaps because of inadequate study designs (eg, a lack of suitable control groups and non-standardized scripts).
Evidence exists supporting the efficacy of hypnotic analgesia in a variety of experimental13–15 and clinical settings, including pain associated with medical or surgical procedures.16–19 Gil and colleagues 20 demonstrated a direct correlation between daily use of pain-coping skills and less major health care contacts. Thus, cognitive measures that influence attitudes and improve pain-coping skills appear to have a significant impact on sleep, functional outcomes such as work and school attendance, use of analgesics, and major health care utilization. Since hypnosis is a cognitive-behavioral strategy that has been shown to have a powerful effect on pain management in a number of settings, it is postulated that a program designed to teach and encourage the use of self-hypnosis may positively impact the pain perception, sleep quality, functional outcomes, quality of life, and satisfaction of SCD patients.
As with other acute and chronic pain conditions, a goal in SCD pain management is to maximize function with the least amount of medication. Hypnotic training may offer an effective approach toward improving coping strategies and lessening focus on pain and its interference in functional outcomes. Hypnosis is a natural state of consciousness characterized by highly focused concentration with a relative suspension of global awareness. 21 In addition to addressing conscious processes, as in traditional cognitive-behavioral therapy, hypnosis can also access subconscious and unconscious processes. Hypnosis involves a change in the brain's perception. 22 A study by Rainville and colleagues (2002) using positron emission tomography (PET) provides supportive evidence that distinct brain changes occur during hypnosis particularly in the anterior cingulate cortex, the thalamus, and the pontomesencephalic brainstem during the production of hypnotic states. Furthermore, hypnotic relaxation is distinguished by a decrease in cortical arousal and disinhibition. 23
The efficacy of hypnosis has been demonstrated in treating numerous conditions including acute pain, chronic pain, burn injury progression, pulmonary diseases, and hemophilia, to name a few. 24 Hypnosis has also become part of a broader model of integrative mind–body interventions for breast cancer 25 and palliative care.26,27 Hypnotherapy, including self-hypnosis, has proven particularly effective in pain and symptom management for pediatric pulmonary patients28,29 and pediatric functional abdominal pain. 30 For those with clinically significant pain episodes, learning a cognitive-behavioral intervention centered on self-hypnosis for pain management has proved helpful in reducing pain frequency, improving sleep quality, and decreasing use of narcotic pain medications. 31 In a 12-month non-randomized prospective trial, Dinges et al. 31 demonstrated a reduction in both SCD pain days and non-SCD-related pain days. Analgesic use decreased proportionately in patients who experienced a decrease in pain frequency. The majority of this decrease resulted from a reduction in days with mild pain yet there was no significant reduction in the number of severe-pain days or length of vaso-occlusive episodes. This reduction of mild-pain frequency indicates that self-hypnosis may be most helpful for eliminating mild or moderate pain episodes of vaso-occlusive pain, and less helpful for the management of severe SCD pain episodes. Self-hypnosis training also decreased the frequency of poor-sleep nights, primarily by reducing the frequency of mild-pain nights. These improvements persisted over 12 months. 31 Additionally, two case studies have also been published supporting the use of hypnosis for pain management in SCD patients.32,33
Purpose of Study Protocol
To date, there are no published randomized, controlled trials evaluating the efficacy of hypnosis in SCD pain modulation in adults. Furthermore, there is a need to explore dosing of the hypnosis intervention with limited therapist time, and a model of home-based therapy has yet to be accomplished. This protocol is aimed at longitudinally assessing the effects of hypnosis in such a manner. The major advantage of conducting a longitudinal analysis is the ability to observe and separate changes over time within the study participants from differences among the participants in their baseline characteristics. Using repeated measures allows us to study the trajectory of psychosocial behaviors and pain intensity changes over time after controlling for intrapersonal correlations in order to draw valid scientific inferences regarding the impact of the hypnosis intervention.
Methods/Design
Recruitment
Patients with known or suspected SCD were recruited into this study through referrals by physicians from the National Heart Lung and Blood Institute (NHLBI) Vascular Therapeutic Section of the Cardiovascular Branch. Because Hb SC and S-β-plus-thalassemia patients typically have less pain than hemoglobin SS patients, for this pilot study we enrolled only hemoglobin SS patients.
Participants first underwent a screening history and physical examination to evaluate the presence and severity of SCD. Blood sample results from medical record source documents were utilized to establish hemoglobin genotype and baseline clinical characteristics. Participants had to meet all of the following criteria to be eligible for study enrollment:
Inclusion criteria:
≥ 18 years of age;
Diagnosis of hemoglobin SS SCD;
Patient identifies history of pain as a significant problem during at least 2 days in the month prior to enrollment; Written informed consent/assent has been obtained.
Exclusion criteria:
Less than 18 years of age;
Unwilling to experience hypnosis or to have hetero-hypnosis sessions recorded;
Non-fluency in written and spoken English;
Physical or other disabilities that prevent adequate participation in hypnotic susceptibility testing;
Does not wish to be video and audiotaped;
Psychosis or psychotic depression;
History of seizures or epilepsy.
There has been one published report of a serious consequence related to hypnosis, a seizure in an 18-year-old with a history of epilepsy. 34 For this reason, individuals with a history of seizures or epilepsy were excluded from this study. Reports also suggest that hypnosis in individuals with a history of psychosis or psychotic depression may trigger psychiatric illnesses or produce decompensation or recurrent dissociative episodes. 35 Based on these reports, this pilot study excluded individuals with a history of psychosis or psychotic depression. Although we do not expect that hypnosis will mask the onset of acute vaso-occlusive pain crisis, participants will be monitored and any unexpected adverse events reported to the clinical team as well as the institutional review board. The study complies with the principles of the Declaration of Helsinki and was approved by the institutional review board of NHLBI (NCT00393250).
Sample Size
A meta-analysis conducted by Montgomery et al. 36 of hypnotically induced analgesia exists estimating an average effect size of 0.74 across 18 studies. However, as previously noted, to date there have been no published randomized studies examining the efficacy of hypnosis-induced pain and symptom control in SCD patients. Because of this lack of evidence for accurately estimating an appropriate effect size for sample size selection, we proposed to conduct this study as a pilot with 20 participants in each group for a total of 40 participants. Based on the feasibility of undertaking this time- and resource-intensive intervention study and the possibility that some patients will be lost to follow-up, we requested an additional five participants in each group as our accrual ceiling.
Design
This is a randomized, controlled, single-crossover, repeated measures study (Fig. 2). After completing the intake interview, each participant was asked to begin daily pain diaries for one week. One week following enrollment, participants were randomized to the treatment or control groups. A random allocation scheme was computer-generated to provide participant group assignments. The study principal investigator (PI) and designees were initially blinded to the patient assignments, which were placed in individual, consecutively numbered, sealed envelopes. When the participant returned for their one week clinic visit, the study PI or designee opened the next numbered envelope to obtain that patient's assignment.
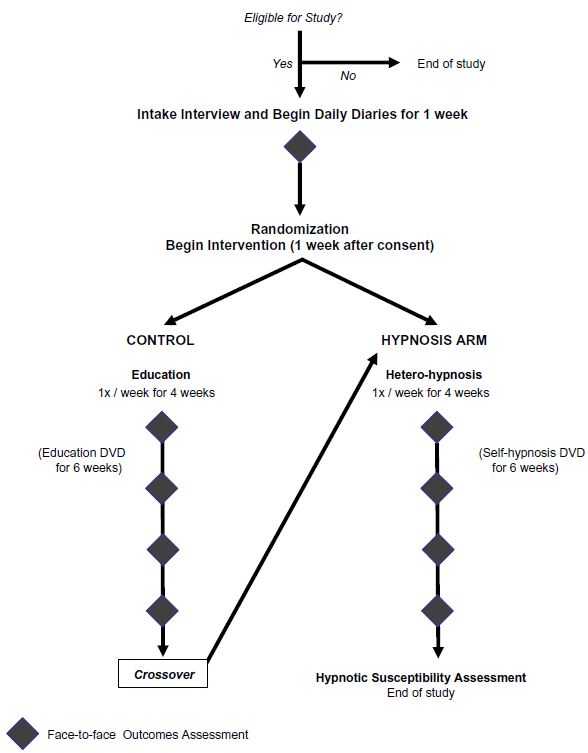
Hypnosis protocol design and randomization.
One week after enrollment, participants returned to the outpatient clinic and were randomized to the initial hypnosis (Group A) or control arm (Group B) of the study. Participants returned to the outpatient clinic as follows:
Interventions
Hypnosis interventions were conducted in four weekly sessions by an investigator certified in hypnosis (hetero-hypnosis). It is important to note that the sessions were conducted in a two-person-contact format in an outpatient clinic patient room rather than a group setting away from the clinic. Interventions consisted of a hypnotic induction followed by individualized suggestions for analgesia, reducing anxiety, improving sleep hygiene, promoting ego-strengthening (self-efficacy), and enhancing health and well-being (see Table 1 for sample scripts). When appropriate, participants also received therapeutic suggestions specific to other symptoms. Sessions lasted about one hour and were conducted typically in a clinic room. After completion of the self-hypnosis, an assessment was conducted to measure hypnotic ability, using the Stanford Hypnotic Susceptibility Clinical Scale for Adults. 37 Hypnosis sessions were videotaped and audiotaped for documentation purposes. Participants were excluded from the study if they did not wish to be video and audio taped because this was the method by which a standard, blinded hypnosis susceptibility score was obtained by an independent rater other than the hypnosis therapist. This hypnosis susceptibility rating was for documentation purposes and as a potential variable that may be associated with the outcomes of the treatment.
Self-hypnosis DVD categories and sample hypnotic excerpts.

Following these hetero-hypnosis sessions, participants entered a self-guided hetero-hypnosis phase. Participants were provided a digital video disc (DVD) for self-guided hetero-hypnosis and a DV D player. Each DVD had four selections from which participants can choose. Each selection had a scene from nature with the hypnotist's voice overlying the accompanying music from the scene. We hypothesized that scenes from nature that were recommended by SCD patients at an open house would provide additional interest and visual focus for the self-guided hetero-hypnosis. The participant only needed to watch one of these selections during a session. Participants were instructed to watch the DVD recording 3–7 times a week for six weeks. Participants were asked to evaluate their self-guided hetero-hypnosis experience in their daily diary (see Appendix C).
Therapeutic Use of Media
In addition to experiencing therapeutic hypnosis during face-to-face encounters in this study (hetero-hypnosis), participants also experienced self-guided hetero-hypnosis through digital media. The use of media technology for this study was twofold. The first reason was that videos allowed for a visual focus. While listening to the hypnotist, the patient was able to watch a scene from nature, thus complementing the audio and further removing them from their environment with the intent of making them more sensitive to suggestion. The other factor was closely tied to self-guidance. The patient had a choice of scenes to select from and therefore could match how they were feeling to what would assist them in visualizing relief.
Study processes for the control group were designed to control for the attention, interpersonal exchange, and positive expectation inherent in the therapeutic hypnosis experiences. Participants in the control group received age-appropriate education on SCD pathophysiology, inheritance, prevalence, common complications, and management in four weekly sessions. Education was delivered by a qualified nurse investigator. Sessions lasted about one hour and were typically conducted in a clinic room. Participants in the control arm received a DVD with educational material that they could use during the six weeks following the face-to-face education sessions. Following the 11th week, participants in the control arm crossed over to the hypnosis arm of the study and completed both the four weeks of hetero-hypnosis and the six weeks of self-hypnosis. All patients could receive standard medical therapy while on the study regardless of study group assignment.
Outcome Measures
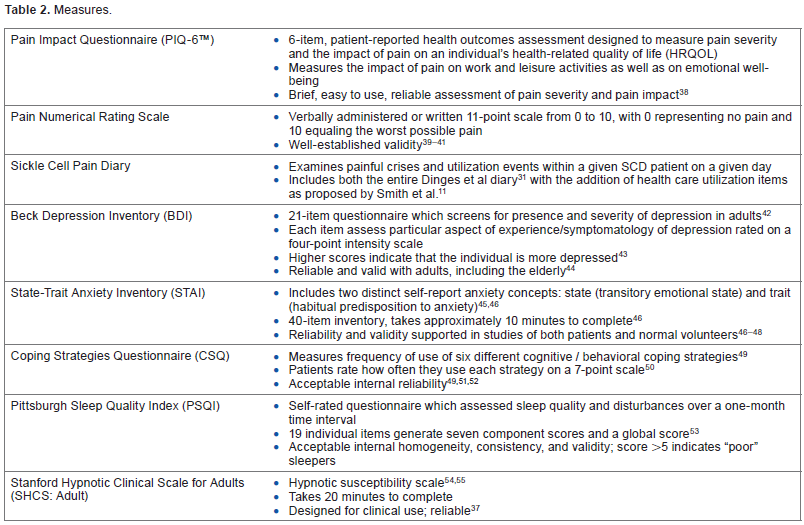
The primary outcome measures in this study were patients’ diary reports of pain severity and pain intensity as measured by the pain numerical rating scale during follow-up clinic assessments. Participants were instructed on daily documentation of pain incidence, pain severity, sleep quality, medications taken, visits to a hospital, emergency room, or physician's office, and absence from school or work. Secondary outcome measures (pain impact, mood, anxiety, sleep, and coping) were collected during face-to-face interviews prior to randomization, at the end of the four-week education or hypnosis interventions, and at two-week intervals until the end of the six-week self-hypnosis (intervention) or education (control) CD/DVD phases. See Table 2 for a list of validated outcome measures.38–55
Measures.
Analysis Plan
Initial analysis will be descriptive and exploratory Our hypotheses for the analysis phase of the protocol are as follows:
Therapeutic hypnosis, guided by a hypnotherapist (hetero-hypnosis) and followed with self-hypnosis using customized digital media, improves disease-related pain, anxiety, coping strategies, sleep, and depression compared to an education control intervention in patients with SCD.
Therapeutic hypnosis, guided by a hypnotherapist (hetero-hypnosis) and followed with self-hypnosis using customized digital media, reduces health care utilization compared to an education control intervention in patients with SCD.
Statistical analysis for each of the main outcomes will involve comparing the patients assigned to the hetero-and self-guided hetero-hypnosis intervention to patients who do not initially receive hypnosis using the appropriate scale/instrument for that outcome. Each scale/instrument will be analyzed separately and the general statistical approach will employ multiple-way analysis of covariance (ANCOVA) to compare the mean scores of the two groups. The analyses will control for specific patient factors (eg, genotype, hematologic measures, treatment, co-morbidity, age, gender, education) as indicated by the conceptual model. Mixed linear modeling will be used to account for some of the expected missing data in this repeated measures study.
Discussion
Previous research related to SCD patients has focused on the frequency of pain resulting in emergency department use and number of hospitalizations because of pain crisis in SCD patients. Few studies focus on these pain manifestations outside the typical health-care delivery system or on how patients manage their pain apart from their physician. Little is known about the percentage of patients who are able to self-manage their crises at home without accessing healthcare professionals.
Recent findings suggest that patients may have two types of positive outcomes following hypnosis treatment: 1) a reduction in the severity of ongoing daily pain intensity; and 2) the ability to use self-hypnosis to experience greater intervals of comfort. 56 However, to date, there are no published randomized, controlled trials evaluating the efficacy of hypnosis in SCD pain modulation. This protocol is aimed at longitudinally assessing the effects of hypnosis in such a manner. The design of this study provides information related to daily diary reports of pain incidence, pain severity, sleep quality, medications taken, as well as visits to a hospital, emergency room, or physician's office, and absence from school or work. Additional secondary outcome measures (pain impact, mood, anxiety, sleep, and coping) were collected during face-to-face interviews.
The major advantage of conducting a longitudinal analysis is its capacity to observe and delineate changes over time within the study participants from differences among the participants while controlling their baseline characteristics. Therefore, repeated measures and mixed linear modeling will allow us to study the trajectory of psychosocial behaviors and pain intensity changes over time after controlling for intrapersonal correlations in order to draw valid scientific inferences regarding the impact of the hypnosis intervention. Limitations exist in this protocol including the lack of qualitative inquiry to explore the patient experience while utilizing hypnosis as a self-care strategy for pain and symptom management. Although this is a randomized, controlled, crossover design, the sample size will not yield conclusive results in terms of treatment or dose efficacy, but rather will serve as a proof of concept for future randomized controlled trials (RCTs) testing hypnosis as a potential non-pharmacological approach to managing chronic pain and symptoms in adults with SCD.
Author Contributions
Conceived and designed the experiments: GW, DH, NA. Wrote the first draft of the manuscript: GW, KM, AB. Contributed to the writing of the manuscript: GW, KM, AB, DH. Agree with manuscript results and conclusions: GW, KM, NA, AB, DH. Jointly developed the structure and arguments for the paper: GW, KM. Made critical revisions and approved final version: GW, KM, NA, AB, DH. All authors reviewed and approved of the final manuscript.
Supplementary Files
Footnotes
Acknowledgments
We thank the NHLBI staff and research participants. We would like to especially acknowledge the following people for their support of this study: Ann Berger, MD; James Nichols, RN; Claiborne Miller-Davis, RN; Caterina Minniti, MD; Gregory J. Kato, MD; and Sinthujah Velummylum.