
Abstract
Background
Although, health status of Bangladeshis has improved, levels of child mortality in Bangladesh remain unacceptably high. This paper reviews household wealth inequalities in immunization coverage in Bangladesh. The objective of the study is to examine how household wealth status and socio-demographic characteristics relate to immunization status of children.
Methods
Using data from the 2004 Bangladesh Demographic and Health Survey (BDHS), this paper investigated the inequalities and implications of infant immunization coverage in Bangladesh. To prepare the proxy variable of household wealth status we applied principal component analysis (PCA) technique based on variables such as assets, utilities and services available at household level. And then scores of the proxy variable was transferred into quintiles.
Results
The difference in immunization status between the richest and the poorest quintiles was significant (crude OR 5.2, p < 0.001). The addition of education to the multivariate model lowered the impact of wealth index by almost half. Increasing education levels were positively associated with achieving full vaccination status. Sex of children and age of mothers were not associated with the child's immunization status.
Conclusions
Despite free immunizations, use is not uniform throughout the population. Access to wealth and education may contribute to disparities in achieving full immunization. Minimizing indirect costs of immunizations may reduce disparities. Health education needs to be intensified for parents with minimal education.
Introduction
The international development community has prioritized improving health outcomes among the world's poor (Labonte et al. 2005) and the millennium development goals (MDGs) have been set as major milestones to achieve this (UN Web, 2005). Gaps in child mortality between rich and poor countries are unacceptably wide and in some areas are becoming wider (Victora et al. 2003). Immunization status is one indicator of progress towards the child health targets established under the Millennium Development Goals (Chowdhury et al. 2003). However, reducing child mortality and achieving the millennium development goal for child survival depends on whether effective and sustainable interventions can be delivered to high proportions of children and mothers (Bryce et al. 2003).
The World Development Report 2004 revealed that health outcomes are consistently worse among the disadvantaged. For example, in low and middle-income countries, under-five mortality rates are 2.3 times higher among the poorest fifth than among the richest fifth (World dev. Report, 2004). Inequalities in health reflect the influence of a number of socio-economic factors at the individual, household and community levels. These existing differentials in health status and health service utilization are generally seen as unnecessary, needless and unfair (Debpuur et al. 2005).
One study that reviewed the inequities in health in Bangladesh (Sen, 2001) commented: “Although the country has achieved some progress in reducing fertility, mortality and malnutrition in the past decade–– as measured by the aggregate trends at the national level––the gap between the poor and the non-poor (however measured) in respect to health indicators remains extraordinarily and unacceptably high”.
Although the health status of Bangladeshis has improved, levels of child mortality are high at 88 deaths per 1000 live births. The national figures conceal substantial differentials in health status among subgroups of the population. Under-5 mortality rates for instance, range from 72 in the richest quintile to 121 in the poorest quintile (BDHS, 2004). Immunization against the six childhood killer diseases (tuberculosis, diphtheria, pertussis [whooping cough], tetanus, polio, and measles) is one of the most effective ways of protecting children against infection and subsequent death (EPI CES, 2005). Longitudinal data on mortality and measles immunization from Bangladesh demonstrate that vaccination reduces mortality risk most among vulnerable children (in terms of socio-economic status) (Koenig et al. 2001). This indicates vaccination coverage is a marker of health service utilization.
This paper investigated the existence of health inequalities in Bangladesh by examining the relationship between household wealth characteristics and immunization coverage. Specifically the study aims to examine the relationship between indicators of household wealth status (HWS) and household demographics, and immunization.
Methods
The Bangladesh Demographic and Health Survey (BDHS) 2004 is the fourth survey of this type conducted in Bangladesh. Fieldwork commenced on January 1, 2004 and was completed on May 25, 2004. The 2004 BDHS survey was conducted under the authority of the National Institute for Population Research and Training (NIPORT) of the Ministry of Health and Family Welfare of the Government of Bangladesh. ORC Macro of Calverton, Maryland, provided technical assistance to the project as part of its international demographic and health surveys (DHS) program, and financial assistance was provided by the U.S. Agency for International Development (USAID)/Bangladesh.
The 2004 BDHS sample is a stratified, multistage cluster sample consisting of 361 primary sampling units, 122 in urban areas and 239 in rural areas. Details of the methodology used to conduct the BDHS have been described elsewhere (BDHS, 2004). We secured permission for analysis of the BDHS 2004 data from ORC Macro in 2006 (www.measuredhs.com). The data file consists of 11,440 eligible women from 10,500 households. It includes information on background characteristics (age, education, religion, etc.); variables of assets, utilities and services (a variable of household wealth status was prepared based on report of households ownership of radio, bi-cycle, motor cycle, television, wardrobe, table, chair/bench, watch or clock, cot or bed, sewing machine, owns any homestead, owns any land, hygienic latrine, type of floor-wall-roof material and access to water, electricity, cooking fuel) available at household level; reproductive history; family planning use; antenatal care, postnatal care; breastfeeding and weaning practices; vaccination and health of children under the age of five; marital status; fertility preferences; and causes of death of children under age five. These 10,500 households had complete data of household asset ownership, housing conditions, and water and sanitation variables, sufficient to create a household wealth index. This wealth index is used as a measure of household wealth status hereafter.
The analysis of immunization was limited to the last/latest reported birth by mothers and so the analysis of immunization included all currently living children aged 12–23 months at interview (born between, 2002–2003); immunization status was not recorded for dead children. This age group was included because according to WHO recommendations, children should be fully vaccinated by the end of the first year of life and this is the standard of assessing immunization coverage.
Vaccination is used in this paper as a proxy for health service utilization. The key explanatory variable considered for the study was household wealth status. Other variables such as sex of the child, maternal age, parental education, number of living children in the household, and location of residence are considered as control variables. Household socio-economic status was measured using a household wealth index as described by Filmer and Pritchett (1998) (Filmer and Pritchett, 1998) and used by others (Wagstaff and Watanbe, 1999; Gwatkin et al. 2000; Gwatkin, 2000; Vyas and Kumaranayake, 2006). However, this approach to measuring household socio-economic status is largely dependent on household durable asset ownership, access to utilities and infrastructure (e.g. sanitation facility and source of water), and housing characteristics (e.g. number of rooms for sleeping and building materials).
The data were analyzed using SPSS (version 11.5) software. Principal component analysis (PCA) was applied to the household data to develop a wealth index as a proxy for household wealth status. Variables included in the PCA were household assets ownership, housing conditions, access to utilities and services. Simple cross-tabulations and multivariate approaches were used to examine the relationship between household wealth strata and full immunization status. As an initial step we used cross-tabulations to explore the existence and magnitude of health inequalities. Regular chi-square tests were performed to assess the significance of these disparities. We used adjusted odds ratios to indicate wealth inequalities in immunization coverage. The variables found not significantly associated with full immunization coverage, were not included in the model of adjusted odds ratios.
In the BDHS survey, vaccination status was determined using the child's vaccination card or mother's statement or both. For the purposes of this analysis we used three measures to describe the vaccination status of children: “never vaccinated” to indicate that a child received none of the four vaccines (BCG, DPT, OPV and Measles); “partially vaccinated” to indicate that a child received at least one complete dose of either BCG, DPT, OPV or Measles, but did not receive all recommended doses of all four vaccines; and “fully vaccinated” to indicate that a child received all recommended doses of all four vaccines.
Results
The 11,440 eligible mothers reported 1,222 living children aged 12–23 months among their last births. A description of the children included in the analysis is provided in Table 1. Overall 6.2% of children aged 12–23 months had never been vaccinated, 21.0% children had been partially vaccinated and 72.7% children had been fully vaccinated. Based on the household wealth index, the highest (26%) portion of children belonged to the poorest quintile; while the lowest proportion (16%) was in the richest quintile. The male-to-female ratio of children in this age group was 47:53. The majority (70%) of mothers of these children were aged 20–34 years. In terms of education, the highest percentage (23%) of parents had no education. Thirty nine percent (39%) of mothers had three or more living children. The majority (80%) of mothers resided in rural areas.
Immunization status of children aged 12–23 months and demographic and socioeconomic characteristics of their households in Bangladesh.

Strong household wealth differences in vaccination coverage among children were found (p < 0.001) with immunization coverage positively related to wealth. Children in the poorest quintile were least likely to have been fully vaccinated (the richest/poorest ratio was 1.56) compared to other quintiles and the percentage of children never vaccinated and partially vaccinated was highest among children in the poorest quintile (Table 2).
Immunization status by household wealth status and demographic characteristics in Bangladesh.
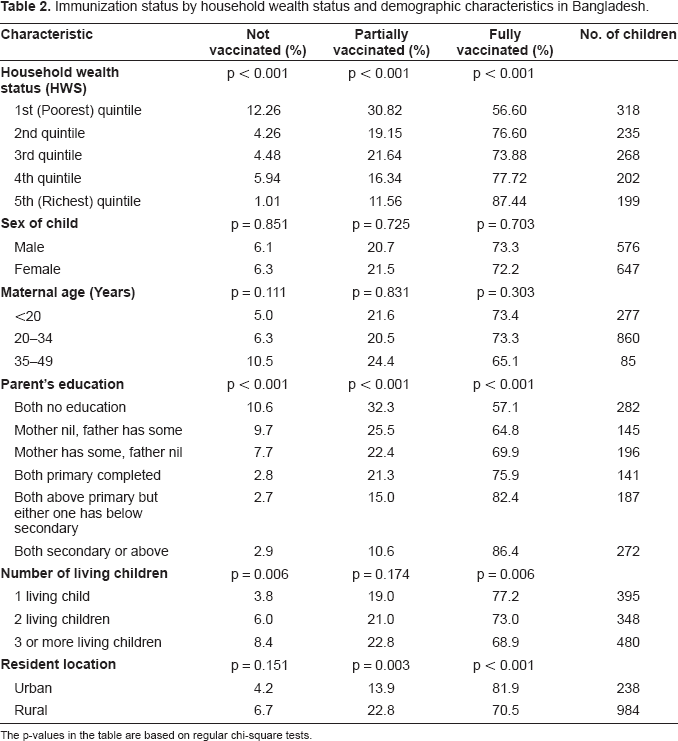
The p-values in the table are based on regular chi-square tests.
While 12% of children in the poorest quintile had never been vaccinated, this was true for only 1% in the richest quintile (Table 2). In addition, the rate of full vaccination was highest (87%) among children in the richest quintile compared to any other quintile. A chi-square test for trend showed a significant difference between the poor and the rich in terms of vaccination coverage as a whole in Bangladesh.
Neither sex of the child nor maternal age was significantly related to vaccination coverage. However, parental education was strongly related to children's immunization status. Children whose parents had better education were more likely to be vaccinated than children whose parents had no education. In particular, children whose mothers had more education also had higher level of immunization coverage (Table 2).
The number of living children was negatively associated with full immunization, as because the number of living children for a mother or in a household increased, the rate of fully immunization coverage decreased (p = 0.006). Full immunization for children in urban areas was significantly better than in rural areas (p < 0.001).
At an early stage of data analysis we checked the possible interacted effects between independent variables and found that education of both mother and father of the children were inter-related. We merged education of mother and father into one variable and named as parent's education to avoid such interactions or multicollinearity. Multivariate analysis was performed to assess the relationship between explanatory variables and full vaccination. Table 3 presents adjusted odds ratios for full vaccination for wealth quintiles adjusted for parental education, number of living children and location of residence. Consistent with the results of the univariate analysis, the odds ratios for full vaccination significantly increased with wealth. For example, a child in the richest quintile was five (5) times more likely to have been fully vaccinated compared to a child in the poorest quintile (unadjusted, logistic model-I). After controlling for education, children in the richest quintile were still almost three times (OR 2.9) more likely to have been fully vaccinated compared to the poorest quintile (adjusted, logistic model-II).
Logistic Regression: Odds ratios of the likelihood of full vaccination for household wealth score quintiles and other associated variables in Bangladesh.
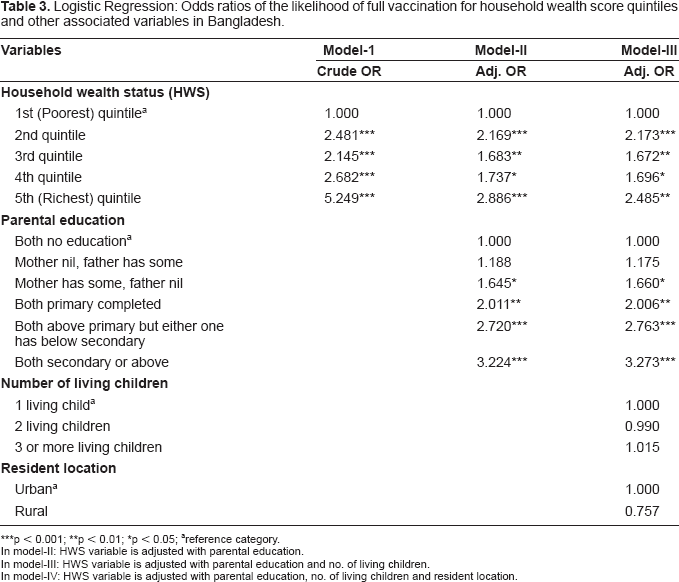
p < 0.001;
p < 0.01;
p < 0.05;
reference category.
In model-II: HWS variable is adjusted with parental education.
In model-III: HWS variable is adjusted with parental education and no. of living children.
In model-IV: HWS variable is adjusted with parental education, no. of living children and resident location.
Addition of the variables “number of living children” and “location of residence” to the multivariate model (Model III) made little difference in the relationship between wealth and full vaccination; the association between wealth and full vaccination remained significant, with an odds ratio of 2.4 after controlling for these variables.
Discussion
Inequalities in immunization that favor the relatively wealthy are worrisome. In Bangladesh, childhood immunizations are free, which should minimize wealth-related barriers to access. However, as the results of our analysis suggest, wealth remains an important factor in access to full vaccination of Bangladeshi children. One possible explanation is that poverty prone people prioritize spending time on income earning opportunities rather than on accessing preventive health services, such as immunization (EPI CES 2005). Other possible explanation for the wealth-related disparities in achieving full vaccination status may be found in the health seeking attitudes and practices of poor households and ignorance about vaccination associated with the people those are difficult to reach (i.e. who live at great distance from an immunization center) (EPI CES 2005). It may also be the case that indirect costs, such as those accrued for travel to immunization centers or time lost from income-generating activities, make it difficult for poorer households to avail themselves of services that exist in the community, regardless of cost. In fact these are all the critical factors which have similarity with other findings as it says that poverty and marginalization are considered the major causes of inequalities in health (Evans et al. 2001). To minimize all associated factors as discussed above, besides all other efforts, initiation of mobile vaccination clinics particularly for difficult to reach areas might help to increase the overall coverage rate.
The indices of HWS (household wealth status) evidenced of clumping and truncation hindered ability to accurately classify wealth quintile borderline households (data not shown). Clumping may be a statistical pnenomenon caused by a lack of input variables that can adequately distinguish between households with a similar HWS, or it may be a product of social and economic homogeneity stalking from the long time because of sociopolitical strategy in Bangladesh. Including variables to PCA such as differentiation between quality of assets, owning any mobile phone, involvement in micro credit program activities may have helped reducing the effect of clumping and/or truncation and might be explored in greater detail, though studies imply that this information may not add to the accuracy or robustness of the index (Hewe, 2008).
Better immunization coverage among relatively better off households may suggest that such households are better able to absorb the indirect costs of getting children immunized. In this regard, efforts to minimize the indirect costs of immunizations (especially to poorer households) may go some way to reduce the inequalities in service utilization.
Although education was found to be independently associated with immunization coverage, to some extent it also attenuated the association with wealth. This is likely because low income is associated with both lower levels of education and with access to immunization (Victora et al. 2003). The independent effect of education may be related to increased knowledge or awareness of existing programs.
The sex of child could be a risk factor as observed in some societies with strong cultural preferences for males (Thein and Goh, 1991). EPI Survey 2005 revealed that in terms of valid coverage rates in Bangladesh, 62 percent of the female children were found fully vaccinated, as compared to 65 percent male children (EPI CES 2005). But our study revealed no significant gender differences in full vaccination. This is likely because people might have good awareness against gender discrimination or gender preference. Also, as like the 2005 EPI Survey, immunization coverage was lower in rural areas, however this different was not significant. This somewhat lower rate of immunization may result from difficulties in providing services to select populations in hard-to-reach areas.
Rates of full immunization have improved from 1996–1997, when coverage was 56 percent to 73 percent in 2004 (Barkat and Majid, 2003; BDHS, 2004). However, the 2004 data show that the goal of fully immunizing at least 80 percent of children has not yet been reached in Bangladesh. In order to reach the targeted coverage, it is critical to decrease disparities as the results of this paper evidenced.
Conflict of Interest
No conflict of interest to declare.
Footnotes
Acknowledgement
We cordially acknowledge MEASURE DHS, Macro International Inc., 11785 Beltsville Drive, Suite 300, Calverton, MD 20705, U.S.A. for giving us access to their database. The study has no involvement of any sponsor.