
Abstract
Currently, in the United States there is a significant physician workforce shortage. This problem is likely to persist as there is no quick solution. The nature of this shortage is complex and involves factors such as an absolute physician shortage, as well as physician shortages in primary care and certain specialty care areas. In addition, there is a misdistribution of physicians to medically underserved areas and populations. The medical education system trains medical school graduates that eventually feed the physician workforce. However, several factors are in place which ultimately limits the effectiveness of this system in providing an appropriate workforce to meet the population demands. For-profit medical schools have been in existence in and around the continental US for many years and some authors have suggested that they may be a major contributor to the physician workforce shortage. There is currently one for-profit medical school in the US, however the majority exist in the Caribbean. The enrollment in and number of these schools have grown to partially meet the ever-growing demand for an increase in medical school graduates and they continue to provide a large number of graduates who return to the US for postgraduate medical training and, ultimately, increase the physician workforce. The question is whether this source will benefit the workforce quality and quantity needs of our growing and aging population.
Introduction
The US health care delivery system is comprised of at least five components: cost, quality, accessibility, maintenance of the medical education system, and availability of a well trained physician workforce, all of which are being threatened by major challenges. 1 Among these challenges is the high cost of health care, the concern for consistent high quality medical services coupled with increased safety concerns, and lack of accessibility to primary care and specialty physicians in specific urban and rural areas. Additionally, the medical education system, long based on a not-for-profit university based model, which advocated fewer schools and a rigorous curriculum, and produced fewer, but well-trained physicians, does not meet the expanding population's need for more doctors and questions the current model of the physician education and training system.
Of particular importance is the issue of physician supply and availability. Currently, there is a significant physician workforce shortage in the US for which there is no “quick” solution. 1 The size, demographics, specialty choice, and practice locations and patterns of the physician workforce are the outcome of current and past decisions made by individual physicians. Their decisions were influenced by many factors including personal choice, market forces, State and Federal policies and programs, and institutions which constitute the health care system and medical education infrastructure. 2 Thus, the nature of our physician shortage is remarkably complex.
As of January 2013, there were 5,900 designated Primary Care Health Profession Shortage Areas, defined by the US Department of Health and Human Services Health Resources and Services Administration as a physician to population ratio of 1:3,500. 3 The physician workforce is unevenly distributed throughout the US and pockets of severe shortages occur primarily in poor, rural, and inner-city areas.
The demand for an increasing number of physicians is also fueled by many factors including population growth, the aging population, changes in medical insurance coverage and type (including the impending implementation of the Affordable Care Act's Health Insurance Marketplace in 2014), economic growth, technological advances, and government policy.
New additions to the physician workforce (including both US and international medical graduates (IMGs)) and the rate of attrition (whether through retirement, death, or disability) determine the supply of active, practicing physicians. Physicians enter practice in the US through one of three routes: graduation from a US allopathic or osteopathic school of medicine, or graduation from an international medical school. One effort within the US to address the workforce shortage has been the expansion of medical school class size and the establishment of new medical schools. US medical schools are on track to increase their enrollment thirty percent by 2017. 4 Concurrent to these efforts has been the increase in the number of ‘for-profit’ schools, particularly in the Caribbean, but now including the US. The concept of for-profit medical schools has been a source of controversy since their inception; however, many can agree that the advantage of these schools is to augment the medical education system by adding more physician providers.
The medical education system is complex as well, in that it encompasses both medical school education and residency training, each governed by its own oversight body. The Association of American Medical Colleges (AAMC) is the oversight organization of medical school education. The Liaison Committee on Medical Education (LCME), jointly sponsored by the AAMC and the Council on Medical Education of the American Medical Association (AMA), accredits undergraduate allopathic medical schools. The Accreditation Council for Graduate Medical Education (ACGME) and the American Board of Medical Specialties (ABMS) oversee different aspects of the graduate medical education system. The AAMC represents the 141 accredited US and 17 accredited Canadian medical schools. Additionally, the AAMC impacts roughly 400 major teaching hospitals and health systems, including 51 Department of Veterans Affairs medical centers, and nearly 90 academic and scientific societies. The AAMC represents 128,000 faculty members, 75,000 medical students, and 110,000 resident physicians. 5 In regards to osteopathic medicine, the American Osteopathic Association (AOA) represents the 29 accredited colleges of osteopathic medicine and oversees the Osteopathic Graduate Medical Education (OGME) as well. Both ACGME and OGME postdoctoral training programs are recognized by the Center for Medicare and Medicaid Services, meaning that such programs receive funding from Medicare and Medicaid. Contributing to the complexity of the overall system is the addition of IMGs and for-profit medical schools (including the Caribbean medical schools) to the pool that feeds resident physician training. This complex system is vital in supplying a well-trained physician workforce. The purpose of this manuscript is to define the role of for-profit medical schools in augmenting the US health care delivery system through its contributions to the medical education system and physician workforce.
For-profit Medical Schools
In order to address the potential impact of for-profit medical schools on the current and future physician workforce, it is important to review their history and evolution. The nation's first medical schools (University of Pennsylvania, Harvard, and Yale, to name a few) were university-based teaching hospitals. Shortly after their openings, in the early 1800s, the first for-profit medical school was established in Baltimore. Over the course of the next century, many more schools came into existence, both university-based and for-profit. The majority in fact, were for-profit; only one-third of the 155 medical schools at the beginning of the 20th century were not-for-profit university-based models. 6 Substandard medical care punctuated this time in US history; lax admission standards, perfunctory testing, the absence of clinical rotations, and the lack of licensing boards contributed to the poor quality of physicians produced in this era. With the founding of Johns Hopkins University School of Medicine in 1893, the practice of medicine was revolutionized. By applying unprecedented standards to medical training, the education of physicians in the US was forever changed. Rigid entrance requirements were established and the curriculum emphasized scientific methods as well as bedside teaching and laboratory research. While other schools followed suit, many continued to adhere to the old standards of medical education, including the for-profits. During this time Abraham Flexner, an American educator, was commissioned by the Carnegie Foundation to compile a report on the medical education system. In 1910, he presented his report titled Medical Education in the United States and Canada: A Report to the Carnegie Foundation for the Advancement of Teaching. In this report, Flexner noted that too many poorly trained physicians were the end product of a multitude of commercial medical schools.
“Such exploitation of medical education is strangely inconsistent with the social aspects of medical practice… The medical profession is an organ differentiated by society for its highest purposes, not a business to be exploited”. 7
He opposed the for-profit medical school concept, instead favoring a university-based system and advocated for fewer medical schools producing quality, well-trained physicians. Flexner's report was a seminal event in the history of American medical education. This standardization, which occurred in the early 1900's, resulted in the last for-profit medical school in the continental US to close in 1930. 8
It is important to attempt to define a “for-profit school” as there are several types. The first type is known as an educational management organization (EMO), which utilizes public funds in conjunction with school districts and charter schools to support primary and secondary education (K-12). The other main type of for-profit schools are those of higher education, including universities, colleges and academies, and trade and vocational schools that award academic degrees or professional certifications. For-profit medical schools fall under this category. Simply put, for-profits are in business to be profitable for owners and shareholders by offering a service, in this case education.
Since the Flexner era, for-profit medical schools have been met with resistance. To combine the words “for-profit” and “medical school” can be considered an enigma. The obvious main concern is whether a for-profit medical school could sustain the altruistic commitment to medical education, in the face of financial challenges. Thus, the term “for-profit medical school” remains contradictory in the eyes of many. Several attempts to reinstitute a for-profit medical school in the US have been challenged and defeated, including a business venture in 1999 by Ross University School of Medicine in Wyoming (a for-profit allopathic medical school with roots on the Caribbean island of Dominica). To date, we have seen the establishment of one proprietary medical school in the continental US. A large majority of the international for-profits reside in the Caribbean.
Rocky Vista University College of Osteopathic Medicine
Currently, there is one for-profit medical school in the US. Founded in 2006, Rocky Vista University College of Osteopathic Medicine (RVUCOM) in Parker, CO is fully accredited by the American Osteopathic Association's Commission on Osteopathic College Accreditation (AOACOCA). Their mission statement reads: “Rocky Vista University provides quality healthcare education while inspiring students to serve with compassion, integrity, and excellence”. Academic admission requirements are similar to other allopathic and osteopathic medical schools, requiring a baccalaureate degree with prerequisite coursework, minimum GPA requirements, and Medical College Admission Test (MCAT) scores.
From an educational standpoint, critics have expressed concern over the lack of academic teaching hospitals associated with the medical school. 9 Clinical rotations are completed at various hospitals throughout the state of Colorado and the Mountain West. Third and fourth year medical students in their clerkships could be sent for rotations to nonacademic community hospitals without a strong background in education and research. Proponents argue that Rocky Vista must adhere to the same educational standards as all other accredited, non-profit allopathic and osteopathic schools and will maintain the same educational outcomes. 10 They state that the change lies in the structure of medical education and does not reflect a subsequent change in curriculum, clinical training, or research.
From a monetary standpoint, critics claim that RVUCOM will be indebted to its investors, and as a result educational quality will be sacrificed. 11 If standardized test scores are a reflection of educational quality, this appears to not be the case. RVUCOM reports a 97% COMLEX-I pass rate and a 98% COMLEX-II pass rate, purportedly amongst the top in the nation for osteopathic schools. 12 The 2012 COMLEX-I and COMLEX-II pass rates among osteopathic schools was 92.6% and 90%, respectively. 13 The founder of Rocky Vista, Florida businessman Yief Tien, remains on the Board of Trustees as does his wife; the scope of independence and influence of this situation remains unclear. Of note, Tien also served as Chief Operating Officer of the American University of the Caribbean in St. Maarten until 2011 and was formerly the President and Director of Medical Education Administrative Services, Inc. The school's auditing firm projected no return on the initial 100 million dollar investment for several years and stated that it will take seventeen years alone to break even. 9 Indeed, in the 2008 fiscal year, approximately two years after the institution's inception, RVUCOM incurred a loss of $9.9 million. 14 By the 2011 fiscal year, RVUCOM had noted a profit of $4.5 million. 15 By these numbers, it will no doubt take some time for RVUCOM to break even.
The 2013–2014 tuition rate for first year medical students is $46,742; the total cost of attendance for the first year (tuition, health insurance, books, supplies, room and board, etc…) is estimated at $77,064. For Colorado residents, the total estimated cost of a four-year medical education at Rocky Vista is $305,490. 16 While certainly not the most expensive of the osteopathic medical schools, it is on the high end according to 2012–2013 cost of attendance data from the American Association of Colleges of Osteopathic Medicine (AACOM). 17 Like other medical schools, RVUCOM participates in Federal student aid programs and students finance their medical education through a combination of federal and private loans, scholarships, and personal contributions. In 2012, RVUCOM's average indebtedness was $199,000. 17 The education section of U.S. News & World Report in 2010 surveyed 112 medical schools (both allopathic and osteopathic), which reported an average medical school indebtedness of $145,020. 18 The majority of schools with the heaviest debt burden of over $200,000 were largely private not for-profit medical schools. Roughly 80% of RVUCOM's revenue, as with the other private osteopathic medical schools, comes from tuition and fees. In contrast, tuition and fees comprise only 14% of public osteopathic medical schools’ revenue. 15
RVUCOM inaugural class of 2012 match results.

Caribbean medical schools
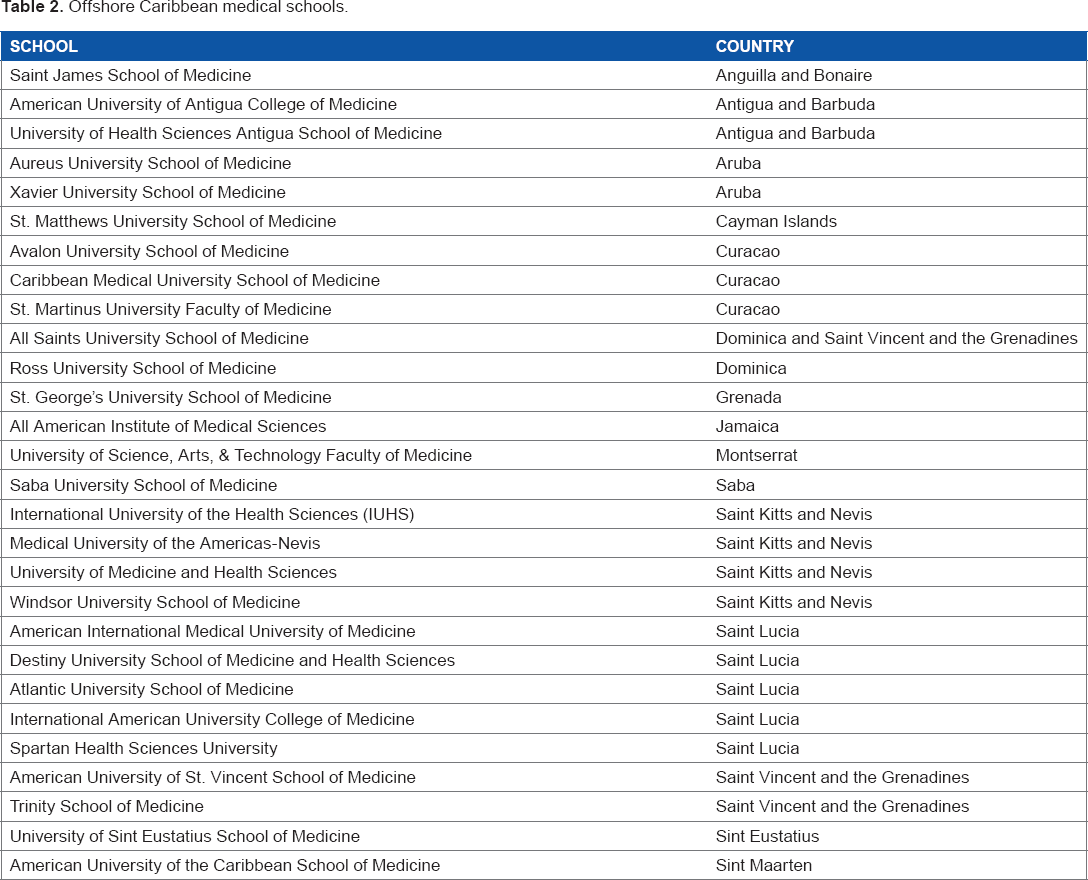
As mentioned, the majority of for-profit medical schools exist in the Caribbean. While other international for-profit schools attract US citizens, the sheer number of schools, the close proximity to the US, and the commonality of the English language draws many US medical students to the Caribbean. Unlike domestic schools, these schools also recruit and cater to the international populations, although the majority of students come from the US. The Caribbean medical school trend began in the 1970s and was spearheaded by American entrepreneurs and medical professionals who addressed the need for medical education which could not be met domestically. This trend has continued as progressively more for-profit medical schools have opened across the Caribbean over the past several decades. Remarkably, forty percent of these schools have been established since 2000. 21 St. George's University, Ross University, American University of the Caribbean, and Saba University Schools of Medicine represent a few of the more established medical schools in the region, having opened in the 1970s or 1980s. Many newer medical schools, including the American University of St. Vincent and of Barbados, All Saints, and Atlantic University Schools of Medicine have opened in the last two or three years alone.
Offshore Caribbean medical schools.
The offshore medical school supply has emerged in part to meet the ever-growing demand for an increase in medical school graduates (and ultimately an increase in the physician workforce). Additionally, Caribbean medical schools are often more appealing to those who view an allopathic Doctor of Medicine (M.D.) degree as more valuable than a stateside acquired osteopathic Doctor of Osteopathic (D.O.) degree, as all degrees awarded from these programs carry the title of Doctor of Medicine. While tuition rates in offshore for-profit medical schools may be high, the cost may be equivalent to or less than that of a private institution in the United States. Similar to RVUCOM in Colorado and other medical schools in the US, many Caribbean medical schools participate in Federal student aid programs. These schools also tend to attract those students who are unable to gain acceptance into US medical schools for various reasons, such as poor scores on standardized testing (i.e., the MCAT) or low undergraduate GPA's. Educational standards vary, and admissions criteria are often less stringent than those required from US schools. For example, some schools such as the American University of Antigua (AUA), the International American University (IAU) College of Medicine, and the Caribbean Medical University do not require the MCAT. Thus, acceptance rates are higher than average and class sizes are often much larger than their US counterparts. St. George's University, in Grenada, had 554 entering students for the 2013 spring enrollment, and each incoming class at Ross University in Dominica accepts approximately 350 students (there are several classes a year). As some of the oldest medical schools in the Caribbean, St. George's and Ross each have approximately 10,000 medical graduates. It is likely that the attrition rate is high given each school's relatively long history (St. George's was established in 1976, Ross in 1978). Other applicants choose Caribbean schools simply because they are one of many highly qualified applicants vying for a limited number of medical school slots in a state with strong competition.
Historically, investors interested in offshore ventures were able to develop profit-generating institutions that were subject to much less stringent oversight from local authorities than in the US. A business license might be all that is required to open an offshore medical school, compared to the highly regulated financial and academic governance for a new medical school in the US. However, since the establishment of the Caribbean Accreditation Authority in 2003, steps have been made to oversee “quality control” across programs in the Caribbean. Nevertheless, it is still difficult to ensure standardization, as the accreditation process is voluntary. As of June 2012, only eleven schools had subjected themselves to accreditation reviews and four have received full accreditation. 22 The World Education Services, a non-profit organization that provides research about international education, does not consider offshore for-profit medical schools equivalent to accredited US medical schools as more time is needed to determine educational quality at these institutions. 23 Thirty years ago, studies demonstrated that US IMGs did not perform as well on standardized tests as did graduates of US medical schools. 24 A more recent study, analyzing the performance of physicians who attended Caribbean medical schools, showed considerable variation in quality indicators, including ECFMG and specialty board certification rates. 25
The structure of medical education in the Caribbean today varies widely by school and country. United States Medical Licensing Exam (USMLE) scores are a good reflection of this. The USMLE is a 3-part test (Step 1, Step 2, which is divided into a Clinical Knowledge (CK) and Clinical Skills (CS) portion, and Step 3) that assesses a physician's medical knowledge applied to clinical skills that are fundamental in providing safe and effective patient care. A physician must pass the exams before being permitted to practice medicine in the US. Step 1 is usually taken after the first two years of basic science studies and just prior to starting clinical rotations. The Step 2 exams are taken during the last year of medical school, and Step 3 is taken following the completion of medical school. According to 2012 USMLE performance data for Step 1, first time test takers from the US and Canadian schools have a 96% pass rate, while the pass rate from non-US schools, including the Caribbean, is 76%. Similarly, the first time pass rate for Step 2 CK and CS amongst American and Canadian schools is 98% and 97%, respectively, while non-US schools have an 85% and 80% pass rates, respectively. 26
The question remains whether the quality of medical education in the Caribbean, from adequate teaching facilities equipped with up to date clinical teaching tools and research facilities to an educationally challenging curriculum taught by qualified instructors, is comparable to US medical schools. 27 As direct patient care is limited on the islands, and given the sheer number of medical students, many schools have multiple affiliations with hospitals throughout the US for third and fourth year medical students in their clinical rotations. In New York for example, the number of students rotating from Caribbean medical schools almost equals the number of students from the state's own medical schools. 28
Historically, US IMG match rates are much lower than those of US graduates and are illustrated in Figure 1. For US allopathic seniors, 93.7 % were matched to post graduate year (PGY) positions in 2013. Match rates have historically ranged from 92%–94%.
29
Only 53.1% of US IMGs matched in 2013, however, and this marked the highest match rate since 2005 (Table 3).
PGY-1 Match Rates by Applicant Type, 1982–2013.a Applicants in the matching program 2009–2013.
a
Data from NRMP.
29
Copyright permission obtained from National Resident Matching Program, Results and Data: 2013 Main Residency Match. National Resident Matching Program, Washington, DC. 2013.

Physician Workforce
Currently, there is a significant physician workforce shortage in the US for which there is no easy solution. 1 The impact of for-profit medical schools on physician workforce could play a role in minimizing this shortage, however the limiting factor remains that graduates of offshore Caribbean schools often face great difficulty in securing a residency position through the US-based National Resident Matching Program (NRMP). It is generally accepted that many residency directors in the US prefer US medical graduates to IMGs. The end result is that these students may go unmatched, or settle for a residency position that does not fulfill their career goals. Candidates must have an Educational Commission for Foreign Medical Graduates (ECFMG) certification, which requires completion of USMLE Step 1 and both portions of USMLE Step 2 as well as a medical degree from an institution that is registered with the International Medical Education Directory (IMED). The ECFMG certification ensures that IMGs are prepared to enter ACGME training programs in the US. US medical students need not have their medical diplomas to enter the match during their final year of medical school. Thus, stateside trained graduates can begin residency right after graduation, whereas IMGs must wait several months before starting training due to the cyclical nature of the match process.
The NRMP recently released data from the 2013 main residency match. 29 Of 26,392 PGY-1 positions available, 25,463 positions were filled. US medical school seniors filled 16,390 (64%) of the positions. US IMGs, including the for-profit medical schools in the Caribbean, filled 2,706 (10.6%) of the positions. Non-US IMGs filled 3,601 (14%) of all available positions. 29
Matches by specialty and applicant type, 2013. a

Data from NRMP. 29
Copyright permission obtained from National Resident Matching Program, Results and Data: 2013 Main Residency Match. National Resident Matching Program, Washington, DC. 2013.
Because of the overall physician workforce shortage, it has been suggested that a partial solution could be recruitment of IMGs from other countries (defined as non-US IMGs). However, students from for-profit medical schools also represent an option. In addition, physician assistants and nurse practitioners are working to fill the gap and have helped to compensate for the physician workforce shortfall.
The medical education system educates medical school graduates in primary care or specialty areas that eventually feed the physician workforce. While there is a push to expand existing medical schools or start new medical schools, the reality is that there is no effort by the Federal Government to increase the number of residency positions. It is important to note that the vast majority of funding for resident training comes from the Department of Health and Human Services, primarily through Medicare. There has been a moratorium on all new resident positions funded through the Federal Government since the Balanced Budget Act of 1997. Thus, the number of government funded residency positions has been capped for 16 years at this point. Historically, hospitals funded the training of residents before Medicare subsidies existed and some hospitals now fund some residency training slots. This accounts, however, for only a marginal increase in residency positions.
As a result, there will not be enough positions for all medical school graduates and the need to increase the physician workforce will not occur at a rate to meet the demand. The annual Medical School Enrollment Survey, conducted by the AAMC's Center for Workforce Studies, found that 40% of medical school deans were extremely concerned about enrollment growth outpacing the number of available residency training positions. 4 In the 2013 match, there were more unmatched US seniors than unfilled positions. This disturbing statistic has happened only once before, in 2010. 4 AAMC President and CEO Dr. Darrell G. Kirch's statement on this issue reflects the need for urgency in the call to increase residency positions:
“We're pleased to see our nation's medical schools increasing enrollment to address the projected physician shortage, but as we saw in the results of this year's Match, Congress now needs to do its part and act quickly to increase the number of federally funded residency training positions in order for all medical school graduates to be able to complete their training and become practicing physicians.” 4
Thus, unless the Federal Government works to lift the cap on residency training positions, the plethora of medical school graduates, from for-profits or otherwise, will not be able to impact on the growing gap between the physician workforce and the public need.
Conclusion
The availability of a well-trained physician workforce and maintaining the medical education system are just two of several components of the health care delivery system that are intricately linked. In order to effect change in one, great efforts at modification and revision must be made in the other. For-profit medical schools represent a novel, albeit controversial, approach to solving this dilemma. The impact of the only for-profit medical school in the US remains to be seen. Offshore for-profit medical schools, including those in the Caribbean, continue to provide a large number of medical school graduates who return to the US for postgraduate medical training. However, these students are also subject to the same residency caps that have and will continue to affect the number of available residency training positions in the US. In the meantime, we will continue to face the challenges of supply vs. demand in providing a well-trained, adequate physician workforce to a US population that should have ready access to quality healthcare.
Author Contributions
Wrote the first draft of the manuscript: JMB, BDB. Contributed to the writing of the manuscript: JMB, BDB, MZS. Agree with manuscript results and conclusions: MZS. Jointly developed the structure and arguments for the paper: JMB, BDB, MZS. Made critical revisions and approved final version: JMB, BDB, MZS. All authors reviewed and approved of the final manuscript.
Footnotes
As a requirement of publication the authors have provided signed confirmation of their compliance with ethical and legal obligations including but not limited to compliance with ICMJE authorship and competing interests guidelines, that the article is neither under consideration for publication nor published elsewhere, of their compliance with legal and ethical guidelines concerning human and animal research participants (if applicable), and that permission has been obtained for reproduction of any copyrighted material. This article was subject to blind, independent, expert peer review. The reviewers reported no competing interests. Provenance: the authors were invited to submit this paper.