
Abstract
Household pharmaceuticals are ubiquitous and untold quantities are wasted annually. Most often, people dispose of household pharmaceuticals by flushing them down the toilet, pouring them down the drain, or throwing them away in the trash. Pharmaceuticals disposed in this manner compromise the safety of our environment. This article provides a comprehensive review on the public health issue of household pharmaceutical waste, describing its epidemiology, explaining its effects on aquatic and human life, estimating its cost burden, and discussing strategies for reducing environmental exposure to it. In doing so, this article proposes two key objectives for our nation: (1) reduce the amount of household pharmaceuticals wasted and (2) devise environmentally friendly and cost-effective ways for handling this waste once it has been generated.
Keywords
Introduction
Prescription and non-prescription drugs, herein referred to as pharmaceuticals, are critical to maintaining health and improving the quality of life for millions of Americans. Not all pharmaceuticals dispensed to or purchased by people are consumed or used. Unconsumed or unused pharmaceuticals frequently are wasted. For example, it has been estimated that hospitals and long-term care (LTC) facilities waste at least 125 million pounds of pharmaceuticals per annum. 1 Although many health services researchers have addressed various issues related to pharmaceutical waste generated by the health services industry, there are currently no articles that fully address issues related to pharmaceutical waste generated by households. This article provides a comprehensive review on the public health issue of household pharmaceutical waste, describing its epidemiology, explaining its effects on aquatic and human life, estimating its cost burden, and discussing strategies to reduce environmental exposure to it.
Epidemiology of Household Pharmaceutical Waste
Pharmaceutical use in the United States
In the United States, the use of prescription drugs, as measured by the number of prescriptions purchased and the annual rate of growth in prescription drug spending, increased considerably over the last 15 years. From 1993 to 2003, the number of prescriptions purchased increased 70% (from 2.0 billion to 3.4 billion). 2 Between 1995 and 2004, the annual rate of growth in prescription drug spending was, on average, 13.4% per year. 3 In 2005, approximately 3.6 billion prescriptions were purchased in the United States, 4 and in 2006, prescription drug spending increased 8.5% from the prior year to reach $216.7 billion. 3 The use of non-prescription drugs has also increased appreciably over time.5–9 However, accurate estimates of non-prescription drug use are comparatively limited because many studies that approximate use of pharmaceuticals either exclude non-prescription drugs or categorize over-the-counter (OTC) drugs and dietary supplements into one category.
At any given period in time, most U.S. adults consume or use at least one pharmaceutical, and many consume or use multiple pharmaceuticals. Using data from the National Social life, Health and Aging Project (NSHAP), researchers studied pharmaceutical use among a nationally representative probability sample of community-residing individuals aged 57 through 85 years. 10 Key findings from the NSHAP are summarized in Table 1. Among 2,976 individuals, 81% used at least one prescription drug on a regular schedule and 29% used at least five. Overall, 91% of U.S. older adults regularly used at least one pharmaceutical. This rate translates into approximately 50.5 million adults aged 57 to 85 years in the United States. 10
Weighted prevalence estimates of pharmaceutical use by sociodemographic characteristics.
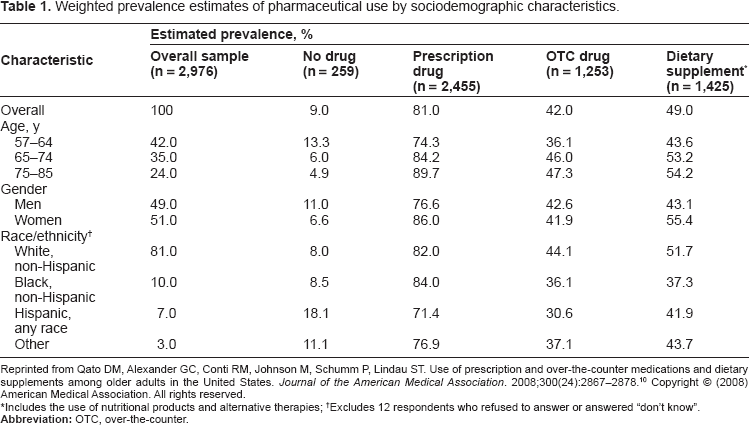
Reprinted from Qato DM, Alexander GC, Conti RM, Johnson M, Schumm P, Lindau ST. Use of prescription and over-the-counter medications and dietary supplements among older adults in the United States. Journal of the American Medical Association. 2008;300(24):2867–2878. 10 Copyright © (2008) American Medical Association. All rights reserved.
Includes the use of nutritional products and alternative therapies;
Excludes 12 respondents who refused to answer or answered “don' t know”.
An on-going telephone survey of a random sample of the non-institutionalized U.S. population (The Slone Survey) showed that among 2,590 individuals aged at least 18 years, 51% used at least one prescription drug during the preceding week and 7% used at least five. Use of non-prescription drugs was also widespread; 40% used one or more vitamin or mineral supplements and 14% used at least one herbal/supplement during a given week. 11 Overall, 81% of U.S. adults used at least one pharmaceutical and 25% used at least five. These rates translate into approximately 169 million and 52 million adults aged 18 years and over, respectively, in the United States. 11
Pharmaceutical waste in the United States
Reasons pharmaceuticals are wasted
Pharmaceuticals designed for humans often are wasted for a variety of reasons. These reasons include, but may not be limited to: the person's medical condition resolves before the pharmaceutical is completely consumed or used; the person experiences an intolerable adverse effect from the pharmaceutical and must stop taking or using it; the person refuses to take or use the pharmaceutical as instructed by his/her prescriber; the pharmaceutical is not effective and the prescriber discontinues or changes it; the pharmaceutical expires or spoils before it is completely consumed or used; or the person dies and leaves behind a supply of pharmaceuticals.12,13 Some of these reasons, such as refusing to take or use the pharmaceutical as instructed, represent potential targets for intervention to reduce pharmaceutical waste.
Scope and magnitude of household pharmaceutical waste
Because U.S. consumers do not keep data on the waste they generate, national estimates of household pharmaceutical waste do not exist. However, in studies performed in and outside the United States, enormous quantities of household pharmaceutical waste have been documented.14–16 In a U.S. pilot study, for example, approximately 17,000 drugs were returned to a community pharmacy located in Houston, Texas over a six-month period. 14 In disposal programs in Alberta, Canada, more than 204 tons of unused drugs were collected over an eight-year period. 15
Two relatively new approaches to acquire data to assess the scope and magnitude of household pharmaceutical waste are to measure the quantity of drugs wasted by hospice programs and the inventories of drugs maintained by coroner offices. Hospice programs provide compassionate care for people living with life-limiting illnesses or injuries. In 2008, the last year for which complete data are available, an estimated 1.45 million patients enrolled in hospice programs; of those, 963,000 (66.4%) died, representing approximately 38.5% of all deaths in the United States. 17 Patients aged 65 years or older are the dominant users of hospice services, accounting for more than 80% of all hospice enrolees. 17 These patients are also the dominant users of drugs, with nearly half using five or more drugs; among those, the most frequently used drugs are opioid analgesics,18,19 which are classified as controlled substances. When a hospice patient dies, most unused drugs are wasted, usually without violating state or federal regulations. 20 As the U.S. population ages, the quantity of drugs wasted by hospice programs is expected to grow, yet there are few data documenting the extent of this waste.
To begin to acquire data to assess the scope and magnitude of drugs wasted by hospice programs in the United States, a group of researchers performed a retrospective chart review of 100 hospice patients who died consecutively between November, 2004 and March, 2005. After exclusion criterion was applied, the final sample was comprised of 51 hospice patients with a mean age of 73.3 years (standard deviation [SD], 14.1). At the time of death, the mean number of drugs per patient was 9.7 (SD, 4.2). 21 The top 10 drugs wasted following the death of these patients are listed in Table 2. With the exception of haloperidol, all of the top 10 drugs wasted were controlled substances. The quantity of drugs wasted totalled 4,762 milliliters, 2,496 tablets, and 67 patches. The average cost of wasted drugs per patient was between approximately $100 and $200. 21 With 963,000 patients dying in U.S. hospice programs per year, this may mean that up to $192,600,000 of drugs are being wasted by hospice programs nationally.
Cost of the top 10 drugs wasted by the Northwestern Memorial Home Hospice Program.
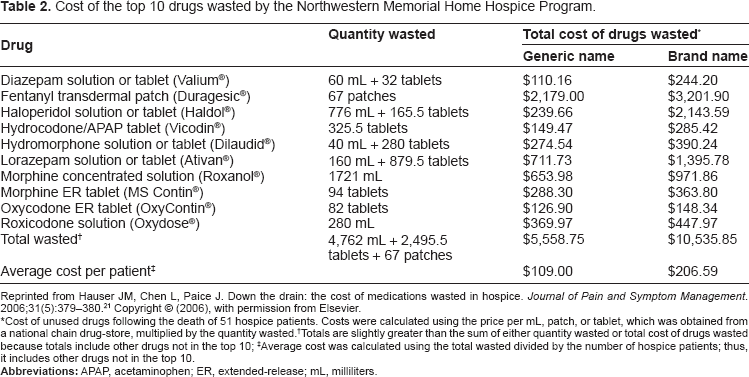
Reprinted from Hauser JM, Chen L, Paice J. Down the drain: the cost of medications wasted in hospice. Journal of Pain and Symptom Management. 2006;31(5):379–380. 21 Copyright © (2006), with permission from Elsevier.
Cost of unused drugs following the death of 51 hospice patients. Costs were calculated using the price per mL, patch, or tablet, which was obtained from a national chain drug-store, multiplied by the quantity wasted.
Totals are slightly greater than the sum of either quantity wasted or total cost of drugs wasted because totals include other drugs not in the top 10;
Average cost was calculated using the total wasted divided by the number of hospice patients; thus, it includes other drugs not in the top 10.
In 2007, another group of researchers performed a retrospective chart review of 105 hospice patients (mean age, 78 years) who died between April, 2007 and June, 2007. Patients were included if they had a completed controlled substance waste destruction record. At the time of death, the overwhelming majority of hospice patients had unused controlled substances in the home. The most commonly unused controlled substances were morphine concentrated solution (99.0% of patients), lorazepam solution or tablet (64.8% of patients), fentanyl transdermal patch (9.5% of patients), and roxicodone solution (6.7% of patients). Among those, more than three liters (3,184 mL) of morphine concentrated solution, 397 milliliters of lorazepam solution, 990 tablets of lorazepam, 57 fentanyl transdermal patches, and 382 milliliters of roxicodone solution were wasted. 20 These findings, coupled with those of Hauser et al 21 indicate that a sizeable quantity of unused drugs are wasted when a hospice patient dies. The fact that countless quantities of wasted drugs are not recorded by hospice programs or have not been measured by researchers suggests that pharmaceutical waste generated by hospice programs in the United States may be grossly underestimated.
As aforementioned, one approach to acquire data to assess the scope and magnitude of household pharmaceutical waste is to measure the inventories of drugs maintained by coroner offices. These inventories, which are compiled as standard protocol by most coroner offices in the United States, are an accurate record of drugs wasted by decedents. 22 Data from a pilot study conducted by the Clark County Coroner's Office (CCCO) in Clark County, Nevada demonstrates proof of this concept.
In 2005, the death rate for Clark County, Nevada was 0.008, which was also the death rate for the United States during 2005. 22 Among the 13,761 deaths reported in Clark County in 2005, 10,135 deaths were reported to the CCCO. The total number of cases accepted by the CCCO was 3,393; of those, 1,574 (46.4%) included drug inventories. During the calendar year of this pilot study, at least 325,000 doses of a wide array of drugs, not including liquids, powders or delivery systems (such as inhalers, patches, and syringes), were collected and disposed of by the CCCO. These doses represented greater than 102 kilograms of active pharmaceutical ingredients (APIs) disposed into the environment. Extrapolating these data to the entire U.S. deceased population, the CCCO estimated that at least 17.9 metric tons of APIs are disposed of by coroner officers annually. 22 If this new approach to acquire data about drugs wasted by decedents was applied on a nationwide basis, it could increase our understanding of the scope and magnitude of household pharmaceutical waste in the United States. 22
Household Pharmaceuticals in the Environment
How household pharmaceuticals enter the environment
Household pharmaceuticals enter the environment in three major ways: (1) they are excreted by the human body, (2) they wash off the human body, or (3) they are disposed. After consumption, pharmaceuticals are metabolized in the body and excreted as either the unaltered parent compound or metabolites, some of which are active compounds. These byproducts are flushed down the toilet and subsequently released into sewage water. 23 After topical application, some pharmaceuticals are washed off during bathing, thereby also entering the domestic sewage system. Thus, a certain amount of environmental pollution from pharmaceuticals is inevitable. Another source of environmental pollution, however, is the disposal of unconsumed or unused household pharmaceuticals.
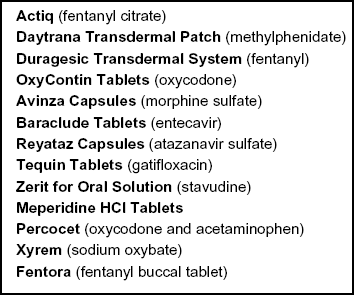
One method of disposal of unconsumed or unused household pharmaceuticals is to flush them down the toilet or pour them down the drain. In February 2007, the White House Office of National Drug Control Policy (ONDCP), in collaboration with the U.S. Food and Drug Administration (FDA) and the Environmental Protection Agency (EPA), published federal guidelines for the proper disposal of drugs. 24 The guidelines recommended that 13 specific drugs with a high potential for abuse or acute toxicity be flushed down the toilet (see Box 1). In October 2009, the guidelines were updated 25 and the list of 13 specific drugs to be flushed down the toilet was removed. Instead, the guidelines refer consumers to a new website launched by the FDA for an updated list of drugs that should be flushed down the toilet or poured down the drain (see Box 2). 26 For a description of U.S. governmental agencies discussed in this article, see Appendix A.
Original list of drugs recommended for disposal by flushing down the toilet. 24
The Drug Enforcement Administration (DEA; see Appendix A) requires most LTC facilities to dispose of unused controlled substances directly, which usually means flushing them down the toilet. 12 Following the death of a hospice patient, the U.S. Code of Federal Regulations 42 CFR 418.96 states: “The hospice must have a policy for the disposal of controlled drugs maintained in the patient's home when those drugs are no longer needed by the patient.” 33 Previously described research has shown that hospice programs commonly dispose of unused controlled substances in the home by flushing them down the toilet or pouring them down the drain. 20 Similarly, the most common method used by coroners to dispose of pharmaceuticals remaining in the household following a person's death is to flush them down the toilet. 22
Disposal by flushing down the toilet or pouring down the drain is not recommended for the vast majority of pharmaceuticals. With the exception of the drugs listed in Box 2, it is recommended that most unconsumed or unused pharmaceuticals be disposed of in the household trash. Specifically, the ONDCP and FDA recommend that most pharmaceuticals be disposed of in the household trash by: (1) taking them out of their original containers; (2) mixing them with an unpalatable (or undesirable) substance such as used coffee grounds or kitty litter; (3) putting the mixture into an impermeable, non-descript disposable container with a lid such as an empty coffee can or into a sealable plastic bag; (4) concealing or removing any personal information from the empty original containers; and, (5) throwing the sealed container or plastic bag with the mixture, and the empty original containers, in the household trash.24–26
Updated list of drugs recommended for disposal by flushing down the toilet or pouring down the drain. 26

Of the two disposal methods, disposal of household pharmaceuticals by flushing them down the toilet or pouring them down the drain is the most significant contributor to water pollution. Pharmaceuticals disposed in this manner are released directly to the environment after passing through wastewater treatment plants or domestic septic systems, which often are not designed to remove pharmaceuticals from the effluent. 34 The result is that small concentrations of pharmaceuticals can end up in drinking water. 12
Disposal of household pharmaceuticals by throwing them into the household trash can also contribute to water pollution. Pharmaceuticals disposed in this manner are delivered to landfills. If these pharmaceuticals are not protected from environmental exposure and not biodegraded, they may leach into groundwater and eventually end up in streams, rivers, or drinking water. Certain antibiotics (e.g. tetracyclines), for example, have a strong tendency to bind with sewage sludge, soils and sediments and, therefore, take months to biodegrade.35–41 Generally, however, throwing pharmaceuticals into the household trash, especially in impermeable containers, results in less water pollution than flushing pharmaceuticals down the toilet or pouring them down the drain because landfills do not empty directly and immediately into waterways like some sewage. 12
Quantity of household pharmaceuticals in the environment
Over time, the use of pharmaceuticals in the United States has been steadily increasing, driven by both pharmaceutical development and an aging population. As a result, the amount of household pharmaceutical waste that is generated and thus the quantity of household pharmaceuticals in the environment is also increasing. 42 Only recently, though, has improved testing equipment been capable of detecting pharmaceuticals at low concentrations, which might be expected in the environment. 43 Even with improved testing equipment, however, it has been difficult for scientists to determine the exact sources of pharmaceuticals in the environment and their correlations to the quantities of unconsumed or unused pharmaceuticals in the home. 22 Nevertheless, pharmaceuticals are increasingly being detected in our nation's water and the massive amount of pharmaceuticals being flushed down the toilet, poured down the drain and thrown in the trash by consumers might aggravate an emerging public health problem.
The U.S. Geological Survey (USGS) provided the first and largest nationwide investigation of the occurrence of organic wastewater contaminants, including pharmaceuticals, in streams. 43 During 1999–2000, USGS personnel sampled water from 139 streams across 30 states to determine if organic wastewater contaminants are entering U.S. streams and to estimate the extent of their occurrence in these waters. One or more of the 95 organic wastewater contaminants evaluated were detected in 80% of the streams sampled for this study, with most (75%) of the streams having mixtures of various contaminants. Among the human pharmaceuticals detected, non-prescription drugs were found with greater frequency than prescription drugs. The most commonly detected non-prescription drug was acetaminophen and the most commonly detected prescription drug was the antibiotic class, including erythromycin, lincomycin, sulfamethoxazole and trimethoprim. Collectively, these specific drugs comprised 16.7% of the 30 most frequently detected organic wastewater contaminants. The levels of concentration of these drugs were low, with median detectable concentrations well below 1 μg/L. 43
Although previous research in other countries has also shown that pharmaceuticals can be introduced into the aquatic environment,44–47 the USGS is the first to document that detectable quantities of pharmaceuticals occur in U.S. streams at the national scale. 43 This indicates that many pharmaceuticals survive wastewater treatment in the United States. In March 2008, as part of an ongoing investigation, the Associated Press shockingly reported that trace concentrations of various pharmaceuticals–-including antibiotics, anticonvulsants and sex hormones–-were detected in the water supplies of 24 major metropolitan areas that provide drinking water for at least 41 million Americans. 48 Although the measured concentrations of pharmaceuticals in the water supplies were low, the findings are still disconcerting. Currently, few wastewater treatment plants even test for the presence of pharmaceuticals and the federal government has not set safety limits for pharmaceuticals in drinking water. Moreover, there is genuine concern that pharmaceuticals in water, even in trace concentrations, could be affecting aquatic organisms and human health. 49
Effect of household pharmaceuticals on aquatic and human life
Aquatic life
Scientists theorize that chronic exposure to even extremely small concentrations of pharmaceuticals could produce harmful effects in aquatic life that would be so insidious that they would be undetectable or go unnoticed until it was too late to reverse them.49–53 In recent years, scientists have found evidence to support the theory that pharmaceuticals in the water harm fish and other aquatic organisms. One of the major findings is the presence of intersex characteristics in fish. The presence of this abnormality has been found in a number of waterways in the United States, including Oregon and West Virginia,54,55 and other countries, including China and the United Kingdom.56–58 As part of the Chesapeake Bay studies (http://chesapeake.usgs.gov/), the USGS found that intersex characteristics in fish were widespread throughout the Potomac and Shenandoah Rivers. 59 The USGS scientists believe that one potential cause of this abnormality is certain pharmaceuticals (e.g. estrogens) that act as endocrine disruptors. Endocrine disruptors are chemicals that interfere with the natural balance of hormones in living organisms. 59
Although scientists have discovered changes in aquatic life that they attribute to pharmaceuticals, scientists have not been able to conclude from field studies, like the Chesapeake Bay studies, that pharmaceuticals directly cause intersex characteristics in fish. In addition, household pharmaceutical waste is only one source of endocrine disruptors in the water. Thus, the contribution of household pharmaceutical waste to the fish-related problems detected in the Chesapeake Bay and in a number of waterways in the United States is unknown. There is a need to further study the extent and cause of aquatic-health problems in the United States and the impact of household pharmaceuticals on this problem. Identifying the pharmaceuticals that are impacting aquatic life and their source will help scientists develop solutions for the problem. 59
Human life
Because there are no testing requirements or safety limits for pharmaceuticals in drinking water, millions of Americans are unwittingly consuming an array of drugs that may be harmful to their health. Potential health concerns from the presence of pharmaceuticals in drinking water include: increased risk of developing cancer, reproductive impairment, and the selection and development of antibiotic-resistant bacteria. 43 These concerns focus on certain drug classes: chemotherapeutic drugs or hormones that can be carcinogenic, hormones that can fetter reproduction or development, and antibiotics that can allow bacteria to mutate into more dangerous forms. 48
Estradiol and synthetic estrogens, which are common constituents of contraceptives and hormone replacement therapies, are established carcinogens in humans. 60 Based on this evidence, some scientists believe that environmental exposure to pharmaceuticals containing estradiol and synthetic estrogens contribute to many unexplained cases of cancer, particularly female breast cancer.61,62 These scientists hypothesize that people who reside in locations where the water is highly polluted by household pharmaceutical waste might take in exogenous estrogens by drinking water. Once ingested, these foreign chemicals may promote the development of breast cancer in a variety of ways, such as through vasculogenesis. 61 Although it is difficult for scientists to link household pharmaceutical waste to female breast cancer, the evidence showing that exogenous estrogens induce carcinogenesis in humans suggests that estrogens in the environment may be a contributing factor.
Exogenous estrogens also pose a health hazard to men. Experimentally, reproductive abnormalities and testicular cancers have occurred in laboratory animals exposed to exogenous estrogen in utero.63–65 These laboratory studies suggest that there are physiological mechanisms by which exposure to exogenous estrogens in fetal life could lead to adverse changes in male reproductive development and function in humans. 66 One of the factors that could, at least theoretically, be partly responsible for the increased exposure of infants to exogenous estrogen during gestation is increased levels of synthetic estrogens in the environment 66 –-a potential consequence of household pharmaceutical waste. Despite the fact that there is no direct evidence from human studies validating a causal link between exposure and effect, trepidation exists and is supported by reports of reproductive and developmental impairment in animals. 67
Resistance to antibiotics constitutes a major threat to public health. Research has shown that a multitude of antibiotics are present in freshwater.43,44 In a national study of antibiotic resistance in freshwater, scientists found that antibiotic-resistant bacteria were widespread in water samples from 16 U.S. rivers. 68 One reason cited is that the exposure of water to antibiotics, such as when people flush unused antibiotics down the toilet, selects for resistant bacteria.69,70 A growing body of evidence supports that even low-level concentrations of antibiotics in the environment could increase the rate at which bacteria develop resistance to antibiotics.71–74
Notwithstanding the aforementioned health concerns, several studies and entities, such as the Pharmaceutical Research and Manufacturers of America (PhRMA), have concluded that pharmaceuticals tested to date in surface and drinking water pose no appreciable risk to human health because environmental concentrations are generally found to be several orders of magnitude below therapeutic or toxic levels.75–79 Based on their research, scientists conducting these studies and PhRMA believe that the detection of household pharmaceuticals in the environment reflects nothing more than better analytical technology. While it is true that better analytical technology now allows scientists to detect household pharmaceuticals in the environment at very low or minute concentrations and this ability will only improve with time, 27 currently no data are available on countless pharmaceuticals being used by consumers and hundreds of new pharmaceuticals are constantly in development. Even with improvements in analytical technology, it has become clear that household pharmaceuticals are ubiquitous and it is doubtful that even the best technology will be able to predict the long-term impact of continual exposure to combinations of pharmaceuticals on highly complex organisms such as humans. 49 Much is yet to be learned about the effects on humans exposed to low-level concentrations of household pharmaceuticals. Nevertheless, if exposure to low-level concentrations of certain pharmaceuticals, such as exogenous estrogens, does pose a threat to human health, reductions in exposure will provide an opportunity for primary prevention.61,66 More research is needed to better understand this problem and to develop solutions.
Financial Impact of Household Pharmaceutical Waste
Environmental and health concerns are not the only public health implications of household pharmaceutical waste; costs are also an important factor. Whether it is consumers, payers, or other entities, someone paid for the pharmaceuticals that end up being wasted. Any unconsumed or unused pharmaceutical indicates wasted healthcare resources and adds to the total costs of our healthcare system.12,22
Nearly a decade ago, experts estimated that more than $1 billion worth of pharmaceuticals were wasted each year in the United States. 80 Since then, pharmaceutical purchases in this country have increased markedly. More recently, researchers studied the cost of household pharmaceuticals wasted during hospice care. 21 In a single hospice program, they found that the average cost of wasted drugs was between $100 and $200 per patient (Table 2). If these data were extrapolated to the number of patients receiving services from all U.S. hospice programs per year, 17 it would mean that up to $290 million (in 2005 dollars) of drugs are being discarded by hospice programs alone. Considering that hospice programs get paid approximately $135 per patient per day for routine home care, which must cover payment for all of the patient's hospice-related drugs, 81 and that this estimate includes a relatively small segment of the U.S. population, these figures are quite staggering.
Reducing Environmental Exposure to Household Pharmaceutical Waste
Background
There are opportunities to reduce environmental exposure to household pharmaceutical waste in every phase of the life cycle of pharmaceuticals: design; approval and regulation; production; use; and discharge and disposal (see Fig. 1). 27 The top priority should be to reduce the amount of pharmaceutical waste generated, rather than dealing with the pharmaceutical waste once it has been generated. 12 Reducing the amount of pharmaceutical waste generated starts at the beginning of the life cycle, where pharmaceuticals are designed.

Five main target areas for reducing environmental exposure to pharmaceutical waste based on the life cycle of pharmaceuticals.* *Adapted from Becker. 27
Potential Solutions and Recommended Strategies
Use green chemistry
Green chemistry, also known as sustainable chemistry, is the design and application of chemical products and processes that reduce or eliminate the use or generation of hazardous substances. 82 Green chemistry offers great potential to help reduce the amount of pharmaceutical waste related to the design and production of pharmaceuticals. It has the potential to enhance or improve the absorption, bioavailability, or delivery of pharmaceuticals, which makes it possible to design pharmaceuticals with the same therapeutic effect that use less APIs. 27 As a result of using less APIs in the design of pharmaceuticals, the amount of pharmaceutical waste generated both by production and by human excretion is decreased. 27 Green chemistry also has the potential to facilitate more rapid removal of pharmaceuticals upon release to the environment, which ultimately would decrease environmental persistence of pharmaceutical waste. 27 The pharmaceutical industry should incorporate green chemistry principles into its pharmaceutical design and production processes. Providing incentives, possibly through the pharmaceutical approval process, to support the use of green chemistry should be examined by the federal government.
Conduct an environmental Assessment (EA) for all pharmaceuticals
In the United States, the FDA is the federal agency responsible for regulating the approval of pharmaceuticals (see Appendix A). While the FDA is required to conduct an EA for pharmaceuticals seeking approval, there are a number of exclusions to this requirement. The federal government should reevaluate and consider removing these exclusions, thereby requiring an EA for all pharmaceuticals before the FDA will approve them to be marketed.
Reduce the amount of unconsumed or unused pharmaceuticals
In the United States, most drugs are prescribed and dispensed in 30- or 90-day supplies, in part due to insurance requirements.12,83 If prescribers and pharmacies, respectively, could prescribe and dispense in shorter supplies, a great deal of pharmaceutical waste could be avoided. The federal government should fund research and pilot programs to identify new payment systems to encourage prescribing and dispensing in shorter supplies and to explore the use of new technologies, such as automated dispensing systems, that facilitate dispensing in shorter supplies. 12
Coordinate efforts of federal agencies to handle pharmaceutical waste
Currently, there is very little coordination between the FDA, the EPA, and the DEA when it comes to handling pharmaceutical waste. 12 The FDA recommends that consumers take advantage of community pharmaceutical take-back programs. 26 The EPA and the DEA have their own individual efforts underway to address the disposal of pharmaceuticals (see Appendix A). The EPA is addressing the disposal of hazardous pharmaceutical waste, while the DEA is addressing the disposal of controlled substance waste. While this patchwork approach has made some progress in handling pharmaceutical waste, these agencies need to work together to establish more cohesive national guidelines that are environmentally friendly, practical, and safe for the public and healthcare providers. 12
Establish more community pharmaceutical take-back programs
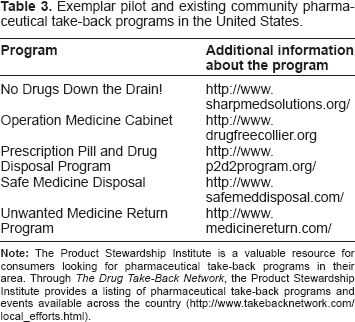
Community pharmaceutical take-back programs are periodic or ongoing events that allow people to bring unconsumed or unused pharmaceuticals to an organized collection site, such as a local pharmacy or police station, for proper management and disposal. 29 Examples of pharmaceutical take-back programs are provided in Table 3. Currently, there are relatively few take-back programs in the United States, primarily because very little funding is available for such programs; they are frequently short-lived, pilot programs funded by federal government grants. 12 To begin to establish more community pharmaceutical take-back programs and to enable them to become permanent programs, the federal government should identify other funding sources for them, including requiring pharmaceutical companies to pay for these programs and levying other waste disposal taxes and fees. 12 Additionally, the federal government must ensure that these programs are convenient to access and free for people who want to participate in them.
Exemplar pilot and existing community pharmaceutical take-back programs in the United States.
Educate the public and healthcare providers about disposal options
Currently, there is no national database or federal coordination to collect and disseminate information to the public or healthcare providers about safe pharmaceutical disposal practices and about community pharmaceutical take-back programs that are available for them to utilize. 12 As a result, the public and healthcare providers may be unaware that these programs exist in their area. To begin to solve this problem, the federal government should establish a national clearinghouse to collect information about safe pharmaceutical disposal practices and community pharmaceutical take-back programs and they should provide technical assistance to state governments to disseminate this information to the public and healthcare providers. 12
Establish more environmentally friendly methods for handling pharmaceutical waste
Incineration has the potential to permanently destroy pharmaceutical waste while simultaneously preventing harm to the environment. It is necessary, however, for the incineration to be done with an incinerator that has been designed and approved for this purpose. 12 Currently, few of these incinerators are available in the United States, and those available can be costly. Providing incentives, possibly through the tax code, to begin to establish more of these incinerators and to expand their use is something that should be explored by the federal government. 12
Although wastewater treatment plants remove some pharmaceuticals, most conventional plants do not effectively remove most pharmaceuticals from wastewater effluents and removal rates are highly variable.84,85 Advanced wastewater treatment techniques such as activated carbon, membrane bioreactors and filtration, and oxidation by chlorination or ozonation can increase pharmaceutical removal rates.27,86 Expanding the use of these techniques to more wastewater treatment plants in the United States is something that should be explored by the federal government and the EPA.
Discussion
The results of this comprehensive review demonstrate that trace concentrations of household pharmaceuticals, such as antibiotics, hormones and controlled substances, are finding their way into our nation's environment. In many cases, household pharmaceuticals enter the water when people excrete them or wash them away in the shower. 87 In other cases, unconsumed or unused household pharmaceuticals are being flushed down the toilet or the drain and disposed of in the trash. Researchers suspect that the quantity of household pharmaceuticals entering our nation's water supply is increasing, particularly because per capita drug use in the United States is on the rise. This has public health and environmental officials in a quandary. 87
On the one hand, there is no evidence that trace concentrations of household pharmaceuticals found in the environment thus far are harmful to human life. On the other hand, researchers have found pharmaceuticals almost everywhere they have looked for them, and there is evidence that trace concentrations of household pharmaceuticals are harmful to aquatic life. This begs the question: should public health and environmental officials wait until scientists can make a still stronger case for a link between household pharmaceutical waste and harmful effects in humans? It would seem cavalier to dismiss the possibility of harm because of a paucity of evidence. Our nation's experience with the most egregious of chemicals such as asbestos, lead, and tobacco demonstrates that it can be costly, in terms of human lives, health and dollars, to defer action until evidence of harm is overwhelming.61,87
Although swift action is needed to mitigate the public health threat of household pharmaceutical waste, implementing the strategies recommended in this article will require major changes in attitudes, behaviour and regulations. These changes will take time and some will likely be met with opposition. For example, the use of green chemistry would require a major change in the way pharmaceuticals are designed and brought to market through the regulatory approval process. Today, without the widespread use of green chemistry, it takes more than a decade (on average) to bring a new pharmaceutical to market in the United States, costing the pharmaceutical company millions or billions of dollars. 27 The issue of who will pay for the use of green chemistry certainly needs to be addressed. Reducing the amount of unconsumed or unused household pharmaceuticals would require a major change in attitude and behaviour among prescribers, payers, pharmacies, and consumers. 83 Consumers would need to access their prescribers and their pharmacies more frequently. In exchange, prescribers and pharmacies would need higher or more frequent reimbursement and dispensing fees, respectively, to support their more labor-intensive services. Payers would need to pass on these fees to consumers, resulting in increased premiums, co-payments, or both. Whether or not such a change is possible, even on a small scale, needs to be explored. In summary, no single strategy will fix the problem of household pharmaceutical waste overnight, yet no action is unacceptable.
Conclusion
Household pharmaceuticals are ubiquitous and untold quantities are wasted annually. Most often, people dispose of household pharmaceuticals by flushing them down the toilet, pouring them down the drain, or throwing them away in the trash. Pharmaceuticals disposed in this manner compromise the safety of our environment. Principal reasons to address household pharmaceutical waste include not only protecting our environment but also safeguarding our health, reducing wasted healthcare resources, and preventing the illegal diversion and the abuse of drugs, especially controlled substances. This article proposes two key objectives for our nation: (1) reduce the amount of household pharmaceuticals wasted and (2) devise environmentally friendly and cost-effective ways for handling this waste once it has been generated.
Disclosure
This manuscript has been read and approved by the author. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The author and peer reviewers of this paper report no conflicts of interest. The author confirms that he has permission to reproduce any copyrighted material.