
Abstract
Little is known about the efficiency of health care in correction settings. This article reports an efficiency analysis of health care in state correctional institutions (SCIs) in a single, mid-Atlantic state from 2003 to 2006. A two-stage data envelopment analysis was used to estimate the technical efficiency of prison health care and determine inmate and institutional characteristics that were associated with efficiency. Our output variable was the number of infirmary inpatient days for each year of study. The input variable for the first stage was the sum of personnel medical staff costs and other medical operating costs. SCIs with more white prisoners, older prisoners, and higher proportions of inmates with parole violations were significantly less efficient in their provision of health care than other SCIs. There were no SCI characteristics that were predictive of efficiency. These results suggest that healthcare efficiency in corrections may decline as the prison population continues to age.
Introduction
Prisons are one of the most complex, restrictive organizations responsible for the health care of highly vulnerable individuals, and the demands for providing prison health care are increasing. 1 Harsher sentencing laws have led to more offenders’ aging in place and result in a prison population with more advanced chronic illness and more difficult healthcare needs.2,3 For example, a survey of chronic conditions from 2009 suggested that 39–43% of all inmates in federal, state, and local prisons had at least one chronic disease. 4 Furthermore, after entering the prison system, 46–69% of prisoners were taking medication for a mental health condition. 4 Such conditions are expected to increase as the number of older and elderly inmates increases, as does the financial burden to provide health care to an older and sicker inmate population.5,6
The increasing healthcare requirements of older inmates will require that prison healthcare budget be increased, prisons become more technically efficient in their provision of health care, or both. 7 Technical efficiency measures how well an organization uses its inputs (eg, nurses, infirmary beds, technology) to produce an output (eg, infirmary care). There is some literature that measures efficiency in health care outside of the prison context.8–10 These studies make comparisons of efficiency between hospitals and health systems and identify factors that are associated with efficiency.
There are no studies, however, that estimate the efficiency of health care in a prison setting. Yet given the growing, aging population and their anticipated need for more healthcare resources, there is a need to understand efficiency in the provision of health care in prisons. This study estimates the technical efficiency of health care in terms of infirmary bed days of care in the state correctional institutions (SCIs) of a single mid-Atlantic state and tests whether there are characteristics of the prison or the inmate population that are associated with efficiency.
Methods
Data
This study was part of a larger study on end-of-life care in SCIs.1,11,12 Data for this study came from all 28 SCIs in a mid-Atlantic state and were collected from a central office, which maintains an electronic database of infirmary visits for each inmate. Data from each SCI on all infirmary visits were collected for 2003–2006, including infirmary patient days, security level (low, medium, high), custody level (minimum, medium, close, maximum), population demographics, healthcare expenditures, non-healthcare expenditures, and total expenditures. SCIs without an infirmary were excluded from the analysis as were SCIs with an infirmary that served multiple prison locations (N = 7). Three SCIs lacked data for one or two years and were only excluded for those years with missing data. Therefore, the final analysis data set included a total of 19 SCIs with 71 annual measurements of infirmary days across the years 2003–2006.
Efficiency
Our efficiency analysis proceeded in two stages. In the first stage, efficiency scores were estimated using data envelopment analysis (DEA). DEA is a linear programming technique that converts multiple inputs that are required to produce an output into a single efficiency score that ranges from 0 to 1. 13 The most efficient organizations receive a score of 1. Other organizations that are less efficient receive scores less than 1, with an efficiency score proportional to their distance to the efficient frontier. Originally proposed by Charnes et al, DEA has been used to estimate efficiency in health care, prisons, and other public and private sector settings.13–16 After estimating efficiency scores for each SCI, estimated efficiency scores were modeled as a function of institutional and population characteristics using mixed-effects Tobit regression models. Tobit regression was used because the dependent variable (the efficiency score) is censored at 1, making other forms of linear regression inappropriate.
Outputs and inputs
Our output variable (outcome) for the DEA model was the number of infirmary inpatient days for each year of study. This was used in order to capture both the number of inmates who may occupy a bed in the infirmary as well as the amount of time they may occupy the bed.
Inputs for the DEA were expenditures from each SCI's budget. Three inputs were considered in the DEA: total medical costs, non-medical personnel costs, and non-medical operating costs. Total medical costs included medical staff costs and other medical operating costs in the budget of each SCI. Non-medical personnel costs included the sum of personnel administrative costs and dental costs. Non-medical operating costs were computed as the sum of operating administrative costs, operating dental service costs, and other operating costs. All costs were inflated to year 2006 using the consumer price index (CPI) for all urban wage-earners. The CPI was used because both medical and non-medical costs were included.
Statistical analysis
As mentioned above, the first step in our analysis was to estimate an efficiency score for each SCI. Next, a multiple-input DEA model was fit (assuming variable returns to scale) using the three inputs. The estimated efficiencies from this model were used as the dependent variable in the second stage of the analyses.
In the second stage, mixed-effects Tobit regression models were used to examine associations between efficiency scores and institutional and population characteristics. Because of the relatively limited sample size, separate Tobit models were fit for each characteristic. Tobit regression assumes that the efficiency scores are normally distributed but censored at some upper limit, in our case an upper limit of 1 because the most efficient prisons have a score of 1. This is necessarily a misspecification, as efficiency scores can never exceed 1. However, given the relatively small number of fully efficient data points (8 total; 11%), Tobit regression still yielded reasonable results, and is typically used in the second stage DEA. 15
In order to account for the correlated data within an SCI across years, several model specifications were tested, including linear and categorical year effects with random intercept or random intercept and slope effects. Akaike's in-formation criterion suggested the best fitting model with the simplest model, with a linear fixed effect for year and a random effect for SCI. All subsequent models for institutional and population characteristics included these years and SCI effects.
Finally, health care that is provided outside the infirmary, for example when inmates require surgical care at a nearby community hospital, is paid by the central office from a separate prison budget through an external contractor. These costs are not included in the operating costs of the SCI. Therefore, a separate analysis of these external costs was performed using a linear mixed-effects model to determine whether these external costs were associated with efficiency scores. The size of the prisoner population explained much of the variability among total external costs, and was therefore included in our model as a linear effect. Linear effects were also included for year (2003–2006) and efficiency scores. All variables included in the models were centered so that the intercept could be interpreted as the average off-site costs for an SCI in 2003 with an average prisoner population (N = 1780) and an efficiency score of 0.50. The final model also included random intercept and slopes (across years of study) for each SCI, to account for the correlation within an SCI.
Results
Among the 19 SCIs in our sample, at least 1 SCI had missing data for each year (2003–2006). For 2003, there were 17 SCIs with data, and 18 SCIs had data for years 2004–2006. Characteristics of the prison population for our sample are presented in Table 1. Most inmates were black (48–50%) and had a mean age of 35 years in 2003, rising to 36 years by the end of the sample. The average prison population rose during the study period from 1,741 in 2003 to 1,869 in 2006, although the ratio of inmates to capacity remained relatively constant.
Characteristics of prisons and prisoners in PA SCIs, 2003–2006.

Average infirmary bed days for each SCI are presented in Figure 1A. In general, the number of days was similar for a given SCI across 2003–2006, although, as seen in Figure 1A, some SCIs had variable average infirmary bed days across years.

(
As a precursor to fitting a multiple-input DEA model, we fit single-input DEA models separately for each of our inputs. Approximately six SCIs formed the efficient frontier for each input, with substantial variation in efficiency across SCIs and years. The results of these models are presented in Figure 1B–D, which shows the estimated efficient frontier for each of the three candidate inputs. There were six SCIs that were on the efficient frontier when medical costs were assumed to be the only input (Fig. 1B), six SCIs on the efficient frontier when non-medical personnel cost were assumed to be the only input (Fig. 1C), and four SCIs on the efficient frontier when non-medical operating costs were assumed to be the only input (Fig. 1D).
We next fit a multiple-input DEA model using all three cost inputs for all combinations of SCI and calendar year. The efficiency scores, one for each SCI for each year, calculated from this model for each SCI and year are shown in Table 2. The eight SCI/year combinations on the efficient frontier have a score of 1. Note the substantial variation in efficiency across SCIs. One SCI (ie, D) was on the efficient frontier for all four years. In contrast, SCI C was on the efficient frontier in 2004 but had the lowest efficiency score in 2006.
Estimated efficiencies for single output of infirmary inpatient days from multiple-input DEA model.

In the second stage of our analysis, we used these efficiency scores as an outcome in mixed-effects Tobit regression models to determine whether inmate or institutional characteristics were associated with efficient provision of health care. Since the sample was not large enough to accommodate a single Tobit model, we fit covariates one at a time. Results of each Tobit model are presented in Table 3. Three inmate characteristics were associated with healthcare efficiency: race distribution, average age, and percent of prison population with parole violations. A 10% increase in the proportion of white inmates was associated with a reduction in healthcare efficiency of 0.10 (P = 0.039). A five-year increase in the average age of the inmate population was associated with an average reduction in the efficiency score of 0.16 (P = 0.02), indicating that SCIs with older inmates tended to be significantly less efficient in terms of health care than SCIs with younger inmates. A 10% increase in the proportion of the population with parole violations was associated with an average reduction in the efficiency score of 0.16 (P = 0.011). SCIs with a higher proportion of Hispanic inmates had higher healthcare efficiency scores, but this effect was not statistically significant, and there were no institutional measures that had a statistically significant association with healthcare efficiency scores.
Results of mixed-effects Tobit regression.

Significant at the 0.05 level.
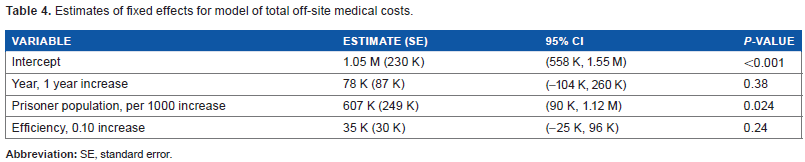
The analysis of efficiency and external healthcare costs is presented in Table 4. The size of the prison population was associated with external healthcare costs; each 1,000-inmate increase in the population was associated with approximately $607,000 in increased costs per SCI per year (P = 0.024). The effect of efficiency on external healthcare costs was not statistically significant (P = 0.24), although more efficient SCIs tended to have higher external healthcare costs.
Estimates of fixed effects for model of total off-site medical costs.
Discussion
To our knowledge, this is the first study to rigorously estimate efficiency of healthcare provision in a prison population and identify characteristics of the SCI and the inmate population that are associated with efficiency. We found substantial variation in the efficiency of health care provided at SCIs in this mid-Atlantic state. Although no SCI characteristics (eg, capacity, region, security level) were associated with efficiency of health care, a higher proportion of white inmates, an older average age, and a higher proportion of inmates with parole violations were all associated with less efficient care.
We find it difficult to explain the finding that SCIs with higher proportions of white inmates are less efficient on average, unless white inmates tend to be older, have more or more severe comorbidities, or have poorer health than other inmates. Unfortunately, we do not have data on any of these conditions at the inmate level. Certainly an assertion that, all other things equal, white patients would have more comorbidities, more severe comorbidities, or poorer health than non-white patients would run counter to current knowledge about racial disparities in health and health care in the US. We suspect, therefore, that the explanation lies in age, but our data do not provide individual level information on age, health status, or comorbidities, and we must leave this question to future research.
The finding that SCIs with older inmate populations were significantly less efficient than SCIs that housed younger inmates may have budget and policy implications for states as harsher sentencing laws drive up the average age of inmates. We also found that SCIs that were more efficient at providing care in the infirmary did not spend significantly more on health care outside of the prison on average. They did, however, spend more on average than less-efficient prisons. This may suggest that outside care is a substitute for infirmary care, and sending more inmates to receive care outside of the SCI frees resources within the SCI, making it appear more efficient. More research with a larger sample of years and SCIs would be required to parse out these effects.
For prisons, the correlation between the proportion of inmates with parole violations and efficiency means that efforts to release parole violators may increase the overall efficiency of health care in prisons. There have been efforts recently to release inmates who are incarcerated for technical parole violations, not new crimes, in order to relieve prison overcrowding. Our results suggest that efficiency of health care at some SCIs may be improved by such initiatives.
The impact of the age of the inmate population on efficiency is potentially more problematic. Many states have adopted three strikes law that mandates harsher sentences or life imprisonment after the third felony conviction. Also, in this mid-Atlantic state, as well as in many others, a life sentence comes without the possibility of parole. These policies have had the effect of increasing the age of the prison population. According to the Bureau of Justice Statistics data, 231,900 people aged 50 and older were incarcerated in the US state and federal prisons in 2011, constituting 16% of the overall prison population. 17 In addition, inmates tend to experience accelerated aging in the prison setting. 18 A previous study by Loeb et al found that the health of older male inmates was comparable to community-dwelling men who were 15 years older. 19 This chronological and premature aging may continue to erode the overall efficiency of health care in prisons without changes either to incarceration practice and policy or to interventions inside the prison to better manage the unique healthcare needs of an older inmate population. This also suggests that movements such as the Project for Older Prisoners (POPS) and the Release Aging People in Prison (RAPP) programs, which work to release older inmates who are at low risk of recidivism, may indirectly improve the efficiency of health care in prisons in addition to easing overcrowding.
We recognize several limitations to this study. First, our data come from a single state, and therefore, may not be generalizable to other states with different populations and incarceration policies and practices. Second, the data were from a state prison setting, and therefore, there may be concerns about generalizing to federal prisons or county jails, where, again, the populations may differ. Another potential limitation is that in this state, health care is provided by a mix of state employees and contracts with private sector vendors. The cost data we used only apply to the state employees. The costs for private sector vendors are paid in an omnibus fashion across all SCIs. Vendors are, however, responsible for payment of care outside the infirmary, and our analysis of off-site costs does begin to address the correlation between efficiency and these vendor costs. Finally, our study only used data through 2006. We attempted to obtain more recent data, but changes in information technology affected the measures collected over time and comparable data were not available beyond 2006. The relatively older sample was a deliberate decision to use a larger sample of older data rather than a substantially smaller sample of more recent data.
In the US, annual medical expenditures are three to eight times higher for older prisoners. 3 This may in part provide some explanation for the finding that SCIs with an older average inmate population tend to be less efficient. Perhaps, more important for all SCIs is why there is so much variation in efficiency between SCIs. We suggest that future research should focus on what the more efficient SCIs do in order to achieve greater efficiency and provide lessons for less efficient SCIs so that they may improve. Also, research should estimate determinants of efficiency in federal and county prison systems to learn whether trends identified in SCIs also hold for other correction environments.
Conclusions
In this study, we have performed an efficiency analysis of health care in a single-state prison system. There is substantial variation in the efficiency of health care provided at SCIs, but no specific SCI characteristics (eg, capacity, region, security level) were associated with efficiency of health care. However, SCIs with higher proportions of white inmates, older inmates, and inmates with parole violations were all associated with less efficient care. As prison health care budgets continue to be strained, there may be benefit to identifying the most efficient SCIs and learning what innovations allow them to provide the most infirmary bed days with the least resources.
Author Contributions
Conceived and designed the experiments: CSH, EWS. Analyzed the data: CSH, EWS. Wrote the first draft of the manuscript: CSH, EWS, SJL. Contributed to the writing of the manuscript: CSH, EWS, SJL, JP, CAS. Agree with manuscript results and conclusions: CSH, EWS, SJL, JP, CAS. Jointly developed the structure and arguments for the paper: CSH, SJL, JP, CAS. Made critical revisions and approved final version: CSH, EWS, SJL, JP, CAS. All authors reviewed and approved of the final manuscript.
Footnotes
Acknowledgment
The assistance of Nicholas Scharff, MD, of the Pennsylvania Department of Corrections is gratefully acknowledged for facilitating access to the data.