
Abstract
Childhood asthma is highly prevalent, affecting approximately nine million children in the United States. Negative effects of pediatric asthma are disproportionately experienced by ethnic minorities living in low-income, urban settings. Given the great diversity in families' ways of addressing children's asthma symptoms, sociocultural factors underlying asthma disparities must be examined. The current study investigated associations among parents' beliefs about conventional and holistic/alternative medications, parents' religious problem-solving strategies and childrens' risks for asthma treatment nonadherence. The sample included 66 parents of ethnically diverse children with asthma living in urban settings. Factor analysis of the Religious Problem Solving Questionnaire yielded two factors, self-directed (ie, solving problems independently of God) and God-involved problem solving. Parents' strong positive beliefs about conventional and alternative medications were associated with greater self-directed problem solving and with more risks for nonadherence. Higher levels of self-directed problem solving also were associated with more risks for nonadherence. Self-directed problem solving mediated the associations of conventional and alternative medication beliefs with risks for nonadherence. Possible explanations for these findings are discussed.
Introduction
Asthma is among the most prevalent childhood illnesses in the United States. 1 Children from urban, minority, and low-income backgrounds are disproportionately affected by asthma, with African American and Hispanic children experiencing the highest rates of asthma prevalence, morbidity, and mortality. 2 The National Heart, Lung and Blood (NHLBI) Workshop Report on reducing asthma health disparities stressed that social class, education, and minority status interact and influence asthma prevalence. Thus, it is crucial for health care researchers and providers to be aware of patients' culture-related beliefs and practices in order to reduce disparities and promote health and wellness. Parental beliefs about medications may impact families' use of specific disease management strategies, including complementary and alternative medications (CAM) and religiously-informed approaches. These strategy choices may in turn affect the physical and psychosocial functioning of children with asthma.3,4
The health belief model
According to the Health Belief Model, attitudes and beliefs are integral determinants of health behavior change 5 and affect an individual's health-related actions. 6 A person's health-related decisions are influenced by perceptual factors such as susceptibility to illness, severity of the illness, efficacy or control in treating the illness, and barriers to intervention. 7 This model has also been adapted for pediatric populations and now includes other determinants of health behavior change, such as various socioeconomic and environmental factors that impact health decisions. 8
Parents' beliefs about CAM in pediatric asthma management
Parents' beliefs appear to have a direct and indirect influence on children's beliefs and self-management actions, particularly when the child is under the age of 11.9,10 Parents' beliefs can have a profound effect on clinical care by either facilitating or impeding prescribed treatments or promoting the use of strategies that have not been recommended by health care professionals. 11 Negative parental beliefs about conventional medications may serve as barriers to care and have been associated with poor medication adherence and increased asthma morbidity in children.4,12
Over recent years more research has been conducted examining the association between parents' beliefs and perceptions of asthma and children's asthma related outcomes.12–15 Evidence suggests that parents' beliefs about asthma are a risk factor for suboptimal asthma management, specifically poor adherence to the prescribed asthma treatment regimen. For instance, in a sample of African-American families, Mansour and colleagues 14 found that parents' health beliefs and perceptions about medications were at the core of many barriers to optimal care, specifically medication adherence. Parents who had worries and concerns about the use, safety and long-term complications of medication use were likely to modify their children's asthma treatment plan. 14 Additionally, in a Latino sample, beliefs about asthma practices were informed by one's cultural traditions and origins. Puerto Rican and Dominican caregivers reporting that remedies, home treatments and manipulative body-based practices were effective interventions for asthma. 15 Furthermore, McQuaid and colleagues (2009) reported that caregiver's beliefs in the necessity of medications were important factors in medication underuse. 16
In some literature, beliefs about holistic health and beliefs about CAM are considered as separate constructs that may uniquely impact functional outcomes. Strong beliefs about CAM have been associated with a general dissatisfaction with the ability of conventional medications to adequately treat chronic illness. 17 No firm conclusions have been drawn regarding whether strong beliefs about CAM predict actual CAM use. 18 Strong beliefs about holistic health have been associated with a broader sense that multiple factors, such as nutrition, emotions, religion and lifestyle choices, affect health. 17 Strong alternative/holistic health beliefs have been found to be an important factor in the decision to actively use alternative treatment strategies. 19 Although holistic and CAM belief systems have been shown to be distinct, it has been concluded that that both constructs can be combined to validly measure a person's attitude about nonmedicalized strategies to treat illness. 17
Parents' use of religious CAM in pediatric asthma management
Religion and spirituality are often considered CAM strategies classified under the category of mind-body interventions. However, many theorists debate that religion and spirituality are separate and distinct constructs from other mind-body strategies. 20 Religion and spirituality have been documented as the most used type of CAM among adults. Moreover, when religion and spirituality are included in the definition of CAM, the frequency of CAM use among individuals rises. 21 Religion and spirituality may also impact physical health through encouraging behaviors that reduce risks (eg, avoiding smoking and drug use). Therefore, religiously- and spiritually-based approaches to illness management and healing deserve special attention in the research on CAM.
Religious orientation in parents' problem-solving
Adults' use of religious coping is an important factor in the management of their physical and mental health, 22 and thus it also may influence how parents manage children's asthma. Parents of children with asthma must respond to children's symptom exacerbations, sleep disruption, activity restrictions and school absences, as well as manage asthma treatment. Families from urban, minority, and low-income backgrounds may be burdened by cumulative stressors such as economic strain, environmental hazards, discrimination, or substandard housing. In this context, parents' coping resources and problem solving approaches are likely to affect how well children's asthma is kept under control. As such, it is important to assess the role that religious coping and/or problem solving serves in the process of illness management.
The construct of religious problem solving refers to religiously-informed efforts to solve stressful situations in one's life. Religious problem solving is a multidimensional process including cognitive appraisals of the triggering event, the desired outcome, and the methods necessary to achieve the outcome. 23 Pargament and colleagues 24 conceptualized religious problem-solving on a continuum of beliefs regarding God's involvement in solving human problems. On one end of the continuum, solving problems is the active and direct responsibility of individuals themselves, and on the other end, individuals play a passive role to God in solving problems. Three religious problem solving orientations were revealed in Pargament and colleagues' original sample, primarily comprised of white, church-going, Midwestern adults. The self-directed problem solving orientation reflected the belief that God allows individuals free will to direct their own lives. This orientation was associated with a quest orientation to religion (ie, a willingness to question existential ideas), as well as higher personal control, increased self-esteem and better mental health status.22,24 The collaborative problem solving orientation referred to a combination of reliance on God and individual agency to solve problems. It was associated with an internalized form of religiousness characterized by a highly involved relationship with God. The deferring problem-solving orientation reflected full reliance on God to solve problems with little no individual agency. It was associated with high religious involvement and reliance on external rules. 24 It has been unclear if these problem-solving orientations characterize the experiences of adults with other demographic profiles and/or coping with specific stressors such as chronic illness.
The current study
The specific aim of the study was to conduct preliminary analyses exploring parents' problem-solving orientations, particularly with regard to the perceived role of God in solving problems, in a socioculturally diverse sample. In this model, two types of religious problem-solving (ie, self-directed and God- involved) serve as mediators between the predictor variables, beliefs about conventional and alternative medications, and the outcome variable, risks for nonadherence. Please see Figure 1.

Self-directed and god-Involved problem solving as mediators between beliefs about conventional medications and risks for nonadherence (Model 1) and beliefs about alternative medications and risks for nonadherence (Model 2).
Method
Design, recruitment and study participants
Data presented here are part of a larger study conducted in 2005 investigating complementary and alternative medication use in minority children with asthma. 26 Approval for this study was provided by the University of Massachusetts Boston Institutional Review Board. It is important to note that all participants that completed the larger study were included in the present analysis. Primary caregivers of 3–17-year-old children with physician-diagnosed asthma were recruited from three community health centers in a large northeastern city. Primary caregivers utilizing these health centers are of diverse ethnic and racial backgrounds.
Due to budgetary and logistical factors associated with data recruitment, recruitment for this study began at one local health center. A mailing list was generated of primary caregivers of 3–17 year-old children served by the center who have been diagnosed with asthma. Questionnaire packets containing the following materials in English and Spanish were sent directly from the health center to families meeting inclusion criteria: 1) A description of the study; 2) A UMass Boston Institutional Review Board approved consent form; 3) A questionnaire packet of study measures; and 4) A self-addressed, pre-stamped envelope to return the questionnaire packet. The questionnaire packet took approximately 20 minutes to complete. The questionnaire packets were translated into Spanish using forward and backward translation, followed by a consensus group. A statement was included offering for the questionnaire packets to be read over the phone in order to cater to participants who may require assistance. After signing the consent form and returning the questionnaire packet, participants were sent a $15 gift card to either Target, Walmart, or Stop and Shop as compensation for their time. Participants were also entered into a raffle for a gift basket. Out of the 176 packets mailed to potential participants, only 12 families responded. Given the low participant response from this recruitment method, additional recruitment methods were employed.
Remaining participants were recruited directly by research assistants in the pediatric health center waiting rooms and completed the questionnaire packet while they waited for their child's appointment (n = 60). All research assistants were trained by the Principal Investigator in proper consent and administration techniques. Research assistants were also instructed to offer to administer the questionnaires to participants in case they were uncomfortable or unable to read the packet. However, the majority of questionnaire packets were self-administered by parents as they waited for their child's medical appointment. Of the research packets that were collected, six questionnaire packets were omitted from analyses for a variety of reasons (eg, the child was not diagnosed with asthma, caregivers participated in the protocol twice, and an adolescent completed the questionnaire packet). The final sample size totaled 66 participants. Of the approximately 500 families who were approached for participation in the study, the response rate was 13%.
Six questionnaire packets were omitted from the analyses for a variety of reasons (eg, the child was not diagnosed with asthma, caregivers participated in the protocol twice, and an adolescent completed the research packet). The final sample totaled 66 participants.
Study instrument and measures
A demographic questionnaire assessed characteristics of the child's family and household. Medical chart reviews were conducted to determine children's most recent physician-rated asthma severity level. Additionally, the following measures were used to assess primary study variables.
Parents' conventional medication beliefs
The Asthma Beliefs Scale (ABS) 28 was administered to parents to assess beliefs about their children's physician-prescribed asthma medications. Developed for parents of 2–12 year-old inner-city children with asthma, it contains 19 items that comprise three subscales: Self-efficacy (ie, positive attitudes toward preventive care); Symptom Based Outcome Expectancy (ie, confidence in managing asthma attacks); and Worries and Concerns (ie, concerns about medication side effects). 29 A sample item is: “It is difficult for me to help my child take asthma medications exactly the way the doctor said to”. Parents responded on 5-point scale (strongly agree to strongly disagree) with higher scores reflecting more positive beliefs about conventional medications. Adequate internal consistency has been reported for the scale (alpha = 0.72). 29 Internal consistency in this sample was low (alpha = 0.56).
Parents' alternative medication beliefs
The 11-item Holistic Complementary and Alternative Health Questionnaire (HCAMQ), 17 which assesses healthcare provider attitudes to CAM and holistic health beliefs, was modified for use with parents. Wording changes were made to assess for asthma-and child-specific factors associated with CAM use. The HCAMQ includes two subscales: CAM beliefs and holistic health beliefs. The authors reported that given the hierarchical structure of the HCAMQ, the subscales can be combined to create a total score, which was used in the current study. Participants responded on a 6-point scale (strongly agree to strongly disagree) with higher scores reflecting more positive beliefs about CAM/holistic health. Sample items are: “Alternative medicine (eg, herbs, acupuncture) should go through more scientific testing before it can be accepted by medical doctors” and “ Alternative medicine (eg, home remedies) should only be used as a last resort when conventional medicine has nothing to offer”. Good internal consistency has been reported for the scale (alpha = 0.86). 30 Internal consistency in this sample was good (alpha = 0.80). For conciseness, this variable will be referred to as “alternative medication beliefs” although it represents both holistic health beliefs and beliefs in CAM.
Parents' religious problem-solving orientation
A modified version of the short form of the Religious Problem-Solving Scale (RPS) 24 was used to assess primary caregivers' beliefs regarding the responsibility of God versus self in the problem-solving process. Primary caregivers responded to 18 items using a 5-point scale (never to always). Items are presented in Table 1. Responses are broken down into three 6-item subscales reflecting self-directed, collaborative, and deferring religious problem-solving orientations. Pargament and colleagues (1988) reported high reliability and internal consistency for the long form and short form of the RPS, as well as normative data for each subscale, as follows: self-directed (M = 29.7, SD = 10.7), collaborative (M = 36.0, SD = 10.7), and deferring (M = 25.8, SD = 9.2). Subjects from the normative sample included 179 Midwestern church members. The subjects were exclusively white, had an average age of 46 years old, and 69% were married. In the current sample of minority parents from urban neighborhoods, internal consistency was 0.87.
Factor loadings of religious problem-solving items.

Pargament, Kennell, Hathaway, Grevengoed, Newman, and Jones, 1988.
Risks for asthma treatment nonadherence
The Risks for Nonadherence Scale is a parent-report measure including 12 factors that have been associated with failure to comply with physician- prescribed asthma treatment protocols. 31 Higher scores have been significantly associated with measures of asthma morbidity. 32 This measure does not require parents to admit nonadherence, which may decrease social desirability bias. Sample factors are: “ multiple asthma caregivers (caregiver plus 3 others)” and “you have trouble getting a doctor's appointment for your child”. Primary caregivers endorsed either ‘Yes’ or ‘No’ for a given risk factor. A summary score of positively endorsed items was calculated with scores ranging from 0–12. Internal consistency in this sample was adequate at alpha = 0.66.
Data analysis
Descriptive analyses using SPSS 16.0 were generated to explore demographic characteristics of the sample. In all analyses, a P-value of less than 0.05 was considered significant. Pearson product-moment correlational analyses, t-tests and ANOVA's were conducted to examine the association between demographic/ descriptive, predictor and outcome variables. Hierarchical multiple regression analyses were used to assess multivariate associations among primary study variables. To test mediation, a series of hierarchical regression analyses was conducted as outlined by Baron and Kenny. 25 First, associations were tested between the predictor variables (conventional and alternative medication beliefs) and the outcome variable (risks for asthma treatment nonadherence), between the predictor variables and the hypothesized mediating variable (parents' problem-solving orientation), and between the mediator and the outcome. A mediating effect is demonstrated if the magnitude of the relationship between the predictor and outcome is no longer significant (complete mediation) or weakened (partial mediation) when the mediator is statistically controlled. Finally, the religious problem-solving measure developed by Pargament and colleagues was factor analyzed to assess its validity among urban parents of children with asthma.
Factor analysis of religious problem-solving orientation
The dimensionality of the 18 items from the religious problem-solving measure was analyzed using maximum likelihood factor analysis. The scree plot showed a two factor solution, each of which had an eigenvalue greater than one. Two factors were rotated using a Varimax rotation procedure. In Table 1 the factor loadings are presented for each item. Although one item (#14) loaded weakly on both factors, all remaining items loaded on their primary factor at 0.64 or above and loaded on the other factor at 0.27 or below. The factors were easily interpretable with relation to Pargament and colleagues, 24 original conceptualization. The first factor includes all items on the original collaborative and deferring subscales, both of which could be considered types of God-involved problem-solving. The second factor includes all items on the original self-directed subscale, with the exception of item #14, which did not load on either factor and was dropped from all subsequent analyses in this study. Cronbach's alpha was calculated for the two factors and internal consistency estimates were high: 0.96 for God-involved problem-solving and 0.89 for self-directed problem-solving.
Results
Descriptive and bivariate analyses
Descriptive statistics of the study sample appear in Table 2. Pearson product- moment correlations and one-way ANOVAs were utilized to explore associations between demographic and primary study variables. Child's age was significantly and positively correlated with parents' self-directed problem solving (r = 0.27, P < 0.05) and therefore was controlled for in all regression analyses. A series of independent samples t-tests was conducted to examine the effects of gender on primary study variables. A significant difference (t (64) = −2.055, P = 0.04), emerged in parents' alternative medication beliefs by child's gender, with parents of girls having more positive views toward alternative medication (M = 39.37, SD = 4.78) than parents of boys (M = 36.83, SD = 5.15).
Demographic characteristics of participants (n = 66).
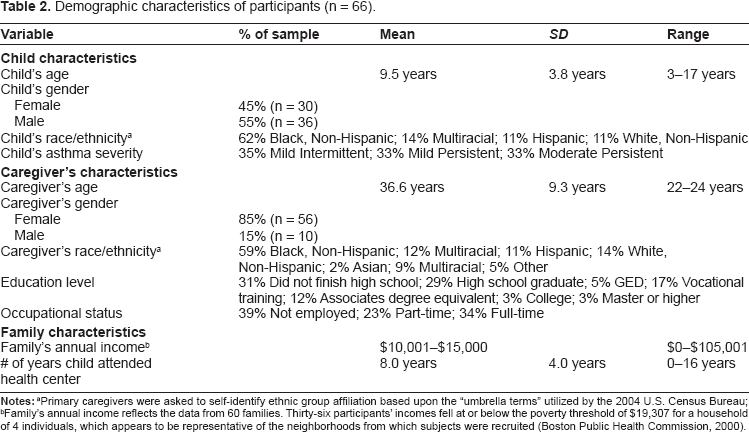
Primary caregivers were asked to self-identify ethnic group affiliation based upon the “umbrella terms” utilized by the 2004 U.S. Census Bureau;
Family's annual income reflects the data from 60 families. Thirty-six participants' incomes fell at or below the poverty threshold of $19,307 for a household of 4 individuals, which appears to be representative of the neighborhoods from which subjects were recruited (Boston Public Health commission, 2000).
Multivariate/mediational analyses
Two meditational models were tested, the first including the predictor of conventional medication beliefs, and the second including the predictor of alternative medication beliefs. Initial correlational analyses of God-involved problem solving did not support its role as a mediator, and thus only self-directed problem solving was tested as a mediator in regression analyses.
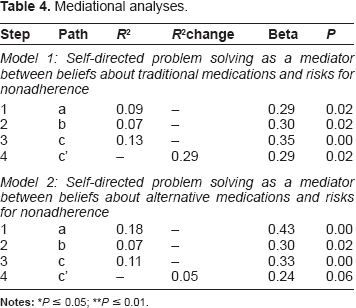
Conventional medication beliefs was significantly associated with risks for nonadherence (β = 0.35, P = 0.00, R2 = 0.13) and with self-directed problem solving (β = 0.29, P = 0.02, R2 = 0.09). Self-directed problem solving was associated with risks for nonadherence (β = 0.30, P = 0.02, R2 = 0.07). When conventional medication beliefs was entered into a hierarchical regression equation after the variance of self-directed problem solving was taken into account, its association with risks for nonadherence was weakened (β = 0.29, P = 0.02, R2 change = 0.08), suggesting partial mediation.
Bivariate correlations of demographic and primary study variables (n = 66).

P ≤ 0.05;
P ≤ 0.01.
More positive alternative medication beliefs was positively and significantly associated with risks for nonadherence (β = 0.33, P = 0.00, R2 = 0.11) and with self-directed problem solving (β = 0.43, P = 0.00, R2 = 0.18). When alternative medication beliefs was entered into a hierarchical regression equation after the variance of self-directed problem solving was taken into account, it was no longer a significant predictor of risks for nonadherence (β = 0.24, P = 0.06, R 2 change = 0.05), suggesting full mediation. Please see Table 4.
Mediational analyses.
Discussion
Religious problem-solving factor analysis
Pargament and colleagues 24 identified three religious problem solving styles (self-directed, collaborative, and deferring) in a sample of white, middle class adults. In the current sample of families from varying racial and ethnic backgrounds living in low income urban neighborhoods, the self-directed problem solving factor was replicated. However, items from the original deferring and collaborative problem solving styles loaded onto a single factor (ie, God-involved), suggesting that the primary distinction in individuals' problem-solving attempts regards whether there is any involvement of God versus none at all. In contrast to the original sample, which was recruited from a church-going population, the current sample was recruited from community health centers. It is possible that these participants were less religiously-oriented than members of Pargament and colleagues' sample, which may have decreased the measure's sensitivity to detect subtle differences in religious problem solving. Moreover, given the disparate demographic composition of the two groups, comparisons must be made with caution. It should not be assumed that there are only two religious problem-solving styles. Rather, religious problem solving may be distinctly different depending on the racial, ethnic or sociocultural background of the individual. Despite these significant differences, however, it is noteworthy that similar factor loadings emerged. These preliminary results highlight the importance of analyzing the factor structure of instruments across diverse sociocultural contexts.
Associations among beliefs about medications and risks for nonadherence
More positive beliefs about conventional and alternative medications also were predictive of more risks for nonadherence. Positive conventional medication beliefs have typically been associated with enhanced asthma management and treatment adherence. 28 The current findings could stem from the nature of the outcome measure in this study, risks for nonadherence, which includes a range of asthma management issues (eg, inability to schedule doctor's appointment when needed, having medication in the home if the child needs it, having multiple children in the home who have been diagnosed with asthma), some of which could be linked with low socioeconomic status. Parents' strong sense of trust in the effectiveness of conventional medications may predispose them to undervalue the importance of avoiding environmental triggers (eg, cigarette smoke, pet dander) to control their children's asthma. In the current sample of urban, primarily low-income families, children's exposure to environmental triggers may be high, resulting in greater risks for nonadherence. Thus, a parent's overconfidence in the effectiveness of conventional medications to fix asthma exacerbations may be particularly problematic in this sociocultural context. The link between alternative medication beliefs and risks for nonadherence also mirror findings that CAM utilization for asthma symptoms can result in poorer health outcomes. 26 Moreover, researchers have questioned if other sociocultural (eg, religion) or biological factors (eg, bronchodilator reversibility) may influence the association.26,33
Self-directed religious problem-solving as a mediating variable
Of the two problem-solving orientations identified in this sample, self-directed problem solving was a more consistent and powerful correlate of other study variables than God-involved problem solving. God-involved problem solving was negatively and significantly correlated with self-directed problem solving, but it was not significantly correlated with age, asthma severity, or the study predictor and outcome variables.
Self-directed problem solving mediated the associations of both conventional and alternative medication beliefs with risks for nonadherence. The steps of mediation testing yielded several intriguing findings regarding associations among medication beliefs, problem-solving and risks for asthma treatment nonadherence. More positive beliefs about both conventional and alternative medications were associated with higher levels of parents' self-directed problem solving. It is important to note that using a self- directed approach does not negate God's involvement; rather, it presumes that God allows individuals free will to determine the best course of action to solve problems. Thus, strong beliefs in either conventional or alternative approaches could be viewed as consistent with this orientation. It is not surprising that individuals with a strong sense of confidence in conventional western health care would tend to value secular forms of illness management and may not involve God in this process. This perspective is consistent with previous results from the current dataset indicating that that parents with more positive beliefs about conventional medications reported using fewer forms of CAM, 26 including religious treatment strategies. Likewise, individuals who have a strong investment in CAM and/or holistic approaches may rely on their own personal judgments and act autonomously in managing health concerns (which would be reflected in a higher self-directed problem solving score in this study), even if they ultimately choose to use CAM strategies in managing their children's asthma.
Interestingly, higher levels of self-directed problem solving were associated with greater risks for nonadherence. There are several possible interpretations of this finding. Parents who highly value free will in problem-solving may possess other personality characteristics that affect their approaches to illness management. It could be speculated that such parents feel more empowered to take personal responsibility for deciding how to manage children's asthma symptoms, as opposed to strictly complying with prescribed treatment regimens. They also may be more likely to utilize a variety of methods to manage asthma. Moreover, parents who are confident in their own knowledge and skills related to asthma may be less likely to engage in activities that promote continued education about asthma management (eg, formal asthma education classes or talking with other parents). To the extent that any of these patterns of behavior do not conform to current standards of conventional medical care, children's measured risks for nonadherence scores would be higher in this study.
Alternatively, a parent's strong sense of independence from God in decision-making may reflect other aspects of family life affecting risks for nonadherence. For instance, individuals endorsing high levels of self-directed problem solving on this measure may be less likely to be affiliated with religious organizations and thus may not benefit from positive aspects of religious involvement such as perceived support from God or emotional and instrumental support from other community members. With limited sources of support and coping, parents may be vulnerable to illness-related or life stressors, resulting in increased risks for nonadherence.
Limitations and future directions
The current study provides a preliminary assessment of sociocultural constructs that have received little attention in the pediatric asthma literature, but findings should be interpreted in light of its methodological limitations. First, with regard to assessment, common reporter variance is a potential issue, as all primary study variables were obtained from parent self-report. Also, the risks for nonadherence scale is a proxy measure for asthma outcomes, but objective measures of asthma outcomes would have been ideal. Second, statistical power of this study was limited by a small sample size. Moreover, although factor analysis is typically utilized in larger samples, its use in the current small sample is warranted given the relationship among factor loadings, number of factors, and number of items in this data. 34 Third, with regard to the sample, participants were drawn from three community health centers serving a large number of children with asthma. Parents that participated may not be fully representative of families served in urban community health centers, as they may be characterized by fewer asthma-related and/or life stressors that would pose a barrier to participation. Furthermore, the age range of children was between 3 and 17, which is a large range with significant implications for treatment adherence. However, analyses conducted by age did not yield statistically significant differences on primary study variables. Lastly, limitations are present with regard to the study's design. The temporal relationships among variables cannot be determined in this cross-sectional data.
Our aim in this study was to conduct preliminary analyses to examine the utility of the Religious Problem Solving Questionnaire in a diverse population and examine associations with parental beliefs and nonadherence. Although the questionnaire shows promise, further data on the use of this measure in diverse populations should be collected and examined to validate these findings. Given that God-involved problem solving did not emerge as a significant variable in our study, the role of other mitigating variables must be considered. For instance, it is plausible that other factors that are more proximal to the families' current situation may have a more significant impact asthma outcomes than religious problem solving. These factors could be related to families' living environments (eg, exposure to asthma triggers), socioeconomic factors (eg, money for medications), and factors related to healthcare utilization (eg, medication adherence, relationship with healthcare providers).
As the importance of religious beliefs and practices continue to be a source of support in families coping with chronic illness, it is important that researchers continue to view religiosity and religious problem solving as working through a variety of mechanisms to influence health and chronic illness. For instance, effective problem solving fosters better coping with difficult events, an increased sense of control and hope, a decreased sense of isolation, or a sense of meaning and purpose in life. 22 Parents' religious problem-solving should be explored in association with religious involvement in order to clarify mechanisms through which self-directed and God- involved problem-solving styles might influence illness management. Importantly, studies should assess not only parents' beliefs and behaviors surrounding asthma medications, but also their other strategies for asthma control (eg, minimizing triggers), as well as the influence of socioeconomic, environmental and cultural factors. With a clearer perspective of the role of families' philosophical and religious beliefs and behaviors in pediatric asthma management, more effective protective processes may be targeted to reduce asthma disparities across sociocultural contexts.
Disclosure
This manuscript has been read and approved by all authors. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The authors and peer reviewers of this paper report no conflicts of interest. The authors confirm that they have permission to reproduce any copyrighted material.
Footnotes
Acknowledgments
This research study was funded by the the University of Massachusetts Bollinger Dissertation Grant, the University of Massachusetts Boston Doctoral Dissertation Grant Program, and the Ronald E. McNair Post–Baccalaureate Achievement Program.