
Abstract
We assessed the applicability of the Glasgow Coma Scale (GCS) and the QT interval (QTc) to predicting outcomes in patients with organophosphate (OP) poisoning. In the hospital setting, QTc and GCS were monitored in each patient at admission. Patients with respiratory failure were compared to patients without these complications, and mortality was compared between groups. We found that the group with complications had a significantly longer QTc and a lower GCS score, a higher number of intubations, and worse outcomes (P < 0.05). GCS score and QTc have been shown to be equally good in predicting respiratory failure and hospital mortality in patients with OP poisoning. These results suggest that during initial out-of-hospital care of patients with OP poisoning, it is essential to monitor the QTc and the GCS score. The simplicity and promptness of these methods will allow providers to perform early and effective triage.
Introduction
Organophosphate (OP)-based pesticides are widely used and have emerged as the major contributor to ill health associated with pesticides worldwide.
Though accidental poisoning can occur following exposure with inhalation, serious poisoning often follows suicidal ingestion. Since respiratory failure is the most common cause of death in OP poisoning, early identification and effective management will help to reduce overall mortality in OP poisoning.1,2
The Glasgow coma scale (GCS) remains the most widely used scale to describe the level of consciousness of the victim and is reliable for assessment and prognosis of patients with nontraumatic coma.3–5 The GCS has been shown to be an effective clinical parameter that helps clinicians to predict the outcome of OP poisoning cases in the initial assessment.6,7
Poisoning with drugs influences biochemical elements of the brain and causes brain damage. This may change one's level of consciousness as well. The GCS has been performed to assess outcome and recovery of patients admitted to an intensive care unit (ICU) following drug overdose, 8 the mental status evaluation of poisoning patients, 9 the need for intubation in patients with antidepressant poisoning, 10 and to predict acute and delayed poisoning outcomes.11,12
The QT interval (QTc) is a measure of the time between the start of the Q wave and the end of the T wave in the heart's electrical cycle. A prolonged QTc is a biomarker for ventricular arrhythmia like torsade de pointes, and is a risk factor for sudden death. 13 A major retrospective study conducted in Taiwan by Chuang and colleagues 14 confirmed the relationship of QTc prolongation with the severity of OP poisoning in terms of respiratory failure and mortality. Shadnia and colleagues 15 also found that QTc prolongation may have prognostic value in OP compound poisoning.
The current study was performed with the aim of assessing the applicability of the GCS and QTc interval in predicting the outcome and complications of OP compound poisoning.
Methodology
This study was carried out from November 2009 to September 2011 in the ICU of the Government Medical College Nagpur in Maharashtra, India.
This is a prospective analytical study in which a total of 140 patients with organophosphate compound (OP) poisoning were included. Poisoning was confirmed by history, as well as classical features of OP in the form of hypersalivation, miosis fasciculations, characteristic odor of stomach wash and serum cholinesterase levels. It was also substantiated by examination of the container containing the compound, whenever this was brought in.
Patients who had history of alcohol consumption, chronic lung disease and cardiac disease were excluded.
In all patients, a detailed clinical examination was carried out to assess respiratory insufficiency, heurological status and cardiovascular system functioning. Special reference was given to the QTc and GCS score.
All patients underwent biochemical examination in the form of LFT, KFT, Blood glucose, ECG and X-ray. ECG was conducted while stabilizing the patient with a gastric lavage, atropine, oxygen and pralidoxime (PAM).
All patients were divided into two groups. Group A included those who developed respiratory failure, and group B included those who did not develop respiratory failure. Various parameters were also compared between patients who did and did not survive.
Statistical analyses
Continuous variables were presented in terms of the mean ± standard deviation. Categorical variables were expressed as percentages. Continuous variables were compared using unpaired t-tests for normalized data. The Wilcoxon rank-sum test was used for nonnormalized data. Categorical variables were compared using the Chi-square test. Linear trends were calculated to study the relationship between various factors and respiratory failure as well as mortality. The predictive performance of GCS and QTc was assessed using an ROC curve. To discriminate between respiratory failure and no respiratory failure, as well as mortality outcomes, the selected alpha criterion was 0.05. STATA statistical software was used for data analysis.
Results and Discussion
We evaluated a total of 140 patients with OP compound poisoning. They were grouped according to the presence of respiratory failure (RF) in Group A who developed RF and Group B who did not develop RF.
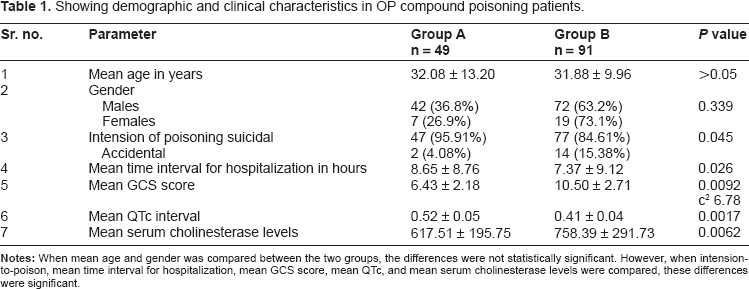
Our study included 140 patients with OP poisoning. These patients were divided into two groups. Group A included those with RF and Group B those who did not develop RF (Table 1).
Showing demographic and clinical characteristics in OP compound poisoning patients.
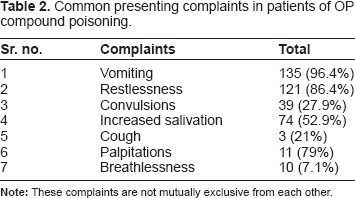
The symptoms of OP poisoning usually manifest within 30–90 minutes. Stimulation of the muscarinic parasympathetic system causes miosis, bradycardia, hypotension, bronchoconstriction, oversecretion of exocrine glands and hyperactivity of gastrointestinal smooth muscles.16,17 Its nicotinic effects manifest in the form of tachycardia, hypertension, mydriasis, fasciculations, muscle weakness and muscle paralysis (Table 2).18,19
Common presenting complaints in patients of OP compound poisoning.
RF occurs in two forms, early and delayed. Early RF occurs at or soon after admission, while the delayed form occurs several hours to 5 days after admission. 20 The mechanism of respiratory failure is likely to involve three components, including depression of central respiratory drive from the respiratory centre, respiratory muscle weakness and direct pulmonary effects such as bronchospasm and bronchorrhea. 20 A substantial number of deaths can be prevented with proper management of RF. Hence, it is important to identify the factors which help in prediction of RF in early stage, which will help in the early institution of ventilatory support. This will facilitate the selection of patients needing intensive management in the ICU. 21
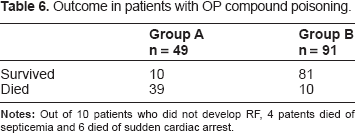
In our study, 49 (35%) of 140 patients developed RF and 91 (65%) did not develop RF. Out of 91 patients who did not develop respiratory failure 10 patients died, 4 due to septicemia and 6 due to sudden cardiac arrest (Table 6).
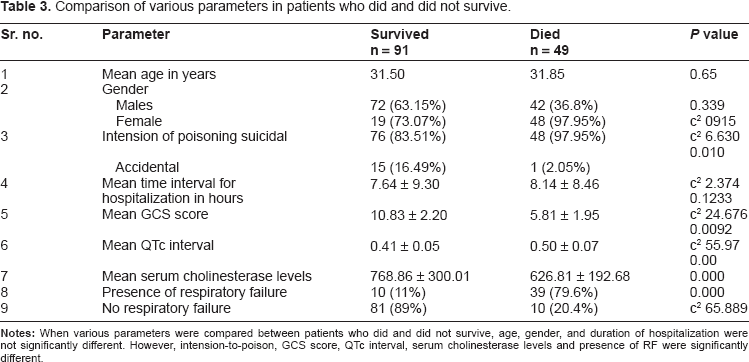
The consciousness level of each patient was judged according to GCS score at the time of admission. From the study it was found that a lower GCS score (3–6) on admission was associated with more incidences of RF (72.2%) and more mortality (Table 3).
Comparison of various parameters in patients who did and did not survive.
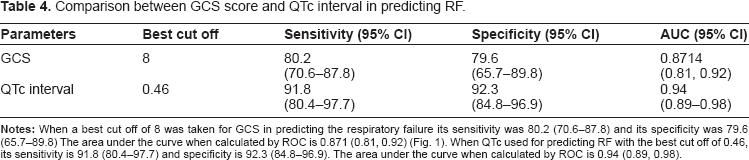
In our study sensitivity of QTc in predicting RF when 0.45 sec was used as best cut off was 91.8% and specificity was 92.3 % (Table 4, Fig. 1).
Comparison between GCS score and QTc interval in predicting RF.
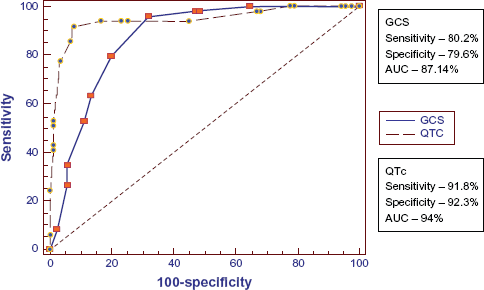
ROC of GCS and QTc for RF.
When best cut off of 8 was taken for GCS in predicting mortality its sensitivity is 87.8% and specificity is 84.6%. AUC when calculated by ROC is 0.94 (0.89, 0.97) (Table 5 and Fig. 2).
Comparison between GCS score and QTc interval in predicating mortality.

Outcome in patients with OP compound poisoning.
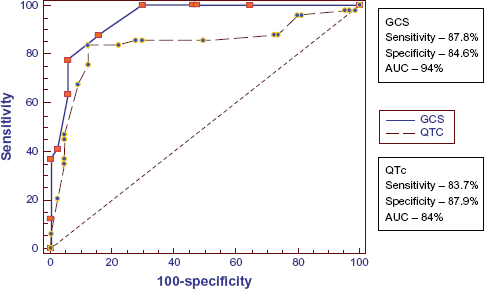
ROC of GCS and QTc for mortality.
Although rapid changes in the level of consciousness in poisoning cases may raise a question of the role of GCS on admission in predicting outcome, Ezadi Mood and colleagues 22 showed that the admission GCS score as well as its components can be validated for poisoned patients with mixed drug ingestion.
Grmec and colleagues 23 studied 65 patients of OP poisoning. Their results showed that the group with complications had significantly different values of measured parameters, including a longer QTc interval and lower GCS score, a higher number of intubations and a worse outcome. They have concluded that GCS score and QTc interval have been shown to be equally good in predicting RF as well as hospital mortality in patients with OP poisoning. 23
Okhan Akdur and colleagues 24 studied the effectiveness of poison severity score (PSS), GCS score and corrected QTc in predicting the outcome of acute OP poisoning. They found a significant correlation between GCS and PSS for grade 3 and grade 4 cases. They have stated that GCS is a parameter that helps clinicians to identify advanced-grade OP poisoning patients during initial assessment in the emergency department. However, ECG findings such as prolonged QTcs are not effective for determination of short-term prognosis, and show no relationship with the PSS.
Cander and colleagues 25 conducted a study including 25 patients with OP compound poisoning. They found that the mean GCS value was significantly lower compared to that of the group that survived.
Davies and colleagues 26 studied 1365 patients with a history of OP poisoning. They found that GCS, the International Program On Chemical Safety Poison (IPCS), and the PSS were similarly effective at predicting outcomes. Patients presenting with a GCS ≤ 13 need intensive monitoring and treatment.
Sungur and colleagues 27 studied 47 patients of OP poisoning. 10 (21.2%) patients required mechanical ventilation. The mortality rate for the patients who required mechanical ventilation was 50%. The mortality rate was 21.6% for the patients who were not mechanically ventilated. So they have concluded that since RF is the major reason for mortality, careful monitoring, appropriate management and early recognition of this components may decrease the mortality rate among these patients.
The mean serum cholinesterase levels in Group A and Group B in our study differ significantly (Tables 1 and 3). Rehiman and colleagues 28 also found a significant correlation of serum cholinesterase levels with the severity and ultimate prognosis in OP poisoning. Siu 29 showed that severity of OP poisoning can be predicted by serum cholinesterase levels. However, Nouira and colleagues 30 found that mean cholinesterase levels did not correlate with respiratory failure.
Our study shows that RF in patients with OP compound poisoning can be predicted by simple variables such as the presence of lower GCS on admission, and prolonged QTc on admission. These prognostic parameters can help doctors at peripheral health centers successfully predict outcomes. This way, high-risk cases can be referred to higher centers for expert management without wasting time, after necessary initial treatment such as doses of Atro-pine to assist with ventilation in patients with respiratory failure (Table 4).
In this way, the incidence of compilation and hence mortality due to OP compound poisoning can be reduced. For this reason it is necessary to train the doctors at the periphery, making them realize the importance of early treatment in OP poisoning and how to identify high-risk patients.
One limitation of our study is that the type of OP ingested could not be identified in all patients.
Footnotes
Author Contributions
Conceived and designed the experiment: AD, NG. Analysed the data: AD, NG. Wrote the first draft of manuscript: AD, NG. Contributed to the writing of manuscript: SD, AD. Agree with the manuscript, results and conclusions: AD, NG, SD. Jointly developed the structure and arguments for the paper: All authors. Made critical revisions and approved final version: All authors.
Funding
Author(s) disclose no funding sources
Competing Interests
Author(s) disclose no potential conflicts of interest.
Disclosures and Ethics
As a requirement of publication author(s) have provided to the publisher signed confirmation of compliance with legal and ethical obligations including but not limited to the following: authorship and contributorship, conflicts of interest, privacy and confidentiality and (where applicable) protection of human and animal research subjects. The authors have read and confirmed their agreement with the ICMJE authorship and conflict of interest criteria. The authors have also confirmed that this article is unique and not under consideration or published in any other publication, and that they have permission from rights holders to reproduce any copyrighted material. Any disclosures are made in this section. The external blind peer reviewers report no conflicts of interest.