
Abstract
Objective
Knowing tuberculosis (TB) patients’ satisfaction enables TB program managers to identify gaps in service delivery and institute measures to address them. This study is aimed at evaluating patients’ satisfaction with TB services in southern Nigeria.
Materials and Methods
A total of 378 patients accessing TB care were studied using a validated Patient Satisfaction (PS-38) questionnaire on various aspects of TB services. Factor analysis was used to identify eight factors related to TB patient satisfaction. Test of association was used to study the relation between patient satisfaction scores and patient and health facility characteristics, while multilinear regression analysis was used to identify predictors of patient satisfaction.
Results
Highest satisfaction was reported for adherence counseling and access to care. Patient characteristics were associated with overall satisfaction, registration, adherence counseling, access to care, amenities, and staff attitude, while health system factors were associated with staff attitude, amenities, and health education. Predictors of satisfaction with TB services included gender, educational status, if tested for HIV, distance, payment for TB services, and level and type of health-care facility.
Conclusion
Patient- and health system–related factors were found to influence patient satisfaction and, hence, should be taken into consideration in TB service programing.
Introduction
Patient satisfaction is a key criterion for evaluating the quality of health-care services. 1 It can be defined as the level of congruence between patients’ expectations and their perceptions concerning care received. It is a positive evaluation of the dimensions of health care and also a subjective perception that may be considered a reflection of reality. 2 Patient satisfaction has emerged as an increasingly important health outcome and is currently used for the following purposes: (i) to compare different health-care programs or systems; (ii) to evaluate the quality of care; (iii) to identify which aspects of a service need to be changed to improve patient satisfaction; and (iv) to assist organizations in identifying consumers likely to disenroll. 3 Also, it has been shown to influence health-care utilization and can be a predictor of subsequent health-related behavior such as whether patients are willing to recommend their health-care provider to others. 4 In general, patient satisfaction is a useful measure in assessing patterns of communication among clients, health providers, and health managers.
There are several motivations for surveying patient satisfaction. Traditionally, decisions about health services were made on the basis of the health providers and health authorities’ views on what is in the best interest of the patient. This was informed by the perception that the general public lack the requisite technical knowledge to make informed decisions themselves. However, even though patients may lack the ability to judge specific technical aspects of health services, they serve as the best source of accurate information regarding clarity of explanations, helpfulness of information that they receive, barriers to accessing care or their relationship with health-care providers. 5
With regard to tuberculosis (TB) program services, outcome measures have focused on mortality and microbiologic cure and have neglected patients’ preferences such as satisfaction with care, which may be crucial in influencing clinical and treatment outcomes. 6 However, greater satisfaction with care received has been associated with superior compliance, improved attendance at return visits, better treatment success, and higher cure rates. 7 Furthermore, knowing patients’ satisfaction would enable TB program managers to understand the gaps in health-care delivery, to understand clinicians, and to understand the specific needs of individual patients so that strategies to meet the needs and expectations of patients and improve access to quality TB services are instituted. 6
It is in recognition of this that patient satisfaction surveys are designed for the purpose of determining patients’ views on health-care services and programs. Such surveys help to provide insight into health-care service quality and the demand for these services. These include aspects of care that need improvement in a health-care setting, basis for developing measures to increase utilization of health-care services, as well as help to provide feedback to medical staff, program managers, and policy makers. Such feedback helps in facilitating improved prioritization and improved resource allocation. Patients’ judgment of hospital service quality and their feedback are essential in quality-of-care monitoring and improvement. 8
Despite the increased focus on satisfaction as an outcome measure and a growing body of research, satisfaction has remained difficult to compartmentalize. While numerous satisfaction surveys have been developed, most with acceptable psychometric properties, the factors individual patients use to deem themselves satisfied remain largely unknown. Consequently, studies measuring predictors of satisfaction have explained only a small portion of satisfaction's variance, nearly always less than 20%, because patient satisfaction is a multidimensional health-care construct affected by many variables. 3
Although globally there is growing experience with measures of patient satisfaction, they have been rarely used in Nigeria and particularly with respect to TB services, despite its potential role in improving health-care delivery. 6 Studies on patient satisfaction in the country are few and are often focused on general health-care services and in some cases HIV services. In Nigeria, TB services are provided as part of the primary health-care services and are available mostly but not limited to the primary health centers (PHC). However, a significant proportion of the TB patients are seen in secondary and tertiary health facilities including public and private facilities. These facilities are called Directly Observed Therapy (DOTS) facilities and their scope of service includes diagnosis of TB (where microscopy services are available), supervised TB treatment, health education and adherence counseling, as well as HIV counseling and testing. As part of measures to increase access to TB services, the country launched the Public-Private Mix DOTS program in 2002, which is aimed at increasing private sector participation in TB service provision. 9 Evaluation of TB services has often been based on treatment outcome using sputum acid fast bacilli (AFB) result and clinical assessment and does not take into consideration patient's perception of the quality of service received. Therefore, this present study addresses this gap by evaluating patients’ satisfaction with access and utilization of TB services in southern Nigeria.
Materials and Methods
The study was conducted in six states in southern Nigeria supported by German Leprosy and Tuberculosis Relief Association (GLRA). GLRA provides technical assistance to 15 states out of the 36 states and Federal Capital Territory until recently when Lagos State was ceded to Damian Foundation. The six states were selected by simple random sampling from the list of 15 GLRA-supported states and the selected states include Akwa Ibom, Anambra, Cross Rivers, Imo, Ogun, and Ondo states. In each selected state, DOTS facilities accounting for ≥60% of the patient (case) load in the state were purposively selected based on the following criteria: level of health care–- tertiary, secondary, or primary, and type of health facility–- private or public to ensure adequate representation of the study population. Hence, a total 29 health facilities comprising 6 tertiary health facilities, 14 secondary health facilities, and 9 PHCs were selected. The study population was patients accessing TB services in Southern Nigeria. A total of 378 patients accessing TB care were selected and interviewed using a prevalidated patient satisfaction questionnaire. Because the researchers did not foresee any risk of harm or discomfort to the subjects except the risk of administering questionnaire, they applied and obtained approval of the study and waiver of consent from the Ethics Committee, College of Medicine and Health Sciences, Abia State University, Aba, Abia State, Nigeria.
Inclusion criteria
Only patients who were aged ≥15, confirmed to have TB, and have commenced anti-TB treatment in any of the selected DOTS facilities were enrolled for the study.
Data collection
Identification and interview of eligible participants were carried by out two monitoring and evaluation officers of GLRA. Explanation was provided on the reasons for conducting the survey, and data confidentiality was guaranteed. Exit interview was conducted after a patient has been attended to by the health-care providers in the facility. The study questionnaire assessed socio-demographic characteristics of patients including age, sex, educational level, and marital status as well as if tested for HIV, HIV status, distance between place of residence and DOTS facility, and payment for TB services. Distance between place of residence and DOTS was estimated based on the time taken to reach the DOTS facility, near if it took ≤30 minutes and far if it took more than 30 minutes for a patient to get to a DOTS facility from home. Payment for TB services was used to describe those who paid for either AFB microscopy or anti-TB medications only. However, no patient paid for anti-TB medications but some did pay for AFB microscopy. Waiting time was defined as perceived time spent at various service points–-registration, consultation, and laboratory including waiting to collect laboratory test result. While adherence counseling, which is an integral component of TB services, can be described as the counseling provided to TB patients prior to commencement of treatment. It includes information on TB symptoms and diagnosis and TB medications including dosage, duration, side effects, and benefits, and it is aimed at helping the patient make an informed decision to cooperate with the care provider to achieve cure.
Patient satisfaction with TB services was measured using a total of 38 questions, which follow in chronological order of the sequence of services a TB patient receives from the time of first visit to a DOTS facility till commencement of treatment. In addition, other dimensions of quality of TB care comprising amenities, staff attitude, and confidentiality were assessed. The questionnaire was an adaptation of the patient satisfaction tool used by Nwabueze et al 10 to assess patients’ satisfaction among HIV patients in Anambra State, Nigeria. The tool was originally developed by the Clinical Quality Services Branch of the Bureau of Primary Health Care. The questionnaire (named PS-38) was originally divided into 10 domains (factors) based on review of literature. They included access to TB services (six items), waiting time (four items), registration (four items), health education (five items), and laboratory services (three items). Others were adherence counseling (four items), medication (three items), amenities (four items), staff attitude (three items), and confidentiality (two items). Patient satisfaction was measured using a scale of measurement graded as follows: 5, excellent; 4, very good; 3, good; 2, fair; and 1, poor. The response scale ranged from zero to five, and scores for each domain were calculated by adding the answers to all the items in each domain and the average for each domain calculated.
Statistical analysis
The completed questionnaires were entered into MS Excel 2007 and were exported to SPSS version 20 (IBM SPSS Inc., Chicago, IL, USA) for analysis.
Scale factor structures
The exploratory factor analysis of the patient satisfaction score using varimax rotation yielded eight (8) factors with eigen values greater than 1, and they include the following: access to TB care, waiting time, registration, health education, adherence counseling, medication, staff attitude, and amenities. These factors combined to account for 79.2% of the variance.
Validation of the instrument
The questionnaire was pretested using 20 TB patients in a DOTS facility in Enugu State for feasibility, acceptability, and validity.
Acceptability and feasibility
Feasibility and acceptability were examined by the proportion of missing item responses, interviewer-reported acceptability, and the time and ease of administration.
Reliability
Cronbach's alpha reliability coefficient was used to measure the internal consistency reliability of the PS-38 questionnaire. The full-scale alpha was 0.94, and subscale alpha were access to care = 0.77, waiting time = 0.91, registration = 0.93, health education = 0.94, adherence counseling = 0.91, medication = 0.92, staff attitude = 0.93, and amenities = 0.72, which implies that the scales generated were reliable and the results reproducible.
Patient satisfaction score
Descriptive statistics, including frequencies, percentages, means, and standard deviations, were calculated for the socio-demographic variables and patient satisfaction scores. All the questions that assessed satisfaction level were scored on a five-point Likert scale. After scoring, items within the same subscale were averaged together to create subscale score. Items left blank by respondents (missing data) were ignored when calculating subscale scores. In other words, scale scores represent the average for all items in the scale that were answered. Overall satisfaction was calculated by determining the average of all the mean scores of all the subscales. We used a t-test or analysis of variance (ANOVA) for continuous variables. Bivariate and multivariate statistical tests were used to assess and compare the effect of different variables on overall patient satisfaction score. In bivariate analysis, we studied the relationships among the socio-demographic variables with the eight domains of the questionnaire using t-test/ANOVA. The mean satisfaction score of the eight factors identified in the factor analysis and the mean overall satisfaction were regressed on patients’ characteristics–-age, sex, marital status, educational status, HIV status, and health system factors–-health-care level, health-care type, and distance from DOTS facility using multilinear regression. In all analyses, a P-value of <0.05 was considered statistically significant.
Results
The total number of respondents surveyed was 378 and they comprise Akwa Ibom 52 (13.8%), Anambra 67 (17.7%), Cross Rivers 63 (16.7%), Imo 61 (16.1%), Ogun 60 (15.9%), and Ondo 75 (19.8%) as shown in Table 1. As at 2006, the population of the total population of the six states was 22,095,227, thus accounting for 15.8% of the total population of Nigeria. Their GDP ranges between $6,764 for Anambra State and $14,212 for Imo State and was higher than the national average of $4,874 as at 2010. All the states have adult literacy rate greater than 65%, compared to the national average of 58%.11–14
Distribution of the respondents by states.
Table 2 shows the socio-demographic characteristics of the respondents. Most of them were aged between 21 and 40 (67.7%) with a mean age of 34.6 ± 12.8 years. Majority of them (53.0%) were not married. Most of them (64.8%) possess at least secondary education and 60.1% lived near the DOTS facility. The TB patients studied expressed satisfaction with all the aspects of TB services received. They were most satisfied with access to care and adherence counseling services (median = 3.75), but were least satisfied with amenities (median = 3.17) and staff attitude (median = 3.00). However, overall patient satisfaction score for TB services was fairly high (median = 3.43) (Table 3).
Socio-demographic characteristics of the patients.

Univariate analysis of the patient satisfaction score.

Table 4 shows the association between patient and health facility characteristics and mean patient satisfaction scores. Only age was associated with mean overall satisfaction score (P = 0.03). Men, being married, being HIV positive, utilization of private facility, and tertiary facility were all associated with higher mean overall satisfaction score even though not statistically significant. Age is the only factor significantly associated with satisfaction with registration process (P = 0.01), adherence counseling (P = 0.04), and staff attitude (<0.01). Younger people (aged <40) were less satisfied with the registration process, adherence counseling, staff attitude, and overall satisfaction. Females were significantly less satisfied with the registration process (P = 0.02), even as patients who were not married were less likely to be satisfied with the attitude of DOTS facility staff (P = 0.01). Educational status was not associated with overall satisfaction score; however, patients with lower education were more satisfied with access to care, but were less satisfied with amenities at DOTS facilities. Being HIV negative was significantly related to lower satisfaction score for access to TB care (P = 0.03). Payment for TB services and distance between DOTS facility and place of residence were both significantly associated with satisfaction with staff attitude (P < 0.01; P = 0.03) and amenities (P = 0.03; P = 0.03). Patients who paid for TB services were less satisfied with the attitude of TB staff but were more satisfied with the amenities in TB facilities. On the other hand, those who live near DOTS facilities were significantly less satisfied with the attitude of staff and amenities in DOTS facilities than those living farther away from facilities in which they were accessing care. Type of facility was associated with lower mean satisfaction score for health education (P = 0.02) as TB patients attending private health facilities were less satisfied with health education received from care providers.
Bivariate analysis of respondents’ characteristics, health system factors, and patient satisfaction score.

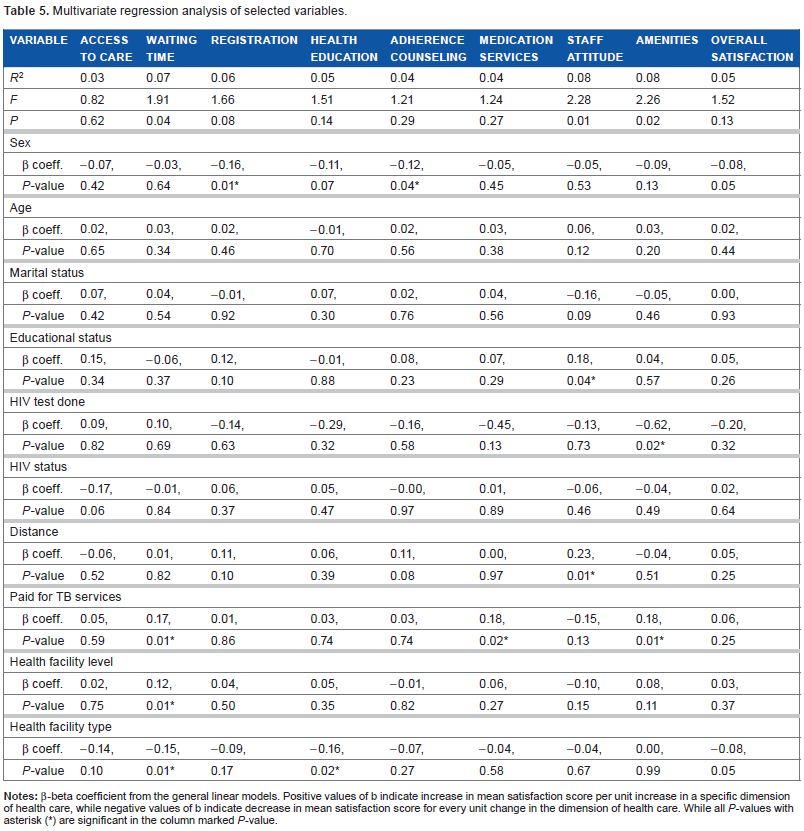
The R2 of each domain model also was estimated and ranged between 0.03 (access to TB care) and 0.08 (staff attitude and amenities). No covariate has significant effect on the following dimensions of TB services–-access to care, registration, and overall satisfaction. Being a male was statistically associated with higher satisfaction with TB registration process (P = 0.01) and adherence counseling (P = 04). Higher educational status was associated with increased satisfaction with staff attitude (P = 0.04). On the other hand, being tested for HIV was associated with decreased satisfaction with amenities (P = 0.02) while living farther away from TB facility was associated with higher satisfaction with TB staff attitude (P = 0.01). Payment for TB services was positively correlated with satisfaction with waiting time (P = 0.01), medication services (P = 0.02), and amenities (P = 0.01). Accessing TB care in higher levels of healthcare system was associated with higher satisfaction with time spent accessing services (P = 0.01), while utilization of private health facilities was negatively correlated with satisfaction with waiting time (P = 0.02) and health education (P = 0.01). Age, marital status, and HIV status were not significantly correlated with mean satisfaction score of any of the dimensions of TB services and overall satisfaction (Table 5).
Multivariate regression analysis of selected variables.
Discussion
Studies that evaluate the satisfaction of patients are permeated by a complex interaction of elements (related to the social characteristics of users and health-care delivery). However, the PS-38 item tool used for this study performed well on most of the psychometric indicators and can be said to be an effective tool for assessing TB services. The scales and the subscales demonstrated acceptable overall internal consistency among TB patients.
Overall patient satisfaction score for TB services in southern Nigeria was high. The aspects of TB care they were most satisfied with were access to care and adherence counseling, while areas of least satisfaction were staff attitude, waiting time, and amenities. Similarly, in Vietnam, patient dissatisfaction with TB services was mostly with respect to long waiting time, poor attitude of staff, poor state of amenities, and limited access to care. 15 In this study, satisfaction with access to care could be attributed to increased access to TB care following DOTS expansion and enhancement embarked upon in recent years, thereby bringing TB services closer to the people. Between 2008 and 2010, the National TB Programme (NTP) undertook massive expansion of TB diagnostic and treatment centers across the country. By the end of 2010, there was nearly 100% DOTS coverage by Local Government Areas, with 3,931 TB DOTS service centers and 1025 TB microscopy laboratory services.16,17
High level of satisfaction with adherence counseling could be because of the reassurance it offers to patients suffering from a disease that is often associated with a number of misconceptions that often result in inappropriate care-seeking practices. Adherence counseling has remained the cornerstone of the success of DOTS services in the country considering the length of time and limited availability of treatment options. Adherence counseling provides patients opportunity for better understanding of their health condition, enhanced provider–patient relationship, stigma reduction, and increased confidence in TB program. Furthermore, it increases frequency of provider–patient contact, which has been found to have a positive effect on TB service satisfaction and improved health outcome.4,18,19
Even though TB services were readily accessible, yet patient satisfaction score with time spent on accessing TB care was low. Low satisfaction with waiting time could be because of multiple visits (at least three visits) before commencing treatment. 20 Also, inadequacy of trained personnel to provide TB services results in increased work load for few trained staff and consequently delay in accessing care. In addition, low satisfaction with waiting time could also be due the fact that most people affected are within the economically productive age group and are engaged in one economic activity or the other, such that spending long time in DOTS facility results in high opportunity costs. 19 Opportunity costs in this context are the earnings lost or could be lost by an individual consequent upon time spent while accessing TB care. Umar et al reported that long waiting time is associated with higher economic loss to TB patients. 21 Long waiting time before accessing care has also been identified as one of the reasons TB patients do not seek care early. 20 Therefore, improving TB services should include reducing the time spent on accessing care.
Patients’ low satisfaction with amenities could be because many TB facilities particularly the public DOTS facilities are unkempt and lack basic amenities required for the comfort of the patients. Funding of TB program in the country is often not prioritized by health managers and policy makers because rather than viewing TB management and control as a public good, they consider it as a nonrevenue-yielding service.
Furthermore, most of the patients expressed low satisfaction with TB staff attitude. Provider–client relationship has been found to be a significant predictor in satisfaction with healthcare services; hence, perceived satisfaction with staff attitude is important in TB services. 22 Because TB care often involves prolonged contact between staff and client, an unfriendly attitude by health workers will likely result in low satisfaction with TB services and eventually an unfavorable outcome.
Few studies in sub-Saharan Africa have documented the effect of patients’ characteristics and health-care system on patients’ satisfaction. 23 Our study showed that except for age, no other variable was associated with overall satisfaction with TB services, an effect that disappeared following regression analysis (when it was regressed with other variables). We observed that young people have significantly lower satisfaction with registration, adherence counseling, staff attitude, and overall satisfaction. Several studies have reported higher satisfaction with various aspects of health services among older patients compared to young patients,4,24 even though few have reported otherwise. 6 Reason for this could be the different manner in which patients of different age groups are treated by care providers, such as more respectful disposition toward older patients.4,24 Difference in satisfaction among individuals from different socio-demographic backgrounds could also be explained by the variability in patient expectation. Patients with high expectations tend to be less satisfied with health services. 6 However, there is need to adapt TB services/care to meet the expectations of young people.
Gender was found to be significantly associated with both registration process and attitude of TB staff. Men in our study reported higher satisfaction scores than females. Evidence from developed countries for gender differences in mean satisfaction levels is inconsistent. While some authors reported higher satisfaction with health-care services among men, others reported the converse and few others have reported no difference. However, it is believed that any difference in satisfaction could have been influenced by frequency of utilization of services or the type of service being assessed. However, identifying the gender needs of patients accessing TB services is important in improving the quality of the NTP. 24 Marital status was also found to be statistically associated with staff attitude as those who were married reported higher satisfaction scores than others. This contrasts with what has been reported elsewhere.23,24 Higher educational status was correlated with higher level of satisfaction with staff behavior. Patients with higher education are much more likely to appreciate information and services provided by DOTS staff as well as make better informed decision to improve their health. In some cases, however, low satisfaction has been reported among patients with higher educational status because of high expectation of good services from providers.25,26
Patients who were HIV positive had greater satisfaction with access to TB services. This could be because TB–HIV coinfected patients are encouraged to access both TB and HIV services in a facility providing both services, so as to reduce the burden of accessing care on them both in terms of cost and time. Payment for TB services was associated with lower satisfaction with staff attitude, an expression that the patients were not happy with facility staff that collect money for a service that ought to be free. It could also mean that patients hold care providers responsible for any payment made for TB services. Elsewhere, incurrence of unnecessary service cost has been associated with dissatisfaction with health services. 1 On the other hand, those who paid for TB services expressed higher satisfaction with amenities in the facilities they visited and these facilities probably were private facilities. Private TB facilities are often known to have better amenities than public facilities and are allowed to charge some fees to cover operational costs, accommodation, and feeding for in-patient TB care.20,27 Living near DOTS facility was found to be associated with low satisfaction with staff attitude and amenities. Despite the significant progress made in TB management and control over the years, it has remained one of the few stigmatized disease conditions in the country. Consequently, patient's preference for treatment in facilities farther away from their residence is common. However, the NTP encourages TB patients to access care in DOTS facilities closest to them to ensure effective patient monitoring and prevent treatment interruption. In instances where stigma is a significant problem, patients may feel dissatisfied if compelled to access services in nearby facilities despite the potential benefits. In contrast to a study in Uganda, TB patients who accessed care in private facilities were less satisfied with the health education received and time spent accessing care in the facility. 6 Failure to provide adequate information to TB patients has been linked to poor treatment outcome. Previous studies have highlighted the important role private facilities play in TB control program in the country and most of them are known to provide more patient-centered services.6,27 However many of them consider TB services to be less profitable compared to other services and hence may not devote their limited time to patient education. Time constraint has been identified as one of the major reasons why health workers do not provide adequate information to TB patients. 28 It is worthy to note that the public sector has more care providers dedicated primarily to TB services than the private sector and as such are more likely to devote time and attention toward patient education. More so, there is higher attrition of trained TB workers in private facilities, resulting in provision of TB services by less skilled personnel.
Limitations
Limitations of our study include the following: first, it should be noted that since patients’ evaluations of health-care services are often subjective, it is debatable whether their ratings truly reflect technical quality or the providers’ interpersonal skills. Secondly, this study is descriptive and cross-sectional and therefore, did not capture changes in patient satisfaction over time. Studies have shown that patient satisfaction and its determinants change over time as a result of chance, measurement error, changes in societal trends in health-care attitudes, and changes in utilization patterns. In addition, the associations observed in our study should not be interpreted as causal. Thirdly, the facilities were selected purposively (nonrandomized); however, the criteria for their selection (client load, health facility type, and level) were to ensure adequate representation of the population studied. Finally, as in other studies, 24 the R2 values were low, suggesting room for improving the prediction of patient satisfaction with other variables not included here. Even though the range of possible explicative variables included in this study is large, they were not exhaustive. So, we expect, theoretically, that the absence of some of these variables may explain some of the differences in patient satisfaction observed in our study.
Conclusion
This study showed that TB patients in Nigeria were least satisfied with the attitude of DOTS staff, waiting time, and state of amenities in DOTS facilities; therefore, interventions for improving TB services in the country should focus on these aspects of the service. This can be done through training DOTS workers on providing patient-friendly services and prompt service delivery to reduce waiting time and upgrading of DOTS facilities. Also, as in previous studies, there is evidence that patient characteristics and health system factors affect patient satisfaction levels and, hence, should be taken into consideration in TB service programing.
Author Contributions
Conceived and designed the experiments: UUO, JNC, CCN, AOM. Analyzed the data: UUO, CO, JNI. Wrote the first draft of the manuscript: UUO, JNC, CCN. Contributed to the writing of the manuscript: BIO, NOM, CBD. Agree with manuscript results and conclusions: DCO, NIP, NE. Jointly developed the structure and arguments for the paper: UUO, JNC, CCN, AOM. Made critical revisions and approved final version: BIO, DCO, NIP, CBD, NE. All authors reviewed and approved of the final manuscript.