
Abstract
Many teaching hospitals employ a care team structure composed of a broad range of healthcare providers with different skill sets. Each member of this team has a distinct role and a different level of training ranging from attending physician to resident, intern, and medical student. Often times, these different roles lead to greater complexity and confusion for both patients and nursing staff. It has been demonstrated that patients have a great degree of difficulty in identifying members of their care team. This anonymity also exists between nursing staff and other care providers. In order to better understand the magnitude of anonymity within the teaching hospital, a ten-question survey was sent to nurses across three different departments. Results from this survey demonstrated that 71% of nurses are “Always” or “Often” able to identify which care team is responsible for their patients, while 79% of nurses reported that they either “Often” or “Sometimes” page a provider who is not currently caring for a given patient. Furthermore, 33% of nurses felt that they were either “Rarely” or “Never” able to recognize, by face and name, attending level providers. Residents were “Rarely” or “Never” recognized by face and name 37% of the time, and interns 42% of the time. Contacting the wrong provider repeatedly leads to de facto delays in medication, therapy, and diagnosis. Additionally, these unnecessary interruptions slow workflow for both nurses and members of the care team, making hospital care less efficient and safe overall. Technological systems should focus on reducing anonymity within the hospital in order to enhance healthcare delivery.
Keywords
Today's healthcare system is large and complex. Experts believe complexity may be at least two-fold higher in healthcare than in any other industry. 1 This complexity arises in part from the many technologies, physical infrastructure, cognitive challenges, unpredictable patient needs, and diverse workforce requirements that characterize modern care. While clinical teams have long been central to the structure of care delivery within teaching hospitals, there has been a substantial increase in the complexity of human interactions required to provide care. Each member of a typical care team has a distinct role, different level of training, and a variable degree of visibility to patients and other providers. Duty hour restrictions for trainees have resulted in more rotating physicians working in a 24-hour period, more hand-offs of care, and increased fragmentation of relationships between team members. 2 Previous studies have demonstrated that hospitalized patients have a great degree of difficulty identifying members of their care team. 3 This anonymity poses a unique problem to the healthcare industry. In other industries–-for example, online retail–-customers can receive efficient, effective, low-cost delivery of goods without any interaction or knowledge of employees working behind the scenes. Healthcare, however, requires visible and available human relationships because illness is not only a pathophysiological event requiring logistical and technical management, but also represents an existential crisis during which human interaction is expected. In medicine, ethical frameworks have always highlighted the experience of illness and healing, but the quality and safety movement has only recently begun to emphasize discreet measurement of the patient experience. Patient satisfaction and confidence in care teams within hospitals is now tied to re-imbursement as part of the federally supported Hospital Consumer Assessment of Healthcare Providers and Systems (HCAPHS) surveys.4,5
Compounding the problem of anonymity are the current information technology systems available within hospitals, which rely on paging systems and fragmented silos of information. A number of reported quality improvement projects have focused on reducing the number of erroneous pages sent to physicians, which likely helps streamline communication between nurses and physicians, simultaneously making care coordination easier, faster, and more reliable.6–8 Based in part on these findings, a number of initiatives have been proposed to improve both professional communication and the technology used between clinicians and nursing staff.9,10
As part of a local quality improvement project, we recently explored the interaction between our information technology systems and anonymity within care teams at our large academic medical center. University of Colorado Hospital, a teaching affiliate of the University of Colorado Anschutz Medical Campus, is a 467-bed facility that handles 22,589 admissions, 740,640 outpatient visits, and 65,895 emergency room visits annually. For patients receiving care from internal medicine and related subspecialty services, approximately 130 physician trainees rotate on 19 distinct teams (11 different teams on the med/surg units, 4 dedicated cardiovascular care teams, and 4 distinct intensive care teams). Each team often cares for patients spread across many different geographic locations and floors within the hospital.
To ascertain the degree of difficulty, nurses have contacting teams and identifying different members on those teams, we distributed a 10-question electronic survey to nurses (Table 1). Nurses were instructed to define how often they knew which team was assigned to their patients, and how often they were able to identify, by face and name, members of the care team using a standard, five-point Likert scale. Of the 230 nurses who received the survey, 178 responded (77% response rate). There were 94 respondents from the general medicine units (med/surg), 39 respondents from the cardiovascular care units, and 45 respondents from the medical intensive care units (MICU, Fig. 1).
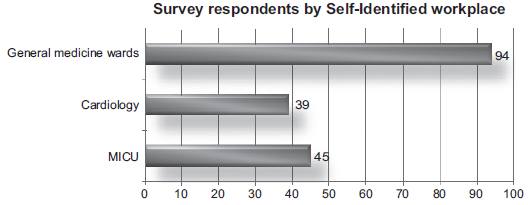
Total survey respondents (n = 178) categorized by workplace; general internal medicine units (med/surg), cardiovascular units (cardiology), and MICU.
The majority of nurses (71%) reported they “always” or “often” knew which care team was assigned to their patients (Fig. 2). However, approximately four out of five nurses (79%) stated they “often” or “sometimes” page a provider who is not currently caring for their patient (Fig. 3). This represents a very high process failure rate for contacting the correct provider and leads to inefficiencies in communication. A consequence is de facto delays in care, as nurses repeat work in order to contact the correct physician. In addition, physicians endure unnecessary interruptions and are contacted about patients they don't know, slowing workflow for all providers.

Survey question number 1, asking nurses to rate how often they knew which team was the team caring for the patient.

Survey question number 3, asking nurses to rate how often they page a provider not caring for the patient.
A 10-question electronic survey was sent to nurses across three different departments. Nurses were instructed to answer using a standard, five-point Likert scale ranging from “always” to “never” or “strongly agree” to “strongly disagree,” depending on the question. Question 10 asked nurses to identify the unit/department in which they typically work.

Our survey also captured the degree of anonymity between physicians and nurses caring for the same patient. When asked to rate their ability to identify the attending physician, by face and name, 33% of nurses felt that they were either “rarely” or “never” able to do so. For residents and interns, the corresponding rates were 37 and 42%, respectively (Fig. 4). Residents, with their rotating schedule, likely introduce more anonymity than attending level providers.

Summary of questions 4, 6, and 7, in which nurses were asked how often they are able to identify (by face and name) the attending, resident, and intern physician on the care team.
Interestingly, there was variability in anonymity between different types of units. Medical intensive care nurses reported they could “always” identify attending providers 58% of the time, whereas nurses on cardiology and med/surg units could “always” identify the attending physician only 18 and 2% of the time, respectively. The work environment accompanying intensive care likely explains this difference. Often times, attending providers are physically in the intensive care unit and, arguably, play a more visible role in the care of critically ill patients than do attending physicians outside the intensive care unit. In addition, the cohort of intensivists at our institution is smaller than the cohort of attending cardiologists and general internists. However, 38% of intensive care nurses still reported they “often” paged the wrong provider with a clinical question. This error rate, especially in the intensive care unit, undermines patient safety and slows hospital efficiency.
Some studies have attempted to decrease hospital anonymity by placing photos of care providers in patients’ rooms, and most medical centers have policies requiring all personnel to visibly wear identification. 11 While our data do not refute the worthiness of such initiatives, we believe the problem of anonymity requires systems redesign that goes well beyond checklists outlined in etiquette-based medicine (eg, consistent personal introductions, making ID badges visible, and explaining one's role). 12 After all, how can patients, in a weakened state of health, or family and friends, in the midst of a stressful inpatient hospitalization, be expected to recognize members of their care team when nurses, who work daily alongside care providers, have the same difficulties? While a greater push toward personal introductions during each shift would certainly be beneficial, the geographic dispersion of care teams throughout the hospital requires a technological solution that connects care team members to one another more transparently and reliably. Indeed, more than 90% of nurses who completed our survey either “strongly agreed” or “agreed” that optimizing the IT system at our hospital, in order to reduce anonymity within the care teams, would make their work easier and care more efficient (Fig. 5).

Survey question number 8, asking nurses to rate how they agreed that reducing anonymity would make nursing jobs easier.
There are limitations to this study. The survey did not take into account both the length of employment and the hours worked by the nurses, which may have introduced bias. For instance, nurses with a shorter duration of employment at our hospital might not have been as familiar with care providers as nurses with many years of employment. However, based on the severe degree of anonymity and the reported failure rate of our process for identifying and contacting the correct physician, duration of employment or nighttime versus daytime shift work is unlikely to substantially alter the implications of our results. In addition, our data are drawn from a single academic center, which relies on a particular paging system (Amion) that many hospitals may not use. Finally, as our data are descriptive, we did not perform rigorous statistical analysis of responses over time or nuances between large subgroups. Such analysis will be important to evaluate future quality improvement interventions based on our initial findings.
This perspective does not offer a simple solution to the pervasive anonymity within modern hospitals, but our hope is that it broadens the conversation. We must think deeply about how to make hospitals more efficient and safe, while at the same time decreasing anonymity. This will not be easy, as doing so requires accounting for the human factors of healthcare, current information technology, and hospital culture when designing solutions to improve and enhance healthcare delivery. Simply imploring healthcare workers to collaborate more frequently with one another without providing technology solutions that make it easier to do so will not suffice.
Author Contributions
Conceived and designed the experiments: DK, RP. Analyzed the data: DK, RP. Wrote the first draft of the manuscript: DK. Contributed to the writing of the manuscript: DK, RP. Agree with manuscript results and conclusions: DK, RP. Jointly developed the structure and arguments for the paper: DK, RP. Made critical revisions and approved final version: DK, RP. All authors reviewed and approved of the final manuscript.