
Abstract
Introduction
E-mentoring uses electronic communications to build and maintain a mentoring relationship. A previous study found E-mentoring to be beneficial to surgical trainees when delivered by a single E-mentor. This study aimed to see if these benefits persisted within a larger network of surgical E-mentors.
Methods
Surgical ST1 to ST3 trainees (E-mentees) and E-mentors were recruited in 2007. The study ran over one year with five questionnaires prompting discussions of a range of issues. At study end, a feedback questionnaire was sent via an independent third party.
Results
Twenty three E-mentees were recruited, 16 (70%) were male, median age was 28 (IQR 2). Fifty four surgical E-mentors volunteered, the majority being Specialist Registrars (n = 52; 96%). E-mentees found the process to be very useful in identifying the good and bad points of their jobs. E-mentoring was not useful for improving academic knowledge, operative skills or clinical management.
Conclusions
This study shows that E-mentoring is beneficial to surgical trainees who are engaged in the process. The process encourages reflection and was a useful source of advice but there remains areas where its scope is limited.
Introduction
“People do grow, learn, thrive and excel when organisations make provision for particular and specific interpersonal support at key times. The skills of training, instructing, advising, coaching, empathising, exploring, guiding, enabling, catalysing, challenging, encouraging, summarising and reflecting all have a place in the mentor's toolkit. The specific situation and best interests of the mentee will determine the selection and mix.” 1
Mentoring is a relationship between two people in which trust and respect enables problems and difficulties to be discussed in an open and supportive environment. 2
Connor studied a group of senior doctors as mentors, and felt that all junior doctors, newly appointed consultants and senior doctors who felt isolated might benefit from mentoring. 3 While there is increasing evidence for face-to-face mentoring, there is still little considering E-mentoring. “Cultivating the Thinking Surgeon” by de Cossart and Fish highlighted that support and reflection should be modernised to the benefit of both surgeons and patients. 4
E-mentoring has identical aims as face-to-face mentoring but it primarily uses electronic communications (internet, email, telementoring, cybermentoring) to build and maintain the mentoring relationship. 5
E-mentoring has been used in both the public and private sector: within the NHS and in business to support courses (eg, MBA), provide career or business development advice and to provide a link between students and future employers.6–9 The advantages and disadvantages of E-mentoring have been previously summarised in depth by Clutterbuck and colleagues.10,11 There remains little research on the effectiveness, dynamics, or results of E—mentoring in the context of Medical Education.
Junior doctors need to experience a culture of development and learning in their early training, where asking for help and engaging in dialogue about personal and professional issues is encouraged.
Surgeons in training face a wide variety of challenges which include maintaining their underlying clinical and medical acumen while developing a range of new practical skills (operating in theatre, learning endoscopy) and ensuring high quality care to a busy ward of peri-operative patients. Even non “on call” days are long (8 am to 6 pm), challenging clinical and operative decisions may need to be made at any time of day or night with senior help perhaps a phone call away. In addition to this the volume of formal assessment and ward administration has increased with a loss of facilities (desks, computers, offices) to complete them.
Professional surgical exams remain the main hurdles to progression with ever present competition for more senior surgical jobs. These pressures inevitably encroach on personal lives and relationships, before considering the overlay of major life events such as bereavement, birth of children or illness. So there are many potential issues and areas which a surgical trainee might benefit from discussing with a mentor.
It would seem logical that the best mentors would be those that have “been through it”. Mentoring however takes time and senior surgical trainees and consultants have ever increasing burdens themselves. A previous study of surgical E-mentoring by this author saw one E-mentor provide support to14 surgical trainees in another training region of the United Kingdom (UK). E-mentoring was found to be technically feasible and the majority found the process useful as part of their global development as future surgeons. It was most useful in encouraging reflection on current training, identifying the good points of a job, providing career advice and improving audit skills. There were mixed opinions to its usefulness in improving research, operative skills, clinical management or in helping achieve a better work/life balance. It was not useful in improving academic knowledge or in changing the bad points identified in a job. With these results in mind, the next stage was to create an E-mentoring network in the Northern Region to see if these results were reproducible on a larger scale, with multiple mentors.
The aim of the study was to examine if the potential benefits of E-mentoring persisted within a larger network of surgical E-mentoring. Secondary aims included ensuring its technical feasibility and focusing on broadening the range of areas where E-mentoring could be beneficial to trainees.
Methods
Recruitment
The prospective case study was advertised by email and via documents included in each new surgical starter pack, for years ST1 to ST3 in the Northern Deanery of the UK. A 10 minute oral presentation was given at three compulsory Deanery inductions for surgery. The programmes aim was to provide independent, confidential, primarily electronic based mentoring to surgical trainees (ST1 to ST3). Ideally, each E-mentee would gain support, encouragement and advice with regards to their professional, personal and career issues over an initial year period.
Five crucial statements about the process were highlighted: it was confidential and voluntary, independent of assessment and endeavoured to aid development through support and constructive challenge. Feedback was requested at intervals and all participants knew it was a research study whose results would be published in peer reviewed journals. The initial letter in the induction packs invited them to email the E mentoring coordinator (DM) if interested. Inviting contact and requiring an email reply to confirm interest were hoped to be markers of those who would engage in the process, be IT competent and be entering into the process without coercion. No surgical speciality was excluded. Each interested E-mentee was sent a consent form to read, complete and return electronically. The E-mentoring coordinator signed each completed consent form and returned it by post to their registered address. With this individual E-mentee consent and observation of appropriate ethical principles, additional institutional consent was not sought.
Matching provided each mentee with information of the mentors seniority, current specialty, likely long term career goal, hobbies and extra-curricular activities. Having a E-mentor in the same specialty was considered to be of potential benefit to the E-mentee although each was offered at least 3 E-mentors usually at least one of which was from another specialty. The majority of the surgical E-mentees enjoyed activity based hobbies similar to their E-mentors. Clear boundaries were to be agreed within each individual mentoring relationship.
Recruitment ran from July to October 2007 and mentees were matched as they entered the process. In 2007, there were 14 ST 1, 16 ST 2 and 40 ST 3 surgical posts in the Northern Region. Twenty nine trainees expressed an interest either verbally or via email. The E-mentee and E-mentor “journey” is illustrated in Figure 1.

The E-mentee journey.
The data collection was completed at one year as planned although mentoring relationships could continue at the discretion of both parties. Through the year, five “E-mentoring” questionnaires were sent to aid reflection and to provide prompts for discussion (Appendix A). E-mentees were advised to complete the questionnaires and send them to their E-mentor for review. The questionnaires covered a range of issues including recent operative and clinical training, positive and negative moments in the job, personal and professional achievements and future goals (Appendix A). This questionnaire would provide a rich source of discussion points for the E-mentor to probe and challenge during the intervening periods. Outside of these defined dates, E-mentees made email contact about new issues, reflections on previous discussions or updates on goals identified and achieved. E-mentees were encouraged to lead the mentoring process, with the E-mentor becoming more of a sounding board or critical friend rather than an advisor, particularly in terms of career advice.
A feedback questionnaire was sent to all E-mentees and E-mentors in November 2008 by an independent third party (Appendix B and C). On receipt of these questionnaires, the feedback was anonymised prior to forwarding to the author for data analysis. Once initial analysis was complete, the identify of each questionnaire was made available to enable full reflection of the process. The identities and research records of each participant were kept confidential on a non-networked computer using anonymised unique identifier numbers.
E-mentor Recruitment
All surgical registrars and General Surgical consultants in the Northern Deanery were emailed inviting them to be involved in the process. Those that confirmed interest by email received a copy of the information provided to E-mentees, a copy of the executive summary of the original surgical E-mentoring study and a summary of qualities and skills required of mentors published by the leaders in the mentoring field. This included basic competencies for mentors and mentees, 12 core competencies of a mentor from the mentees perspective (Fig. 2) 13 and ways of distinguishing a good mentor. 14 An additional table illustrated the many potential benefits of mentoring for the mentee, mentor and their host organisation. 15 Participation of all was voluntary with no funding, sponsorship or monetary rewards.

Mentor qualities.
E-mentors did not undergo formal face to face mentoring training but were provided with the details and evidence supporting the “Skilled Helper Model” devised by Egan. 16 Face-to-face mentoring training courses were available in the North East and E-mentors were encouraged to undertake the course, although no funding support could be offered. None of the E-mentors undertook this course during the study period. All E-mentors had easy and rapid access by phone or email to the E-mentoring coordinator (DM) and every two months received recent mentoring articles for their ongoing mentoring development.
On receipt of the “E-mentoring” questionnaires, E-mentors were requested to respond within 48 hours. Their responses would ideally prompt further discussions such as those illustrated in Figure 1. E-mentors were requested to forward their feedback to the E-mentoring coordinator (DM) as a method of ongoing E-mentoring training and as a quality assurance measure.
Data Analysis
All data was extracted by the lead author during the year long E-mentoring process and from the bimonthly and final feedback questionnaires. It was analysed manually using observer impression with the results presented in structured quantitative and qualitative forms. Percentages, tables and figures were created in Microsoft Word, Excel and Powerpoint. (Microsoft XP Professional 2003). The richest source of information and reflections came from the anonymised final feedback questionnaires.
Results
E-mentees
Twenty three E-mentees were matched with E-mentors over a 12 month period. 16 (70%) were male, median age was 28 (IQR 2), 17 (74%) attended Medical School in the UK and median years qualified was 4 (IQR 1). 16 (70%) were working in University teaching hospitals.
The majority of E-mentees required at least one reminder to complete the E-mentoring questionnaire (average 2 reminders) and overall, each E-mentee returned a median of 2 (range 0–4) of the five questionnaires. Table 1 illustrates the grade and speciality of each of the matched E-mentees and E-mentors. Two E-mentees withdrew from the process after six months due to work pressures in one and a preference for face-to-face mentoring for the other. Feedback questionnaires were received by 11, but only fully completed in 9. The response rate was therefore 42%.
Grade and speciality of matched E-mentees and E-mentors.

There was no obvious gender or age distribution to those that responded more frequently to questionnaires. One E-mentee was initially matched but when the mentor made initial contact and a baseline discussion was undertaken, the E-mentor recognised a potential competing interest which the E-mentoring coordinator agreed was an acceptable reason to re-match. The E-mentee declined to proceed with re-matching.
E-mentors
Recruitment focussed on the Northern Deanery Surgical Specialties although previous E-mentees and surgeons outside the UK were invited also. In total, 119 E-mentors were emailed. There was an excellent response leading to 54 (45%) E-mentors being available, the majority being Specialist Registrars in their 4th to 6th years of training (n = 52; 96%). Seven E-mentors had previously been E-mentees some of whom had moved into research, general practice or other specialties. Two were based outside of the UK (Australia, USA).
E-mentoring Questionnaires
E-mentees suggested a range of positive and negative experiences every month. Positive points included teaching others new skills, astute clinical diagnoses made, good patient rapport, congenial working atmosphere and growing operative confidence. Difficult working relationships with certain colleagues, work stress, delayed identification of critical illness, a range of clinical errors (administrative, informative, operative) and operative complications were the main negatives.
E-mentees felt well supported by their clinical supervisors and had regular contact and face-to-face discussions. Issues of aptitude for a surgical career tended to be discussed at the final job appraisal although the amount of feedback given at this time was variable. The majority of ST trainees felt they had a good work life balance, which they suggested was achieved by good time management, less onerous clinical posts and on call commitments, continued extracurricular activities and enjoyable team working. Future career concerns and exams did affect this balance.
Five of the E-mentors (21%) regularly forwarded their E-mentor responses to the E-mentoring coordinator. All of the feedback given to E-mentees had been constructive and appropriately phrased. In most cases, one aspect of the questionnaire had been focused upon, rather than all questionnaire headings. Most emails included elements of constructive challenge and would have encouraged the E-mentee to reflect. The E-mentoring coordinator reviewed and provided feedback to any email received from an E-mentor. This would include additional areas from the questionnaires that could warrant feedback or alternative methods of phrasing the response to the E-mentee.
E-mentee Final Feedback and Reflection
Eleven E-mentees (47%) responded. All felt that they had received enough information prior to joining the study and were aware they could withdraw at any time, without giving a reason. One E-mentee felt there could have been more information about the E-mentee and their role but the comments broadly suggested a legitimate, ethical, well organised study.
All had easy access to a computer although two had at some point found difficulty contacting their E-mentor. The majority of E-mentees responded to the questionnaire or their E-mentor before work or at home rather than during the working day. The questionnaire took 10–20 minutes to complete on each occasion.
Six of 11 E-mentees found their E-mentor raised issues and made suggestions that they had not previously considered. Ten of 11 were comfortable contacting via email, with 50% responding to the E-mentor comments. Seven considered making contact outside of the formalised questionnaire setting. Two felt an alternative mentor might have improved the relationship.
Reflecting on the process, E-mentees found the process to be very useful in identifying the good and bad points of their jobs and of some use in changing those bad points. E-mentoring was not useful for improving academic knowledge, operative skills or clinical management. It was of some use in focussing or improving research and audit skills. In their feedback, E-mentees had many positive impressions of E-mentoring (Table 2). These have been ordered in terms of organisational or location issues, communication, personal development aspects and workplace issues. Flexibility, convenience, informality and access to senior surgical advice were repeatedly mentioned. Figures 3–5 illustrate the impact of E-mentoring in terms of identifying good points of an E-mentee's job, helping change the bad points in that job and whether it was useful in achieving a better work life balance. These three aspects were chosen for figures as they could be considered important aspects of the mentoring role—not just to highlight what is going well and augment this progress but also to identify things that could be better and crucially help the E-mentee to find ways of making things better. In doing so, and taking a global approach to an E-mentees life, one would hope to see an improvement in work-life balance, which is sometimes challenging for surgical trainees. The majority found E-mentoring to be of at least some use to them.
E-mentee feedback—Benefits of E-mentoring.


Has E-mentoring been useful in identifying the good points of your job?

Has E-mentoring been useful in helping you change those bad points?

Has E-mentoring been useful in achieving a better work life balance?
When asked who might benefit from E-mentoring, all felt Specialty trainees ST1 to ST3 trainees might gain the most followed by ST 4 to 6. It was felt Foundation trainees would benefit more than consultants. The group were divided as to whether the E-mentoring sessions should deal with one topic per session rather than a broader outlook
Reasons given for lack of engagement included personal workload and a preference for face to face mentoring. Others found that their initial enthusiasm waned particularly if they “fell behind” on the questionnaires due to annual and study leave. Fewer forms, more open ended questions and less emphasis on objective measures (eg, number of operations performed) were suggested. Table 3 lists the identified drawbacks or areas for improvement and these have been ordered into communication challenges, email related aspects or other issues.
E-mentee feedback—drawbacks of E-mentoring.
Nine of the eleven E-mentees who responded to the feedback questionnaire felt that participating in E-mentoring had been beneficial and in addition would recommend the process to their surgical colleagues. Eight of eleven felt that they had developed both personally and professionally.
E-mentor Final Feedback and Reflection
Five E-mentors (22%) responded to the final questionnaire. None had IT difficulties but two found contact with their E-mentee problematic at times. All undertook the process in the evenings at home, taking 10 to 15 minutes to review the information and to provide some constructive feedback. None had been a mentor previously, two had met their E-mentee previously for other reasons and all were comfortable with undertaking the process by email.
The benefits identified are shown in Table 4 ordered in terms of convenience aspects, communication issues and surgically specific advice. Table 5 lists some of the drawbacks ordered by communication and then organisation or motivational problems. Flexibility in terms of timing and location, having a process separate from their place of work and the benefit of having access to the experience of a more senior surgeon were seen as positives. Time constraints still existed and the loss of non verbal cues and the asynchronous nature of the process were seen as potential negatives.
E-mentor feedback—benefits of E-mentoring.

E-mentor feedback—drawbacks to E-mentoring.

When considering who would make effective surgical E-mentors, the majority suggested specialist registrars, other senior surgical or other medical doctors or retired surgical consultants. E-mentors had varying views of the effectiveness of the process for E-mentees. It was seen as useful for reflecting on training, providing career advice and identifying the bad points of a job. There were mixed opinions to its usefulness in identifying the good points of jobs and in helping achieve a better work/life balance. It was not useful in improving academic knowledge, operative skills, research skills, clinical management and helping change the bad points identified in a job.
Although a good rapport was achieved if the E-mentee engaged in the process, the majority of E-mentors felt they gained little from being a mentor. The response rates from E-mentees was variable and in some cases non existent. Only occasionally was contact made outside of the pre determined E-mentoring questionnaire contacts. Reasons suggested included a lack of interest after the initial email, progress independent of the E-mentoring process and other priorities delaying or preventing completion of questionnaires. They felt that all surgical grades would benefit from mentoring with more junior trainees gaining the most.
Three of the five E-mentors who responded to the feedback questionnaire felt that participating had been beneficial to their E-mentee. Four of five would recommend to their future trainees and two felt they had personally developed professionally and personally.
Discussion
The study has shown the areas in which E-mentoring augments current surgical training and supervision (eg, encouraging reflection, career and research advice) and where it probably has less of a role (eg, enhancing operative and clinical skills). Overall it appears to be of benefit to those that actively engage in the process although some find face-to-face mentoring more suitable to their needs, character and presumably learning style.
There were a variety of reasons for lack of contact outside of the formal mentoring periods. Some felt there was a limit to the help they could receive from their E-mentor—“Other sources of advice readily available”, “mentor did not have access to higher level advice needed”, “Mentor did not have the ability to ‘open the doors’ that I desired”. For some, access to email was not convenient or “the process was less interesting as time passed”. Others “got far too busy and found obtaining some of the data time consuming” or had “plenty of people at work to seek advice from”. One found that the E-mentor “didn' t know me well enough to enable me to discuss certain topics”.
Encouragingly, those that responded to the feedback questionnaire would recommend E-mentoring to their colleagues and felt it might benefit both younger and more senior surgeons (ie, Foundation trainees and Consultants). E-mentees felt that surgical consultants or specialist registrars were the most appropriate surgical E-mentors. Retired surgical consultants in the same specialty or surgical staff grades were possible but none felt that other professionals (nurses, lawyers) or lay persons could be effective E-mentors
It was heartening to see all E-mentees being keen to become the next generation of Surgical E-mentors.
Six of the 11 E-mentees felt that not having met their E-mentor face to face probably made a difference to the relationship formed. Some felt that they were already receiving adequate support and challenge from clinical and educational supervisor. For some, whilst the questionnaire itself (Appendix A) took on average 10 minutes, the compiling of data and reflection of the previous two months clinical experiences took considerably longer. However, reflection does take time if it is done properly and the potential gains are considerable.
Privacy and confidentiality were seen as vital issues although no specific breach of either was cited. Some E-mentees realised that they had at times forgotten to reply and others thought that the written word could be misinterpreted in comparison to the spoken word. Some found the asynchronous nature of E-mentoring disrupted the flow of discussion and there was concern that more reserved people might be less engaged in putting their true feelings in an email.
There are a variety of different ways to conduct a mentoring process and a spectrum of formality to the process whether that be prearranged meetings or spontaneous sporadic contact. I chose to construct a formalised asynchronous process partly because of the nature and breadth of topics to discuss and to accommodate the on call rotas and varying daytime commitments specific to surgeons and surgical trainees. However, some of the spontaneity is lost by communicating in this manner, something that has previously been identified as a potential drawback to E-mentoring. 10 An online chat room would potentially restore this spontaneity and might foster a more immediate response between users. The potential gravity of the topics being discussed (eg, operative complications) would presumably require a more private and confidential medium. The implications for patient confidentiality and hospital trust responsibility would be even more far reaching.
It is worth bearing in mind that human communication is changing rapidly. Could it be that the next generation of doctors are more comfortable being mentored via text messages, mobile phone, skype and internet forums like Twitter than they are having a face to face meeting. They are certainly so much more technologically advanced and E-mentoring may provide an important bridge between maintaining private, individual contact while suiting the modern methods of communication.
Email and internet services were readily available to all surgical trainees and E-mentors both at work and home. Purchasing of new computer software and broadband were not required but future technologically advanced E-mentoring processes involving live discussion boards and on line conference calls would be more costly and require more complex (and expensive) security systems to be put in place. In turn, E-mentees and E-mentors would need IT tuition and a system of IT support. This study was achievable without funding or sponsorship but relied on the goodwill of many. In these harsh economic times, as long as the will and enthusiasm of mentors and mentees exist, such a programme could still be possible.
One of the limitations of the study is the lack of validation of the bimonthly or feedback questionnaires. The bimonthly questionnaires main focus was to prompt further email discussions and provide a more formalised construct to the contact between E-mentee and E-mentor. I had hoped that E-mentees and E-mentors would make contact out-with the formalised questionnaire emails, but this occurred rarely. When asked about this issue, some considered E-mentoring only at the alternate monthly contact, others had alternative mentors or supervisors who provided more relevant advice but no-one stated they felt impeded to make contact. The formalised nature of the emails may have contributed and perhaps an initial face to face meeting would have fostered a deeper, more trusting relationship.
The low response rate from E-mentees in particular does raise concerns regarding the validity of the data. The study size remains small also, although it remains the largest published surgically specific E-mentoring network.
Concentrating on surgical specialties potentially limits the generalisability of the data although a pilot anaesthetic programme was proposed and E-mentors recruited towards the end of this study. Whether E-mentoring could work for other trainees in other specialities or General Practice is unclear. It is disappointing that no information could be gained from the non-responders in the study who often provide very useful advice about the pitfalls. It would have been useful to assess the pre and post programme expectations as well as E-mentees pre-existing knowledge of mentoring. 8
There was always a risk that issues would be identified that required more support than an asynchronous remote process could provide. In the pilot study, three E-mentees were offered additional telephone support and advice as they dealt with very challenging work related issues. These three found ongoing email support to be sufficient however. None of the E-mentees required such support within the study.
Positive feedback from E-mentees was associated with more frequent email contacts with their E-mentors. They appeared to engage with the process and kept their E-mentor up to date with progress on specific areas. It may be that E-mentees need to be shown a model of how to act within a mentoring relationship- including how to identify problems, what can be done about them and how to communicate by email about these issues. Surgeons as a speciality are not well known for expressing their feelings—either because of being to busy to stop and reflect, unused to admitting challenging issues or complications or concerned about losing face by revealing confidence issues or stresses.
Surgical E-mentoring involved ST1 to 3 trainees and so might not be generalisable to more junior or senior surgical grades. Requiring email contact probably self selects the outgoing, forward looking group of trainees whereas perhaps those that needed E-mentoring the most in surgery are the non-responders? There is no way of ensuring an email response (compared with asking someone to attend a face to face meeting) but with educational support being of good quality in the National Health Service (NHS), hopefully those with difficulties were getting adequate support through the usual work based mechanisms.
This E-mentoring process was separate from clinical or educational supervision. These two latter roles focus on day to day training needs and the assessments linked with those needs and the curriculum. Therefore, E-mentoring dovetailed with good supervision would hopefully see academic knowledge, clinical management and operative skills training being improved.
This study is indebted to all the E-mentors who volunteered to help. All worked in busy, senior surgical training jobs (or as consultants) but gave their support, guidance and experience gladly. It is most unusual for any mentoring programme to have a considerable surplus of E-mentors. The trend of reducing contact with E-mentors and reducing questionnaire completion meant that at the planned year review point, the study was closed rather than expanded although ongoing contact was strongly encouraged within each mentoring relationship.
Every attempt was made to improve the relationship of each mentor:mentee partnership. We had hoped to run a face-to-face induction session having learnt from the pilot study. A lack of resources and the complexities of getting doctors on shift patterns to meet proved to be over optimistic, although it is now the belief of the author that at least one initial face to face meeting is essential if the mentoring pair have not met previously.
Is What We Have Done Mentoring or Not?
What I have not done is identified one specific problem per occasion to focus on and deal with from start to end. The most widely quoted mentoring process is the “Skilled Helper Model” by Egan which takes a mentees story, ensures it is the whole story, works out the options for change and finally helps the E-mentee construct a realistic process for achieving that plan. 16 Previous studies have discussed the need for regular contact (ie, more frequent than alternate monthly) and maybe it was therefore wise to discuss more than one topic, otherwise less would have been achieved. As the coordinator, I encouraged each mentor to listen, challenge, reflect and support. Within each E-mentoring relationship, they have discussed many issues, constructively challenged all aspects of surgical training and encouraged their E-mentee to reflect on their current practice and look forward in their careers. Personally, I believe, we have undertaken what any face-to-face mentoring programme would have done; and hopefully achieved just as much.
The Mentoring Network Construct
Professor Garvey has undertaken extensive research on the mentoring process and considered the mentoring relationship that develops during a one-to-one, face-to-face process.17–20 The people involved already knew each other and interacted in the workplace. The responsibility for managing the relationship was mainly “shared” (46%) or “driven by the mentee” (46%). Figure 6 displays Professor Garvey's norm model for face-to-face mentoring dimensions.

Face-to-face mentoring dimensions “Norm” model.
On reflection, the relationship in this E-mentoring pilot was 100% driven by the mentor (“I will make contact every other month”) whereas a more informal, E-mentee focussed methodology might have altered the dynamics and potential gains. I suspect that with such busy jobs however, contact from the E-mentor would still have been necessary for the majority. Figures 7 and 8 respectively display the E-mentoring coordinators ideal E-mentoring dimensions at study commencement and the perceived dimensions at study conclusion.
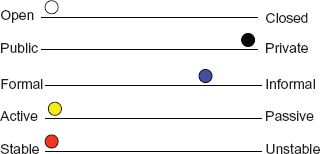
E-mentoring dimensions: E-mentoring coordinators view at study commencement.

E-mentoring dimensions: E-mentoring coordinators reflection at study cessation.
Open versus closed; public versus private
The study was always set up to be a private mentoring relationship and it remained so throughout. Each letter was individually typed and posted, no group emails were sent and all communications took place directly between E-mentor and each E-mentee. Any future expansion of the E-mentoring role might benefit from a more public face.
Formal versus informal
Although E-mentoring could not hope to reproduce a “pop in at any time” culture, I had hoped that the E-mentoring questionnaires would simply form a backbone on which to construct informal but regular flows of discussion. I sensed that for some the process became an alternate monthly “signing in and out” rather than a spontaneous sharing of experiences and reflections, although the results of the questionnaire do not clearly concur with that view.
Active vs. passive (one or both parties)
As the E-mentor coordinator and subsequent author, I had a vested interest in the process so my position and involvement was active. The majority of E-mentees were active at the start of the process but lost way towards the end whether due to questionnaire fatigue or because they felt the process had provided all it could for them.
Stable vs. unstable (ie, agree to the ground-rules and stick to them)
There were few ground-rules formally set at the beginning. There did not appear to be any obvious “boundary crossed” that made either the E-mentee or E-mentors feel uncomfortable. I would have been very keen for more contact between these busy groups of professionals. Future instructions to E-mentors would reinforce the need for constructive challenge, the need to review the issues from previous contacts, to follow particular discussions and plans through to their conclusion and to encourage E-mentees to make regular contact.
How Frequent?
Successful mentoring involves frequent and regular interaction but all sorts of barriers such as time, work responsibilities, geographical distance and lack of trust reduce, if not halt, interaction. 21 This study shows that alternate monthly contact can still be of benefit to E-mentees, with experiences at work accruing through the time period and the E-mentee having time to reflect on their experiences and development. Ultimately, the frequency of discussions should be a decision reached following mentor: mentee discussions. Issues of confidentiality, availability, timescale, expectations and limitations, role conflict and self-management are also crucial in establishing the mentoring boundaries.3,22
Was E-mentoring Useful?
It was encouraging that most E-mentees felt the process was a positive experience and that it encouraged reflection and provided support for instance. It is clear that mentoring should not be used as the primary training and assessment tool as a geographically remote mentor can not review a trainee's clinical knowledge or operative skills.
Interestingly, the discussions did not seemingly improve the work/life balance nor was it useful in changing the bad points in the job that had been identified. I suspect that reason for this was three fold:
Once the problem was identified, the E-mentor did not focus enough on this issue, discuss mechanisms of change or ask for feedback on the situation at subsequent mentoring contacts
It was probably not made clear that the E-mentee would be the key mover in change and that the mentor was there to support them through their transition rather than to drive it or arrange it
Being geographically distant, not having direct responsibility for their training or position and not having an official role in their training (eg, Royal College of Surgeons approved) meant that there was a limit to the amount of networking and negotiating that could be achieved on their behalf.
These areas of potential weakness would need to be clearly stated in future information booklets and at induction.
The Future of Surgical Training
Linda de Cossart and Della Fish in their book “Cultivating a Thinking Surgeon” consider the training of young surgeons in new ways, using reflection and increasing support mechanisms. 4 However, there will always be those who will challenge whether mentoring can improve surgical training. Surgery involves such a mix of practical and knowledge skills but the recognition of the non-technical aspects is very topical in the current surgical and educational literature. Barnett believed successful mentoring led to effective learning achieved through reflection, development of problem solving skills and a gradual movement of the mentee from being a novice, dependent problem solver to an autonomous, expert problem solver—a useful skill for surgeons with difficult clinical diagnoses or complex operative decisions to make. 23 If we are to train surgeons effectively, in a shorter period of time, then we must consider all aspects of their development to bring about an accelerated learning pathway; E-mentoring is, I believe, one area that should be considered.
The E-mentee is Crucial
Having reviewed all the feedback questionnaires, it has re-affirmed the importance of the E-mentee within the process. Those that engaged in E-mentoring appeared to gain and enjoy the process the most. Their feedback as listed in the tables was astute and helpful and will undoubtedly improve future E-mentoring processes.
Conclusions
This study shows that E-mentoring is beneficial to surgical trainees who are engaged in the process. It is technically feasible even when expanded to a training region with multiple trainees and mentors. No funding was needed but a great deal of good will on the part of enthusiastic surgical E-mentors was required. The process encourages reflection and was a useful source of advice but there remains areas where its scope is limited.
Surgical educators recognise that future surgical education should utilise reflection and increase support mechanisms to optimise training experiences. E-mentoring does this and could help enhance and potentially accelerate it. Whether email based mentoring support could be supplemented and enhanced by intermittent face-to-face, phone or web-based forums are interesting areas for future research.
Author Contributions
Conceived and designed the experiments: DALM. Analysed the data: DALM. Wrote the first draft of the manuscript: DALM. Contributed to the writing of the manuscript: DALM. Agree with manuscript results and conclusions: DALM. Jointly developed the structure and arguments for the paper: DALM. Made critical revisions and approved final version: DALM. All authors reviewed and approved of the final manuscript.
Competing Interests
Author(s) disclose no potential conflicts of interest.
Funding
Author(s) disclose no funding sources.
Abbreviations
EWTD, European Working Time Directive; MMC, Modernising Medical Careers; NHS, National Health Service; SHO, Senior House Officer; UK, United Kingdom.
Disclosures and Ethics
As a requirement of publication author(s) have provided to the publisher signed confirmation of compliance with legal and ethical obligations including but not limited to the following: authorship and contributorship, conflicts of interest, privacy and confidentiality and (where applicable) protection of human and animal research subjects. The authors have read and confirmed their agreement with the ICMJE authorship and conflict of interest criteria. The authors have also confirmed that this article is unique and not under consideration or published in any other publication, and that they have permission from rights holders to reproduce any copyrighted material. Any disclosures are made in this section. The external blind peer reviewers report no conflicts of interest.
Footnotes
Acknowledgements
Professor Bob Garvey (St Johns York University) for previous assistance and agreement to compare and adapt his original figures.