
Abstract
Acute exacerbation of chronic obstructive pulmonary disease (AECOPD) is a sudden and sustained worsening in cough, dyspnoea and/or sputum production in patients with COPD. AECOPD is an infrequent occurrence in mild COPD, but is a common feature of moderate to severe COPD. It is essential to treat AECOPD early to prevent morbidity and mortality related to the disease. The treatment can be administered at home or in hospital depending on the facility and patient condition. The pharmacological and non pharmacological therapies are essential component of management and complimentary to each other. Prevention of further exacerbation after its optimum treatment is as important as the treatment, as these episodes lead to progressive decline in lung function. Evidence based management; newer advances and direction for future research are included in this review.
Introduction
Chronic Obstructive Pulmonary Disease (COPD) is a preventable and treatable disease. The pulmonary component characterized by airflow limitation is not fully reversible and is usually progressive, 1 whereas the extra pulmonary component contributes significantly to the morbidity related to the disease. The clinical spectrum of COPD ranges from stable COPD to acute exacerbation of COPD (AECOPD). Exacerbations are infrequent in early COPD and are largely a feature of moderate-to-severe disease. 2 They are often referred as ‘COPD lung attack’. AECOPD has clinical consequences ranging from a self-limited illness to progressive respiratory failure.3–6 The average patient with COPD experiences two episodes of AECOPD per year, and 10% of these episodes require hospitalization. 7 The average duration of an episode is 7 days, although it may take several months for the patient to return to baseline functional status.4,5,8 Thus, prevention and optimum, evidence based treatment of AECOPD is essential for an overall management of COPD.
Definition
AECOPD is a sudden worsening in airway function and respiratory symptoms in patients with COPD. According to GOLD (Global initiative for Obstructive Lung Disease) guidelines an exacerbation of COPD is defined as an event in the natural course of the disease characterized by a change in the patient's baseline dyspnoea, cough, and/or sputum that is beyond normal day-to-day variations, is acute in onset, and may warrant a change in regular medication in a patient with underlying COPD. 9
Etiology of Exacerbation
The diagnosis of AECOPD is made clinically when a patient with COPD experiences a sustained (eg, 24–48h) increase in cough, sputum production, and/or dyspnoea. 10 It is essential to determine the cause of worsening of symptoms for appropriate clinical management. The available evidence suggests that at least 80% of the AECOPD are infectious in origin. Of these infections, 40% to 50% are caused by bacteria, 30% by viruses, and 5% to 10% by atypical bacteria.11–21 Air pollutants like particulate matter, sulphur dioxide, nitrogen dioxide, and ozone have been shown to increase hospital admissions due to AECOPD.22–27 Cardiac dysfunction may be another important factor in AECOPD. 28 It has been observed that acute left heart dysfunction occurs in 25%–30% of patients with AECOPD.29,30 Presence of right heart failure is known to precipitate left heart failure because of comorbid illness and decreased cardiac output reduces oxygen delivery to respiratory muscles, contributing to respiratory decompensation. 28 It is difficult to determine whether the left heart failure is the effect or the cause of AECOPD. Recent development in plasma biomarkers (discussed later) is useful in assessing if the cause of exacerbation is infection or left heart failure. Pulmonary embolism is a common trigger for unknown acute exacerbation; the prevalence may be as high as 25%.29,30 Nonpulmonary infections and pneumothorax can mimic an acute exacerbation or possibly act as “triggers.” In about 30% of cases of AECOPD, no specific cause is identified. Many of these episodes may represent the fluctuating natural progression of COPD or noncompliance to maintenance treatment. 10 The causes are summarized in Box 1.
Causes of exacerbation of COPD.
Bacterial infection
Viral infection
Air pollution
Left heart failure
Pulmonary embolism
Pneumothorax
Non pulmonary infection
Fluctuating natural progression of COPD
Noncompliance to maintenance treatment
Severity of Exacerbation
There are no definite investigations to confirm exacerbation. Winnipeg criteria based on Anthonisen's study on the role of antibiotic in AECOPD are useful for determining the presence and severity of AECOPD. These are also known as Anthonisen's criteria. It includes: increase in sputum purulence, increase in sputum volume, and worsening of dyspnoea. Type I (severe) has all of the three symptoms, type II (moderate) has two, and type III (mild) has one symptom plus at least one of the following: upper respiratory infection in the past 5 days, fever without another apparent cause, increased wheezing, increased cough, or increase in respiratory rate or heart rate by 20% above baseline. 31
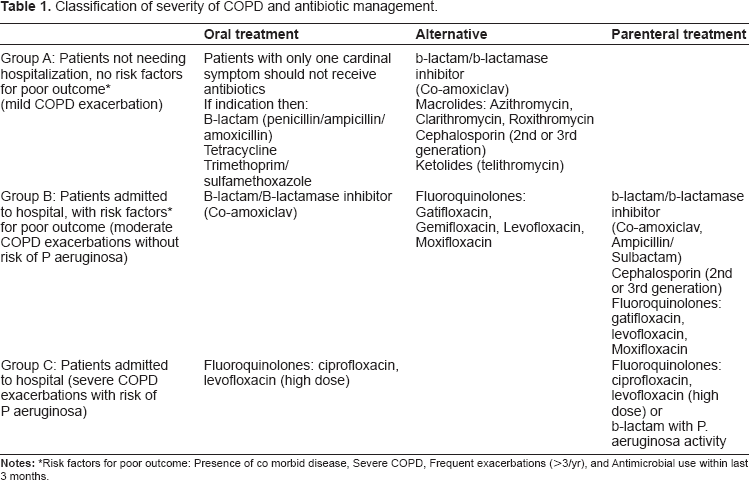
The Canadian guidelines have also laid down scoring system to assess severity of AECOPD for antibiotic therapy based on factors known to have poor response to therapy like age more than 65 years, forced expiratory volume in one second (FEV1) < 50% predicted, frequent exacerbations and significant comorbid illness (Table 1). 32 Another study has classified the severity based on therapy required and is useful for determining the prognosis and outcome of AECOPD. As per the study, mild requires oral steroid, oral antibiotics and SpO2 is more than 92%, moderate: parenteral steroid, antibiotics and SpO2 > 92%, severe: PaO2 < 60 mm of Hg; PaCO2 < 50 mm of Hg; normal pH, very severe: PaO2 < 60 mm of Hg; PaCO2 > 50 mm of Hg; normal pH, life-threatening: PaO2 < 60; PaCO2 > 50; pH < 7.35. 33 However, these are not validated prospectively, hence Anthonisen's/ Winnipeg criteria remains the most useful classification for the severity of AECOPD.
Classification of severity of COPD and antibiotic management.
Investigations for AECOPD
Objective confirmation of the diagnosis of COPD is usually not obtained in 50% of patients who present in exacerbation. 34 Spirometry is usually not feasible at the time of exacerbation. A typical history of smoking and the presence of cough, sputum, and breathlessness with reduced breath sounds and wheezing are the usual pointers to a diagnosis of COPD. 35 The investigations are however required to rule out left heart failure, embolism, pneumonia and pneumothorax and to assess the severity of exacerbations for determining whether the patient requires treatment at home, hospital or in intensive care unit (ICU). Chest radiograph, electrocardiogram and 2 dimensional echocardiography are essential for determining the cause. Whereas, pulse oximetry and arterial blood gas analysis are essential for severity assessment, decision regarding ICU management and subsequent monitoring. 32 Biochemical investigations are useful for assessing comorbid illnesses. Gram stain has limited role in etiology as patients of COPD have colonization with bacteria and is only useful when exacerbations are frequent, or infection with virulent/resistant bacteria is suspected. 32
Management Options for AECOPD
Clinical management consists of pharmacological and nonpharmacological approach which can be administered at home or in the hospital. The pharmacological approach is ABC approach, consists of A = Antibiotics, B = Bronchodilators, C = Systemic Corticosteroids. The nonpharmacological approach consists of oxygen therapy, physiotherapy, noninvasive mechanical ventilation (NIV) and invasive mechanical ventilation (IMV) in the form of assisted and controlled mechanical support. In proven COPD patients, depending on the initial assessment of history and severity of exacerbation, home management versus hospital management is considered. For end stage COPD patients, nurse administered home care is emerging as an alternative to hospitalization in selected patients without acidotic respiratory failure. Algorithm for management at home is shown in Figure 1. Those who cannot be managed at home should be hospitalized and managed in general ward, high dependency care unit, or ICU depending on the clinical scenario. Indications for hospital admission of AECOPD are given in Box 2. Indications for ICU admission are enumerated in Box 3.
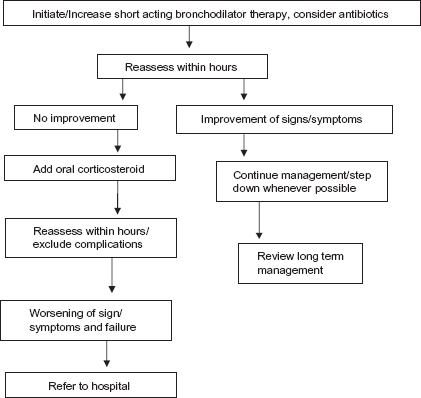
Flow chart for home management of AECOPD.
Indications for hospital admission COPD exacerbations.
Severe underlying COPD with frequent exacerbations
Inadequate response of symptoms to OPD/home management
Inability to eat or sleep
Onset of new physical signs (cyanosis, peripheral edema)
Home support not available
Presence of comorbities like pneumonia and left heart failure
Diagnostic uncertainty
Older age
Altered mentation, worsening hypoxia and new or worsening hypercapnia, arrhythmias
New or worsening corpulmonale
Indications for ICU admission for AECOPD.
Severe dyspnea not responding to emergency therapy
Altered mentation, lethargy, respiratory muscle fatigue
Severe/worsening respiratory acidosis (pH < 7.25), severe/worsening hypercapnia (PCO2 > 60 mmHg), severe/worsening hypoxia (PaO2 < 40 mmHg) in spite of supplemental controlled oxygen therapy and noninvasive ventilation
Requirement of invasive mechanical support and hemodynamic support ie, vasopressors
Pharmacological management
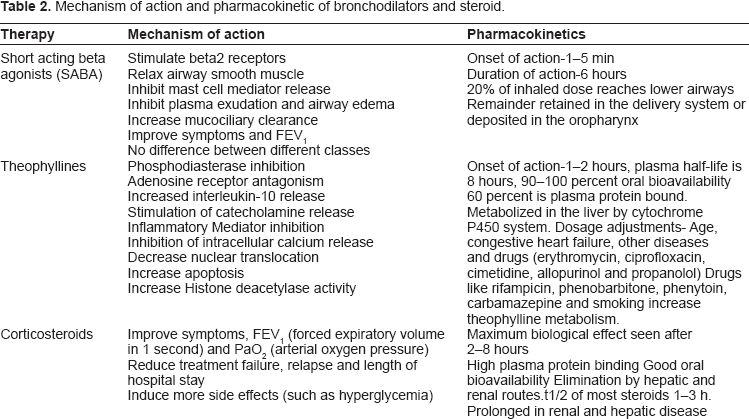
Pharmacotherapy is the cornerstone of AECOPD management in hospital. These include bronchodilators, antibiotics, and corticosteroids. Short acting inhaled beta2 agonists (SABA) are the preferred bronchodilators for exacerbations; addition of an anticholinergic is recommended. No clinical studies have evaluated the role of long acting beta2 agonists and anticholinergic. 1 Drugs include salbutamol (albuterol), levosalbutamol, and terbutaline, ipratropium bromide delivered via a nebulizer or meter dose inhaler (MDI) and spacer. 36 Systemic corticosteroids also have an important place in therapy. The mechanisms of action and pharmacokinetics of the above drugs is given in Table 2. 37 Antibiotics reduce risk of treatment failure, mortality and sputum purulence in moderate to severe exacerbations. Oral route is preferred and is cheaper than systemic route. 38 Antibiotic treatment in exacerbations is described in Table 1. 1 The flow chart for the management of AECOPD is shown in Figure 2.
Mechanism of action and pharmacokinetic of bronchodilators and steroid.
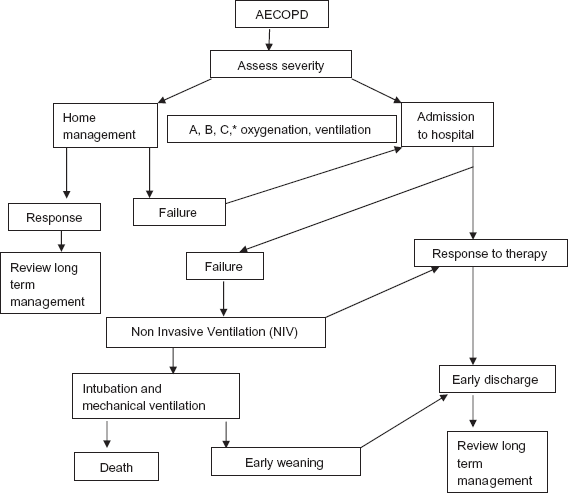
Flow chart for hospital management of AECOPD.
Nonpharmacological management
The aim of nonpharmacological management is to maintain patient's oxygenation status optimally. Oxygen delivered via different delivery devices and supportive noninvasive or invasive ventilation achieves this goal. Controlled oxygen support improves PaO2 with small increase in PaCO2. Repeat arterial blood gas measurements are needed in moderate to severe exacerbations while mild exacerbations can be monitored with pulse oximetry. 1 NIV reduces respiratory rate and improves PaO2, PaCO2, and pH; and decreases mortality, need for intubation, treatment failure and length of hospital stay. It is also cost effective.1,10,32 Indications for use of NIV are described in Box 4. Contraindications for use of NIV are given in Box 5. Invasive mechanical ventilation improves life threatening acute respiratory failure. Indications for use of invasive mechanical ventilation are listed in Box 6.
Indications of Non Invasive Ventilation (NIV) in AECOPD.
Moderate to severe dyspnea with use of accessory muscles of respiration or paradoxical abdominal motion
Moderate to severe acidosis (pH < 7.35) and/or hypercapnia (PaCO2 > 45 mmHg)
Respiratory rate >25 cycles/min
Contraindications of Non Invasive Ventilation (NIV) in AECOPD.
Respiratory arrest
Cardiovascular instability
Uncooperative patient
High aspiration risk
Viscous or copious secretions
Recent facial, oropharyngeal or gastroesophageal surgery
Craniofacial trauma or burns
Indications of Invasive Mechanical Ventilation (IMV) in AECOPD.
Unable to tolerate NIV or NIV failure or NIV contraindicated
Severe dyspnea with use of accessory muscles of respiration with paradoxical abdominal motion
Respiratory rate >35 cycles/min inspite of trial of NIV
Life-threatening hypoxemia
Severe acidosis (pH < 7.25) and/or hypercapnia
(PaCO2 > 60 mmHg)
Respiratory arrest
Impaired mental status
Cardiovascular complications (hypotension, shock)
Other complications
Clinical Studies of Therapeutic Options for AECOPD
Hospital at Home approach
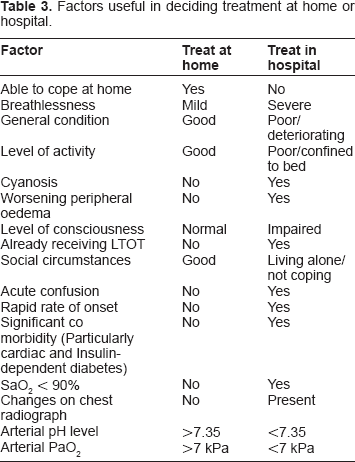
Various studies have been performed to evaluate hospital at home approach (HaH). In a randomized controlled trial for the efficacy of HaH; Shepperd et al reported a preference for inpatient care in their cohort of 32 patients with COPD. 39 In contrast, a similar trial with 184 patients, a satisfaction questionnaire was administered to the HaH arm and 95% of respondents reported complete satisfaction. 40 Ojoo et al did a randomized control trial where they studied patient and caregiver's preferences for home vs. inpatient care which showed that both patients and caregivers were significantly more likely to prefer domiciliary care if they were in the HaH arm. Since patients had to be willing to be looked after at home, both patients' and caregiver's perceptions of the benefits of HaH care were reinforced by their experience. 41 Felix et al found no significant differences between hospital at home and inpatient care for readmission rates and mortality two to three months after an initial exacerbation of COPD. 42 Thus, HaH care of acute exacerbations of COPD is the preferred option in suitable patients. The factors deciding hospital vs. home approach are given in Table 3.
Factors useful in deciding treatment at home or hospital.
Antibiotics
The role of bacteria in exacerbations has not been established with reasonable certainty since bacterial species are present in the airways of 25%-50% patients with COPD even in stable conditions.43–45 Many studies have shown that a routine antibiotic shortens the severity and/or the duration of an AECOPD episode, but this finding is not universal. One of the landmark studies has shown that antibiotics ameliorate improvement in peak expiratory flow rate (PEFR) when used empirically for Anthonisen's type I and II exacerbation. The study did not show any benefit to the patients with Anthonisen's type III exacerbation. 46 Green colored sputum in a patient with a history of COPD is 99.4% sensitive and 77% specific for the yield of high bacterial load and may identify a clear subset of patients likely to benefit from antibiotic therapy. 47 It has been shown that if patients requiring mechanical ventilator are not treated with antibiotics the mortality and incidence of secondary nosocomial pneumonia increases.1,48
Antibiotic selection should be directed against Streptococcus pneumoniae, Moraxella catarrhalis and Haemophilus influenzae. Broader antibiotic coverage is indicated for suspected Pseudomonas aeruginosa infection. 49 The guidelines1,32,45 recommend that amoxycillin, doxycycline and cotrimoxazole should be used as first line agents if risk factors for poor outcome ie, comorbid illness, severe COPD, frequent exacerbations (more than 3 per year) and antimicrobial use in last 6 months are absent. If the first line agents fail, the patients may be given cefuroxime axetil, amoxycillin-clavulinic acid, azithromycin or clarithromycin. The guidelines recommend that newer generation flouroquinolone should be reserved for treatment failures and those with presence of risk factors for poor outcome, although recently conducted trials, TACTIC (acuTe exACerbaTions of chronIC bronchitis), 50 GLOBE (Gemifloxacin Long-term Outcomes in Bronchitis Exacerbations) 51 and MOSAIC (Moxifloxacin to Standard oral antibiotic regimen) 52 studies have shown a better outcome with newer generation flouroquinolones as a first line therapy. Patients with risk of pseudomonas infection ie, recent hospitalization, frequent use of antibiotic (4 courses in last one year), severe exacerbation, and isolation of the organism require treatment with additional antipseudomonal drugs 32 (Table 1).
Thus, though treating an AECOPD episode early improves the speed of functional recovery, the exact role of antibiotic in AECOPD is not defined. 29 Controversy also exists regarding the use of newer and more broad-spectrum (and more expensive) antibiotics. Some light although, has been shed by a few recent trials. The patients who are treated with first line antibiotic have a higher relapse 53 and fail more frequently 54 and are hospitalized more often within 2 weeks of outpatient. 54 However, another study has shown that use of home oxygen correctly and frequency of exacerbation rather than the choice of an antibiotic affect the treatment outcome. 55 So, overall judicial use of antibiotics is required for optimal management of AECOPD.
Short Acting bronchodilator
Although there are no trials for short acting bronchodilator (SABD) agents, their use in the treatment of exacerbations has not been questioned.56,57 There are three relevant issues related to the use of SABDs during exacerbations: efficacy of the drugs, drug combinations, and the delivery system for inhaled treatment. There is no evidence of a difference between classes of SABDs in terms of bronchodilatation. A combination of SABDs given sequentially in exacerbations does not provide additional benefit. 58 A systematic review of the route of delivery of SABDs found no significant differences in forced expiratory volume in one second (FEV1) between the use of hand held MDIs with a good inhaler technique (with or without a spacer device) and nebulizers.
Methylxanthines
The GOLD report mentions a controversial status on use of methylxanthines in COPD exacerbations. Barr et al in A meta-analysis examined data from 4 randomized controlled trials on methylxanthines in exacerbations of COPD and failed to show a consistent benefit with methylxanthines. They concluded that methylxanthines do not confer statistically significant benefit for lung function, clinical outcomes and symptoms in patients with exacerbations of COPD, but significantly increase nausea and vomiting. 59 However anti-inflammatory effects of low dose theophylline are known to prevent progression of stable disease and histone deacetylase (HDAC) activity helps in unlocking steroid resistance and increasing responsiveness to steroids. 36
Corticosteroids
Systematic reviews60–62 have favored the use of systemic steroids during AECOPD. The reviews are based on trials that have shown statistically significant improvements in lung function during the first 3 to 5 days.63–65 Also, it has been demonstrated that a statistically significant improvement occurs in arterial PaO2 in the first 72 hours in favor of the steroid group compared to placebo.65,66 Significantly shorter duration of hospitalization has been demonstrated by Niewoehner and Davies with steroid therapy.63,64 It has also been shown that there are no differences in the clinical outcomes between the 2 vs. 8 week course. 64 Also, there is evidence supporting reduced likelihood of relapse and prolongation of time to next exacerbation with short course steroid treatment in exacerbation. 67 However, systemic steroid use has been shown to increase the adverse events like hyperglycemia by 2.7 times.60,64
The various trials however so far have not determined the optimal dose and duration of treatment. The guidelines recommend that 30–40 mg of oral prednisolone daily for 7–10 days is safe and effective. 1 Whether the patients with mild disease (FEV1 60%–70%) also benefit from a course of oral steroid is unknown. The role of inhaled steroid has also not been defined. A recently published prospective randomized trial comparing high dose nebulised budesonide with prednisolone 30 mg twice daily for 3 days showed no significant difference between active treatments both being superior to placebo in terms of recovery of FEV1. 68 However, high dose nebulized corticosteroids have been tested in a limited number of studies in AECOPD. 32
Overall, the steroid use should be tailor made depending on the severity of exacerbation and risk benefit ratio, also more trials are required to determine the exact dose and duration of steroid and role of inhaled steroid during AECOPD.
Oxygen therapy
AECOPD may cause significant hypoxemia. Studies have shown that the PaO2 falls from 55–60 mmHg to 25–50 mmHg during an exacerbation.69–71 The administration of oxygen has potential therapeutic benefits, which include relief of pulmonary vasoconstriction, decrease on right heart strain, and decrease in myocardial ischemia (if present), and it has become part of the “standard-of-care” during an acute decompensation. 72 However, there is marked variation in the response of individual patient to oxygen. King et al gave 24% oxygen to patients with exacerbations of chronic respiratory failure. They recorded a mean PaO2 of 40.4 mm Hg in these patients on room air and a mean PaO2 of 57.3 mm Hg after 30 to 60 minutes of 24% oxygen but in 15 out of 40 patients PaO2 did not cross 50 mm Hg. 73
To study the role of Venturi mask vs. nasal prongs Agusti et al gave oxygen to 18 patients with COPD with acute respiratory failure in a prospective randomized crossover study. 71 Oxygen was given via nasal prongs at 2–4 l/min and Venturi masks at 24%-28% for 24 hours and crossed over subsequently via each device. Patients had oxygen saturation <90% for a mean of 3.7 hours using the Venturi mask and 5.4 hours using nasal prongs. It was concluded that neither Venturi mask nor nasal prongs worsen respiratory acidosis significantly and Venturi mask is better than nasal prongs for improving hypoxemia.
It is essential to administer low FiO2. Plant et al found a significant negative correlation between pH and PaO2 in 972 patients after oxygen therapy. The more oxygenated patients became the greater was the likelihood of the respiratory acidosis. More than 50% of hypercapnic patients were acidotic if the PaO2 was greater than 75 mm Hg. 74 Thus, oxygen therapy should be controlled and saturation should be aimed between 90%-92%.
Noninvasive Ventilation(Niv)
During the last few years, several studies have consistently shown that noninvasive positive-pressure ventilation improves respiratory acidosis, improves respiratory rate, decreases the likelihood of requiring invasive mechanical ventilation, reduces hospital stay and possibly increases survival time.75–82 Some of these trials have compared NIV to conventional ventilation (endotracheal ventilation). 79 Others have compared NIV to usual medical care and subsequent need for intubation.75–77 When NIV was compared to usual medical care it resulted in improvement in PaCO2, respiratory rate, and pH in the first hour of treatment; fewer complications and shorter duration of hospital stay. 77 Thus, noninvasive mechanical ventilation has become an acceptable option for ventilatory support of AECOPD except in the conditions described in Box 5.
Invasive Mechanical Ventilation(Imv)
AECOPD may lead to pump failure due to reduced spontaneous minute ventilation because of severe airflow limitation and increased work of breathing secondary to intrinsic positive end-expiratory pressure [PEEPi] created by air trapping. 10 NPPV reduces the need for invasive mechanical ventilator support, however in certain cases due to progressive respiratory fatigue and acidosis invasive mechanical ventilator is essential. The survival on mechanical ventilator depends on multiple factors. Esteban et al studied the characteristics and outcomes in adult patients of AECOPD receiving endotracheal ventilation in a 28 day international study involving 361 ICUs, 20 countries and 15,757 patients. The drawbacks of the study were heterogeneous population of ventilated patients and limited availability of information. It was concluded that survival among ventilated patients depend not only on factors present at the start of ventilation but also on development of complications and patient management in intensive care unit. 83 Nevins et al retrospectively studied predictors of outcome for patients with COPD requiring invasive ventilation. 84 Presence of comorbidity and severity of acute illness were found to be the predictors of outcome. A high mortality rate was also observed in those who required >72 hrs mechanical ventilation. Rieves et al studied a population of patients with severe COPD and acute respiratory failure and examined correlates for survival at the time of intubation. It was concluded that apart from severity of airway obstruction, development of acute renal failure and presence of opacities on chest radiograph at the time of intubation are important for survival. 85 The predictors of poor outcome are summarized in Box 7.
Determinants of mortality on Invasive Mechanical Ventilation (IMV) in AECOPD.
Development of complications
Patient management in ICU
Presence of cormorbidity
Severity of acute illness
>72 hrs mechanical ventilation
Severity of airway obstruction
Development of acute renal failure
Presence of opacities on chest radiograph at the time of intubation
The mean duration of mechanical ventilation for COPD patients varies in various groups from 1.2 to 22 days.83,84 Overall, the length of stay in ICU in COPD patients is less than adult respiratory distress syndrome (ARDS) patients and the mortality is also lower in COPD patients compared to patients receiving mechanical ventilation because of acute respiratory failure of other etiologies. 83 The weaning from ventilator can be difficult and prolonged. The role of T piece and pressure support in weaning is controversial and NIV is useful for weaning but does not reduce mortality. 86
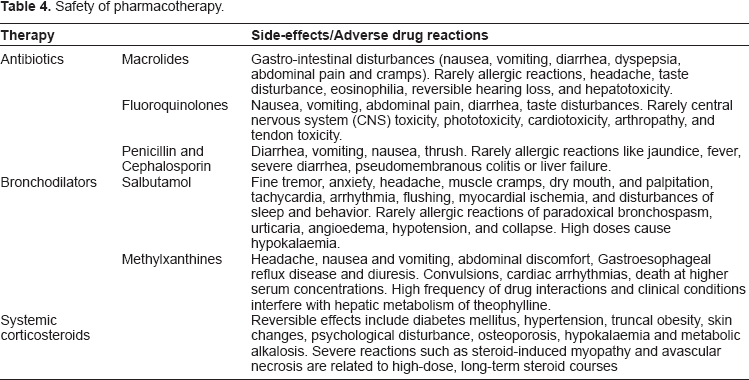
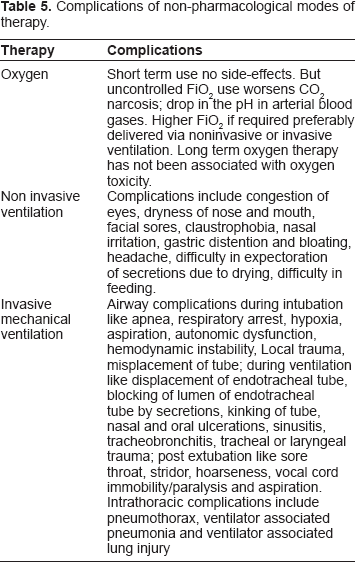
Safety of Aecopd Therapy
The management modalities differ widely in their safety profile. Antibiotics spectrum used in AECOPD is vast so are their side-effects. The adverse drug reactions of commonly used antibiotics are given in Table 4.87–89 Safety of bronchodilators and corticosteroids is also enumerated in Table 4.90,91 Complications associated with use of non pharmacological modes of therapy ie, oxygen, Noninvasive ventilation, mechanical ventilation are listed in Table 5.1,92
Safety of pharmacotherapy.
Complications of nonpharmacological modes of therapy.
Efficacy and Place of Therapeutic Options in AECOPD
HaH care of acute exacerbations of COPD is the preferred option in suitable patients. Inpatient hospital treatment is advisable for critically ill patients (Table 3). Exclusions to HaH are concomitant medical conditions requiring admission, residence over 15 miles from hospital, complications of the exacerbation, acidosis, cor pulmonale, and acute changes on chest radiograph. Good domiciliary support is crucial for HaH approach. 41
Antibiotics are recommended for Anthonisen's type I and type II with increased sputum purulence exacerbation and severe exacerbation of COPD requiring mechanical ventilation. Short acting inhaled beta2 agonists are the preferred bronchodilators for exacerbations; addition of an anticholinergic is recommended. Methylxanthines have a controversial role and are considered second line of therapy. No clinical studies have evaluated the role of long acting beta2 agonists and anticholinergic. 1 Systemic corticosteroids shorten recovery time; improve FEV1 and PaO2; and reduce risk of relapse, treatment failure and length of hospital stay. Oxygen therapy is a cornerstone for management of exacerbations. Low flow oxygen delivery via nasal prongs or Venturi masks are useful for achieving PaO2 > 60 mmHg or SpO2 > 90%. NIV improves respiratory acidosis, decreases respiratory rate, breathlessness and hospital stay. It reduces the need for intubation and mechanical ventilation. Invasive ventilation benefits only patients with less severe disease, not initially using LTOT, with no comorbities and reversible cause of respiratory failure (infection).
Patient Preference of Therapeutic Options in AECOPD
The available medical facilities, social background and awareness about the different modalities of treatment in the medical and paramedical staff largely affect the patient preferences. Hence though the revolution of home care has started in the developed countries for treatment of COPD exacerbations a decade ago, in countries like India HaH still has to gain acceptance in the medical fraternity as patient preferences are largely influenced by the treating physician. Concluding patient preferences will vary according to the severity of exacerbation, social, financial and medical support.
Consequences of AECOPDS
Exacerbations not only account for 10% in hospital mortality in COPD patients but also have an effect on the health related quality of life (HRQOL). 93 Repeated episodes of COPD exacerbations may potentially impair lung tissues and lead to an accelerated rate of decline in pulmonary function. 94 Donaldson et al 95 have reported a greater decline in FEV1 in patients with frequent exacerbations. A recently published Toward a Revolution in COPD Health (TORCH) study showed that patients experiencing greater frequency of exacerbations during the 3-yr study period had a faster decline in FEV1. Also, frequent exacerbations (more than two per year) are associated with increased dyspnoea, reduced exercise capacity, 96 greater decline in health status97,98 and increased likelihood of becoming housebound.95,99 Thus, prevention of exacerbation is as important as the treatment. Important preventive measures of COPD exacerbation are active immunizations, including influenza and pneumococcal vaccinations; chronic maintenance pharmacotherapy and optimum non pharmacological management. 100 The clinical management of AECOPD is incomplete if preventive therapy of vaccination and optimum management of COPD is not considered once the patient recovers from AECOPD.
Recent Advances in Aecopd Management
Biomarkers in AECOPD
The role of biomarker in AECOPD is not yet well defined due to paucity of trials and wide range of inflammatory mediators, cytokines, acute phase reactants found in stable COPD itself and their variation in levels due to severity of the disease, presence of comorbidities and treatment. 101 The best option probably is to monitor levels individually, rather than establishing cut-off points for the general COPD population. It is widely accepted that COPD is associated with an increased systemic inflammatory response in comparison with control individuals 102 and that this inflammatory response is amplified during exacerbation episodes. It has been observed that high levels of procalcitonin (PCT), C-reactive proteins (CRP) and pro atrial natriuretic peptide (ANP) present during an exacerbation episode tend to decrease once the patient is stable. On the contrary, levels of neopterin tend to be higher once the patient is in a stable state. 103
About the role of biomarker in the etiology of AECOPD; it has been observed that patients with bacterial infection have higher level of CRP 104 ; triggering receptor expressed on myeloid cells (sTERM) 105 and PCT. 106 Another recent study has shown that sputum interleukin (IL)-1β, serum C-X-C ligand 10 (CXCL10) and peripheral eosinophils are biomarkers of bacteria, virus or eosinophil associated exacerbations of COPD. 107 Similarly NT-pro brain natriuretic peptide (BNP) and troponin T are useful in excluding AECOPD associated with left ventricular dysfunction. NT-proBNP is more accurate of the two. 108
Heliox Use in AECOPD
In severe airway obstruction, uses of low-density gases (eg, 80:20, 70:30, or 60:40 helium/oxygen or heliox) can help in reducing inspiratory work by facilitating lung emptying due to reduced driving pressure and improved flow rate due to reduction in gas density. 109 If heliox is used, it needs to be ascertained whether the ventilator is functional in the presence of heliox and flow sensors are recalibrated. 10 A recent meta-analysis however, has concluded that there is insufficient data to support its use. 110 One of the randomized trials included in the meta-analysis evaluated the administration of heliox as a driving gas for nebulization of bronchodilators during the first 2 hours of treatment. The use of heliox in this trial failed to improve FEV1 faster than air. 111 A retrospective study however has shown that heliox reduces mortality rates significantly. 112 Thus, more studies are required to ascertain the use of heliox.
Conclusions
The principles of clinical management options of COPD exacerbations are well established and backed by scientific evidence. The evaluation of the cause and the severity of exacerbation of COPD is the first step in deciding whether outpatient or in hospital treatment would be formulated for the patient. Antibiotics, bronchodilators, corticosteroids are the crux of pharmacotherapy. Supportive nonpharmacological management assists in optimizing the therapy. Concluding education of patients and caregivers about the management options and their outcomes, especially hospital at home approach for end stage COPD patients needs to be emphasized to decrease unnecessary hospitalization and the financial burden of illness in these patients. Finally, adequate optimum management of the patient on discharge should be formulated to prevent recurring exacerbations. Future studies should be directed at determining the exact cause and etiopathogenesis of exacerbation; choice of antibiotic and its indications; optimizing the steroid therapy; use of long acting bronchodilators and improving ventilator management and weaning methods.
Footnotes
Disclosures
Author(s) have provided signed confirmations to the publisher of their compliance with all applicable legal and ethical obligations in respect to declaration of conflicts of interest, funding, authorship and contributorship, and compliance with ethical requirements in respect to treatment of human and animal test subjects. If this article contains identifiable human subject(s) author(s) were required to supply signed patient consent prior to publication. Author(s) have confirmed that the published article is unique and not under consideration nor published by any other publication and that they have consent to reproduce any copyrighted material. The peer reviewers declared no conflicts of interest.