
Abstract
The metabolism of arachidonic acid by either the cyclooxygenase (COX) or lipoxygenase (LOX) pathway generates eicosanoids, which have been implicated in the pathogenesis of a variety of human diseases, including cancer. It is now considered that they play important roles in tumor promotion, progression, and metastasis, also, the involvement of COX and LOX expression and function in tumor growth and metastasis has been reported in human tumor cell lines. In this study, we examined the expression of COX and LOX in human urological tumors (renal cell carcinoma, bladder tumor, prostate cancer, testicular cancer) by immunohistochemistry and RT-PCR, and we also examined the effects of COX and LOX (5- and 12-LOX) inhibitors in those cells by MTT assay, hoechest staining, and flow cytometry. COX-2, 5-LOX and 12-LOX expressions were significantly more extensive and intense in malignant tissues than in normal tissues. Furthermore, 5-LOX inhibitor induced the reduction of malignant cell viability through early apoptosis. These results demonstrated COX-2 and LOX were induced in urological tumors, and 5-LOX inhibitor may mediate potent antiproliferative effects against urological tumors cells. Thus, 5-LOX may become a new target in the treatment of urological tumors.
Keywords
Introduction
Angiogenetic factors play important roles in urological tumors as well as in other cancers. In recent years, the expression of angiogenic factors in solid human tumors has been widely reported [1]. Growth factors secreted by tumor cells such as fibroblast growth factor, and transforming growth factor, have increased neovascularization
COX is the first enzyme in the pathway for producing prostaglandin (PG) and thromboxane (Tx) from arachidonic acid, and can occur as three isoforms, COX-1, COX-2 and COX-3. The enzymes of both COX-1 and COX-2 are transformed from the cell membrane phospholipid to arachidonic acid by the phospholipaseA2, and then transform arachidonic acid to PGH2 through PGG2 (Fig. 1). COX-1 occurs in tissues and cells and works to protect the cell. COX-2 express momentarily and strongly in response to growth factors and some endotoxins. It is involved with inflammation, cell proliferation and differentiation [3]. COX-2 has also been shown to play an important role in carcinogenesis. Although the existence of COX-3 has recently been reported, it continues to be argued [4].
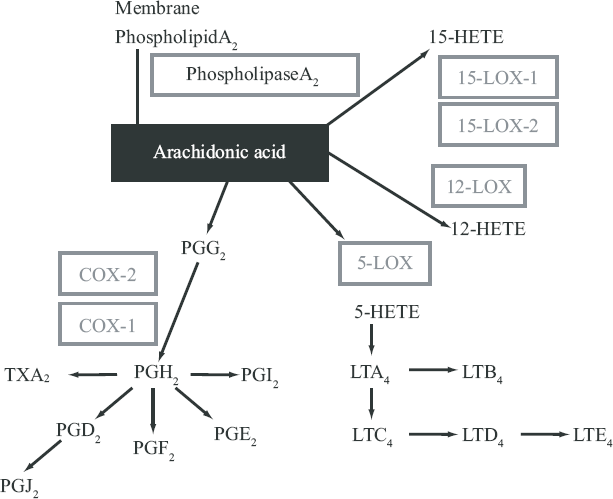
LOX is the first enzyme in the pathway for producing leukotrienes (LT) from arachidonic acid. Isoenzymes of LOX include 5-LOX, 12-LOX and two 15-LOX isoforms (15-LOX-1, 15-LOX-2). These catalyze the biosynthesis of biologically active compounds such as LTs and hydroxyeicosatetraenoic acids (HETEs) [5,6]. 5-LOX catalyzes the first step in oxygenation of arachidonic acid to produce 5-hydroperoxyeicosatetraenoic acid (5-HPETE), and the subsequent metabolism of 5-HPETE to 5-HETE and LTs (Fig. 1). LTs belong to an important group of proinflammatory mediators that are synthesized from arachidonic acid via the 5-LOX pathway. The activity of 5-LOX leads to the formation of unstable LTA4, which can be converted into either LTB4, or cysteinyl LTs (LTC4, LTD4 and LTE4) [7].
The 12-LOX, includes platelet 12-LOX, and leukocyte 12-LOX that oxygenate arachidonic acid at position C-12 to produce 12-hydroperoxyeico-satetra- enoic acid and then 12-HETE [8]. Whereas 5-LOX, 12-LOX and 15-LOX-1, have procarcinogenic roles, 15-LOX-2 appears to have an anti-carcinogenic roles.
Our research focuses on the relationship between COX-2 and LOX (5- and 12-LOX) and urological tumors (renal cell carcinoma, bladder tumor, prostate cancer and testicular cancer) and on the antitumor effects of COX and LOX inhibitors.
Methods
Tumor specimens
All tissue specimens were obtained from Osaka City University Hospital. Tumor tissues, nontumor tissues, vascular endothelium, and interstitial tissues from the subjects were preserved in 10% formalin and embedded in paraffin, serially sectioned onto microscope slides at a thickness of 4 μm.
a) COX
Renal cell carcinoma (RCC) specimens
Specimens were obtained from 108 patients with RCC and 20 patients with normal kidney (NK) tissues who underwent total nephroureterectomy due to ureteral cancer.
Bladder tumor (BT) specimens
Specimens were obtained from 118 patients with BT (including 68 who underwent total cystectomy and 50 who underwent transureteral resection of bladder tumor) and 10 patients with chronic cystitis (CC) and 8 with normal bladder tissues (NB) who underwent total prostatectomy because of prostate cancer.
Prostate cancer (PC) specimens
Specimens were obtained from 28 patients with PC, 8 patients with benign prostatic hyperplasia (BPH), 1 patient with prostatic intraepithelial neoplasia (PIN) who underwent total prostatectomy or subcapsular prostatectomy, and 8 patients with normal prostate (NP) tissues who underwent total cystectomy because of bladder tumor.
Testicular cancer (TC) specimens
Specimens were obtained from 72 patients with TC, 20 patients with normal testis (NT) tissues who underwent orchiectomy for prostate cancer.
b) LOX
RCC specimens
Specimens were obtained from 50 patients with RCC and 10 patients with NK tissues.
BT specimens
Specimens were obtained from 170 patients with BT (87 total cystectomy and 83 transureteral resection) and 20 patients with CC and 20 patients with NB tissues.
PC specimens
Specimens were obtained from 174 patients with PC, 20 patients with BPH, 20 patients with PIN, and 8 patients with NP tissues.
TC specimens
Specimens were obtained from 72 patients with TC, 20 patients with NT tissues.
Immunohistochemical staining
Immunohistochemical staining was performed with a Vectastain (vector Laboratories, Burlingame, California) avidin-biotin preoxidase complex kit, as previously described [9]. Primary antibodies against rabbit COX-1 (DHHILHVAVDV) (1:100 dilution in PBS), rabbit COX-2 (LDDINPTVLLKER) (1:100 dilution in PBS), rabbit 5-LOX (Cayman Chemical, Ann Arbor, Michigan) (1:100 dilution in PBS), rabbit 12-LOX (Oxford Biomedical Research, Oxford, Michigan) (1:100 dilution in PBS) and control PBS were used.
Immunohistochemical analysis
Staining was classified into 5 grades from 0 to 4 according to staining intensity and number of positive cells by two blind observers on two separate occasions using coded slides. An average score was calculated.
A 4 grade indicated that all staining was maximally intense throughout the specimen, while 0 indicated that staining was absent throughout the specimen. Micro-anatomical staining sites were also recorded. This method was perfomed as previously described [9]. All results are presented as the mean ± SD. Data analysis were performed using ANOVA [10].
PT-PCR
Concerning COX, total RNA was extracted from RCC, BT, PC and TC tissues. Concerning LOX, total RNA was extracted from RCC tissues, BT and PC cell lines by the acid guanidium thiocyanate-phenol-chloroform method [11].
a) COX
For Polymerase Chain Reaction (PCR) analysis of RNA, complementary DNA (cDNA) was made by reverse-transcription of 2 μg of each RNA sample using Super Script preamplification system for first-strand cDNA synthesis (GIBCO BRL, MD, U.S.A.). PCR reactions were performed with 3 μl of each cDNA, 3 μl of each sense and antisense primers (20 μM), and 1 unit of Taq polymerase (NIPPON GENE, Toyama, Japan). 35 cycles of denaturation, annealing, and extension (94°C for 45 sec, 54 °C for 45 sec, and 72 °C for 2 min) were performed on automatic heat-block (Model PJ2000 DNA Thermal cycler, PERKIN ELMER, NJ, U.S.A.).
The primers used were:
Human COX-1 sense (5‘-TGCCC AGCTCCTGGCCCGCCGCTT-3’) and antisense (5‘-GTGCATCAACACAGGCGCCTCTT C-3’);
Human COX-2 sense (5‘-TTCAAATGAGATTGTGGGAAAATTGCT-3’) and antisense (5‘-AGATCATCTCTGCCTGAGTATCTT-3’); Human glyceraldehyde 3-phosphate dehydrogenase (G3PDH) sense (5‘-CCACCCATGGCAAATTCCATGGCA-3’) and antisense (5‘-TCTAGAGGGCAGGTCAGGTCCACC-3’).
b) LOX
After the RT reaction, nested PCR was used to examine 5- and 12-LOX mRNA expression. For 5- and 12-LOX, the first run PCR profile was 94 °C, 15s to denature; 61 °C, 30s for annealing and extension for 30 cycles with upstream (5‘-CTTCCCGTGCTACCGCTG-3’) and downstream (5‘-TGGGGTTGGCACCATTGAG-3’) primers. 5 μl of first run PCR product was used for the nested PCR with the profile of 94 °C, 15s to denature; 61 °C, 30s for annealing and extension for 25 cycles with nested primers (upstream 5‘-CCAGGAGACAATGCTTTGGACA-3’; downstream 5‘-GAACAACTCATCATCCTGCCAG-3’).
Reagents and materials
RPMI 1640 was purchased from Nissui Pharmaceutical Company (Tokyo, Japan), fetal bovine serum (FBS) and penicillin-streptomycin mixture from Biowhitteker (Walkerville, MD), and trypsin/EDTA from GIBCO BRL (Rockville, MD).
Ibupurofen, Piroxicam, Meloxicam, and Nimesulide were obtained from BIOMOL Research Laboratories INC (U.S.A.), Naproxen was obtained from Cayman Chemical Company (St. Louis, U.S.A.), Indomethacin and NS 398 were obtained from Wako Pure Chemical Industries Ltd (Osaka, Japan), and Etodolac was obtained from Nippon Shinyaku Co. Ltd (Kyoto, Japan). Ibupurofen, Piroxicam, Meloxicam, Nimesulide Naproxen, Indomethacin, NS 398, and Etodolac were all COX inhibitors.
5-LOX inhibitor (Caffeic acid) and 12-LOX inhibitor (Baicalein) were obtained from BIOMOL. Research Laboratories Inc, U.S.A. Nonspecific LOX inhibitor (NDGA) was obtained from Cayman Chemical, U.S.A. All data characteristics of these inhibitors were published in their product information.
Cell cultures
The human RCC cell line (Caki-1) and normal prostate stromal cell were provided by Dr. Shinichi Ikemoto (Dept. of Urology, Osaka City University School of Medicine, Osaka, Japan). The human BT cell line (T24), PC cell lines (PC3, DU-145), TC cell line (NEC-8) and normal proximal tubular endothelial cell (PRTEC) were obtained from Health Science Research Resources Bank (Osaka, Japan). Normal bladder cell line was obtained from the patients with normal bladder tissues who underwent total prostatectomy due to prostate cancer.
Cells were grown in culture flask (Nunc, Roskilde, Denmark) in RPMI 1640 supplemented with 10% FBS, 100 U/ml of penicillin and 100 μg/ml of streptomycin in a humidified 5% CO2 atmosphere at 37 °C. The media were changed every 3 days and the cells were separated via trypsinization, using trypsin/EDTA when they reached subconfluence.
Cell proliferative studies
Approximately 1.0 × 104 cells placed onto 8 × 8 mm diameter multichamber slides (Nunc, Copenhagen, Denmark) were treated with COX and LOX inhibitors (10–80 μM) dissolved in ethanol. The final concentration of ethanol was <0.05%. Cell viability was measured after 48 hours by a microplate reader using a modified 3-[4,5-dimethylthiazol-2-thiazolyl]-2, 5- diphenyltetrazolium bromide (MTT) assay (WST-1 assay; Dojindo, Kumamoto, Japan) and presented as the percentage of control-culture conditions.
Flow Cytometry (Annexin V and propidium iodide staining)
The effects of LOX inhibitors on human urological tumors cell lines were determined by dual staining with Annexin V-FITC and propidium iodide using Annexin V-FITC Apoptosis Detection Kit I (Biosiences Pharmingen). Annexin V-FITC and propidium iodide (PI) were added to the cellular suspension as in the manufacturer's instruction, and sample fluorescence of 1.0 × 104 cells was analyzed flow cytometry. Flow cytometry was with FACScan (Becton Dickinson, Germany). Cell which were Annexin V-FITC positive and PI negative were identified as early apoptosis. Cell which were Annexin V-FITC positive and PI positive were identified as late apoptosis or necrosis.
Flow Cytometry (Identification of DNA fragmentation)
The assay was performed by TdT-mediated dUTP Nick End Labelling (TUNEL) method using APO-DIRECT™ kit (Becton Dickinson, Germany). Following the experiments, human urological tumors cell lines in suspension (1 × 106/ml) were fixed with 1% PBS, washed in PBS, and suspended in 70%(v/v) ice-cold ethanol. The cells were stored in ethanol at –20 °C until use. The positive and negative controls and the sample were stained with FITC-dUTP by incubation in terminal deoxynucleotidyl transferase buffer as in the manufacturer's instruction, and sample fluorescence of 1 × 104 cells was analyzed by flow cytometry (Becton Dickinson, Germany). Results are given as % of TUNEL-positive cells.
Detection of apoptosis by Hoechst staining
DNA chromatin morphology was assessed using hoechst staining. Human urological tumors cell (5 × 105 cells) were incubated with 50 μM LOX inhibitor for 24 hour. Cells were washed by RPMI-1640 and labeled with 8 mg/ml of hoechest 33342 (Sigma-Aldrich Japan K.K. Tokyo, Japan) for 10 min; PI (Sigma-Aldrich Japan K.K. Tokyo, Japan) was added (10mg/ml final concentration), and the cells were examined by fluorescence microscopy.
Results
Expression of COX and LOX
1) Immunohistochemistry
a) COX
RCC tissue sample
COX-2 expression was observed in proximal and distal tubules of NK tissues. However, in epithelial cells, blood vessels and stromal tissues, while COX-2 was not expressed in NK tissues, COX-2 was strongly expressed in all RCC tissues.
BT tissue sample
COX-1 was weakly expressed in CC tissues but no expression was found in any BT tissues. On the other hand, COX-2 was strongly expressed in all BT tissues with an intense expression in high-grade BT group. Neither COX-1 nor COX-2 were expressed in NB tissues.
PC tissue sample
The expression of COX-1 was very weak in PC, PIN, BPH and NP tissues. However, COX-2 was strongly expressed in all PC tissues, although very weak expression of COX-2 was found in PIN, BPH and NP tissues.
TC tissue sample
COX-1 and COX-2 were strongly expressed in all TC group tissues, although very weak expression of COX-1 and COX-2 were found in NT tissues.
b) LOX
RCC tissue sample
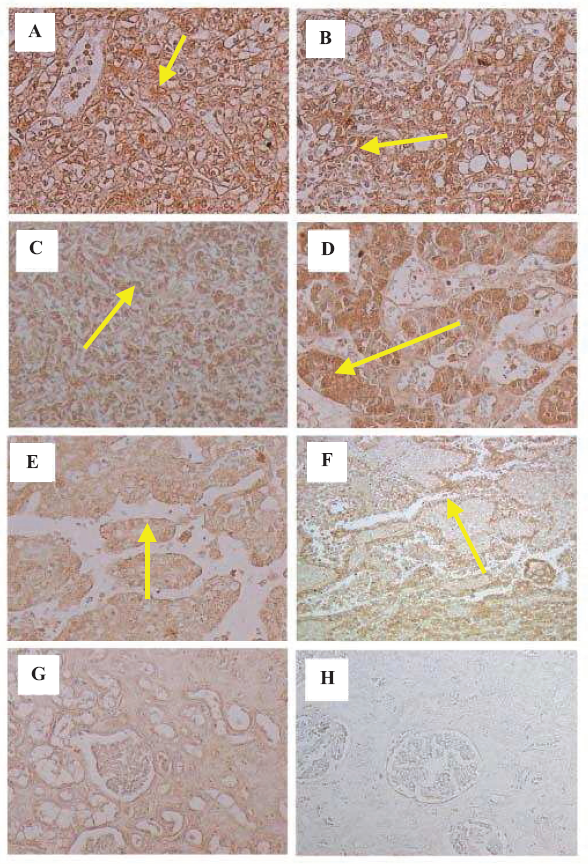
5- and 12-LOX were strongly expressed in all grades RCC tissues (A: RCC -G1, B: RCC -G2, C: RCC -G3) and other types of RCC tissues (D: RCC papillary cell type, E: RCC chromphobe cell type, F: RCC collecting duct type) although very weak expressions of 5- and 12-LOX were found in NK tissues (G). Immunostaining with PBS was negative (H) (Fig. 2).
BT tissue sample
5- and 12-LOX were strongly expressed in all grades of BT tissues, although very weak expressions of 5- and 12-LOX were found in CC and NB tissues.
PC tissue sample
5- and 12-LOX were strongly expressed in all grades of PC and PIN tissues, although very weak expressions of 5- and 12-LOX were found in BPH and NP tissues.
TC tissue sample
5- and 12-LOX were strongly expressed in all TC group tissues, although very weak expressions of 5- and 12-LOX were found in NT tissues.
Statistical analysis of immunohistochemistry
a) COX
RCC tissue sample
We classified 3 categories (epithelium, blood vessel, a small quantity of stromal tissue) in RCC tissues, and examined them for intensity of COX-2 immunostaining. COX-2 expression score was significantly more extensive and intense in all categories of RCC tissues than NK tissues. COX-2 expression score was higher in G1 cancer than in G3 cancer. However, no difference was seen in all categories among grades. Another comparison between stages, the expression score was higher in early stage cancer pT1 than in advanced cancer (pT2 or above). However, this comparison among stages also shows no significant difference among the categories.
BT tissue sample
We classified 3 categories (epithelium, blood vessel, stromal tissue) in BT tissues, and examined them for intensity of COX-1 and COX-2 immunostaining.
COX-2 expression score was significantly more extensive and intense in epithelial cells of BT and CC than in epithelial cells of NB. COX-2 expression score was higher in G3 cancer than in G1 cancer. Moreover, the expression score was higher in advanced cancer (pT2 or above) than in early stage cancer (pT1 or below). On the other hand, no difference was seen in blood vessels and stromal tissues between NB and BT tissues.
PC tissue sample
We classified 3 categories (epithelium, blood vessel, stromal tissue) in PC tissues, and examined them for intensity of COX-1 and COX-2 immunostaining.
COX-2 expression score was significantly more extensive and intense in epithelial cells of all grades PC tissues than in BPH and PIN tissues. On the other hand, COX-2 expression score was high in the blood vessels, and the stromal tissues of PC in the study groups with no significant difference between grades. However, COX-2 expression score in the blood vessels and stromal tissues from BPH, PIN and NP were at basic level.
TC tissue sample
We classified 2 categories (epithelium, blood vessel) in TC tissues, and examined them for intensity of COX-1 and COX-2 immunostaining.
COX-1 expression score was significantly more extensive and intense in all categories of TC tissues than in NT tissues. COX-2 expression score was also significantly more extensive and intense in all categories of TC tissues in the studied groups than in NT tissues. However, there were no significant differences among the five histopathological groups in all categories.
b) LOX
RCC tissue sample
We classified 3 categories (epithelium, blood vessel, a small quantity of stromal tissue) in RCC tissues, and examined them for intensity of 5- and 12-LOX immunostaining.
5- and 12-LOX expression scores were significantly more extensive and intense in all categories of RCC tissues than NK tissues. Only in epithelium, 5- and 12-LOX expression scores were higher in G1 cancer than in G3 cancer. However, no differences were seen in blood vessels and stromal tissues among the three grades.
BT tissue sample
We classified 3 categories (epithelium, blood vessel, stromal tissue) in BT tissues, and examined them for intensity of 5- and 12-LOX immunostaining.
5- and 12-LOX expression scores were significantly more extensive and intense in BT tissues than in CC and NB. A significant difference was seen only in epithelium, showing that staining was intensified as the grade increased. No difference was seen in blood vessels and stromal tissues between grades.
Comparison of early and advanced stages shows a significant difference only in epithelium. No difference was seen in blood vessels and stromal tissues between early stage (pT1 or below) and advanced cancer (pT2 or above).
PC tissue sample
We classified 3 categories (epithelium, blood vessel, stromal tissue) in PC tissues, and examined them for intensity of 5- and 12-LOX immunostaining.
5- and 12-LOX expression scores were significantly more extensive and intense in PC and PIN tissues than BPH and NP tissues in all categories. There was no significant difference between grades.
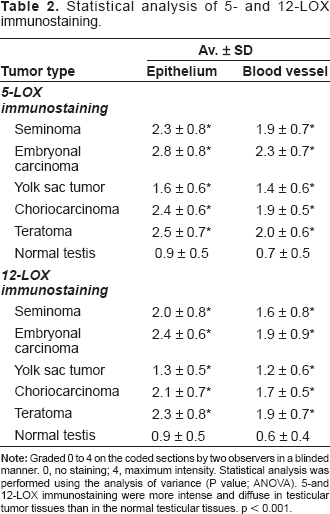
TC tissue sample
We classified 2 categories (epithelium, blood vessel) in TC tissues, and examined them for intensity of 5- and 12-LOX immunostaining.
Effects of COX and LOX inhibitors in viabity of human prostate cancer and normal prostate stromal cells.
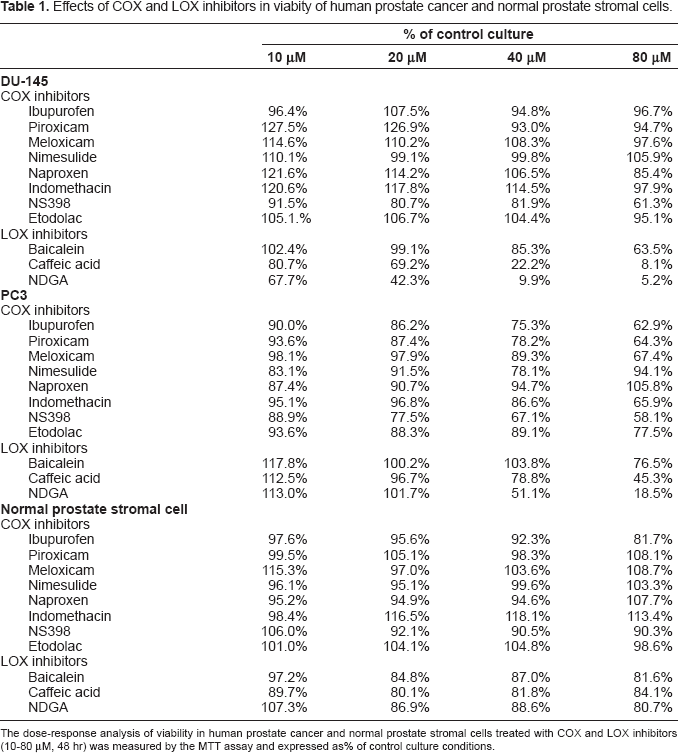
The dose-response analysis of viability in human prostate cancer and normal prostate stromal cells treated with COX and LOX inhibitors (10–80 μM, 48 hr) was measured by the MTT assay and expressed as% of control culture conditions.
RT-PCR
a) COX
RCC tissue
We detected a specific band of COX-2 mRNA band in RCC, whereas sample of from NK displayed no band of COX-2 mRNA.
BT tissue
We detected specific band of COX-1 mRNA in all samples (BT, CC and NB). However, we detected specific band of COX-2 in BT, while a weak band was displayed in CC and no clear band was displayed in NB.
PC tissue
We detected a specific band of COX-1 mRNA in all samples (PC, BPH and NP). However, we detected a specific band of COX-2 was detected in PC, while a weak band was displayed in BPH and no clear band was displayed in NP.
TC tissue
We detected a specific band of COX-1 and COX-2 mRNA all TC groups.
b) LOX
RCC tissue
We detected a specific band of 5- and 12-LOX mRNA in RCC, whereas the sample of from NK displayed no band of–-and 12-LOX mRNA.
BT cell line
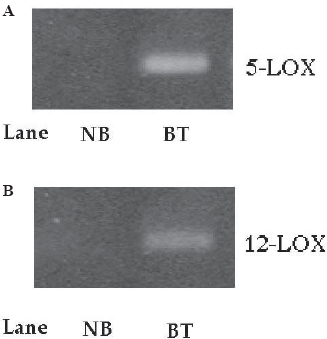
We detected a specific band of 5- and 12-LOX mRNA (A: 5-LOX, B: 12-LOX, lane 2) in BT cell line, whereas the sample of from NB cells displayed no band of–-and 12-LOX mRNA (A: 5-LOX, B: 12-LOX, lane 1) (Fig. 3).
PC cell line
We detected a specific band of 5- and 12-LOX mRNA in PC cell line, whereas a sample of from NP cells displayed no band of–-and 12-LOX mRNA.
2) Effect of COX and LOX inhibitors MTT assay
a) COX
RCC cell line
All COX inhibitors were unable to induce a reduction of cell viability with the half-maximal concentration of growth inhibition of RCC cells in the range of 10–80 μM and were unable to stop the growth of RCC cells. All COX inhibitors had no effect on normal proximal tubular endothelial cells (PRTEC) proliferation.
BT cell line
Similar to RCC cells, COX inhibitors could not induce a reduction of cell viability with the half-maximal concentration of growth inhibition of BT cells in the range of 10–80 μM and could not stop the growth of BT cells. COX inhibitors had no effect on normal bladder cells proliferation.
PC cell line
Statistical analysis of 5- and 12-LOX immunostaining.
TC cell line
Regarding RCC, BT and PC cells, some forms of COX inhibitors induced a slight reduction of TC cells growth in 80 μM, but we were unable to detect the induction of TC cells apoptosis in 80 μM COX inhibitors.
a) LOX
RCC cell line
LOX inhibitors induced a reduction of cell viability with the half-maximal concentration of growth inhibition of RCC cells in the range of 10–80 μM. Although the effect of non-specific LOX inhibitor was strongest, the effect of 5-LOX inhibitor was stronger than that of 12-LOX inhibitor. No LOX inhibitors had any effect on normal proximal tubular endothelial cells (PRTEC) proliferation.
BT cell line
Similar to RCC cells, LOX inhibitors induced a reduction of cell viability with the half-maximal concentration of growth inhibition of BT cells in the range of 10–80 μM. Although the effect of non-specific LOX inhibitor was strongest, the effect of 5-LOX inhibitor was stronger than that of 12-LOX inhibitor. No LOX inhibitors had any effect on normal bladder cells proliferation.
PC cell line
Similar to RCC and BT cells, LOX inhibitors induced a reduction of cell viability with the half-maximal concentration of growth inhibition of PC cells in the range of 10–80 μM. Although the effect of non-specific LOX inhibitor was strongest, the effect of 5-LOX inhibitor was stronger than that of 12-LOX inhibitor. No LOX inhibitors had any effect on normal prostate stromal cells proliferation (Table 2).
TC cell line
Similar to RCC, BT and PC cells, LOX inhibitors induced a reduction of cell viability with the half-maximal concentration of growth inhibition of TC cells in the range of 10–80 μM. Although the effect of non-specific LOX inhibitor was strongest, the effect of 5-LOX inhibitor was stronger than that of 12-LOX inhibitor.
3) Apoptosis effect of LOX inhibitor
a) Flow cytometry
RCC cell line
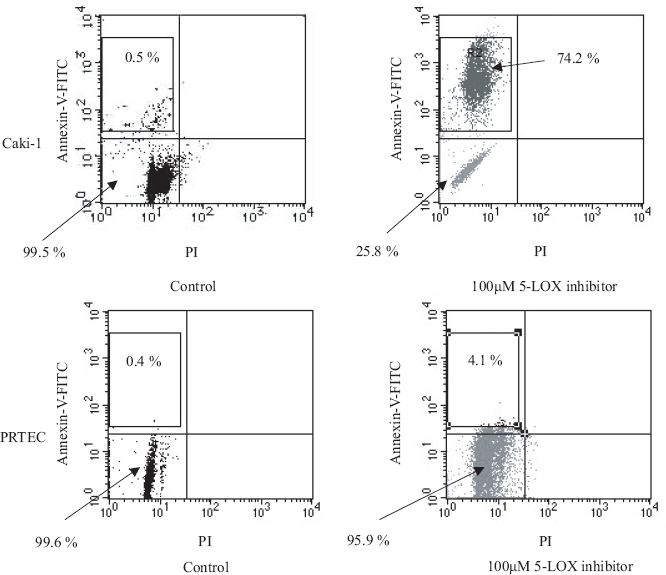
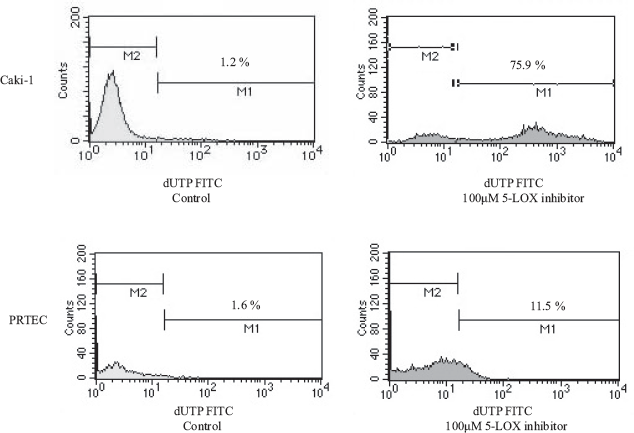
RCC cells treated with 100 μM 5-LOX inhibitor could induce early apoptosis, not late apoptosis or necrosis and DNA fragmentation. However, treated with 100 μM 5-LOX inhibitor did not induce apoptosis in normal proximal tubular endothelial cellss (PRTEC). Diagram of FITC-Annexin V/PI flow cytometry (Fig. 4) and typical flow cytometry analysis histogram are presented (Fig. 5).
BT cell line
Similar to RCC cells, BT cells treated with 100 μM 5-LOX inhibitor could induce early apoptosis, not late apoptosis or necrosis and DNA fragmentation.
PC cell line
Similar to RCC and BT cells, PC cells treated with 100 μM 5-LOX inhibitor could induce early apoptosis, not late apoptosis or necrosis and DNA fragmentation.
TC cell line
Similar to RCC, BT and PC cells, TC cells treated with 100 μM 5-LOX inhibitor could induce early apoptosis, not late apoptosis or necrosis and DNA fragmentation.
2) Hoechest staining
RCC cell line
RCC cells treated with 50 μM 5-LOX inhibitors caffeic acid, and non-specific LOX inhibitor NDGA showed chromatin condensation, cellular shrinkage, small membrane-bound bodies (apoptotic bodies), and cytoplasmic condensation. Cells with 12-LOX inhibitor baicalein showed the same apoptotic changes slightly. In contrast, untreated cells maintained normal chromatin patterns and cell size.
BT cell line
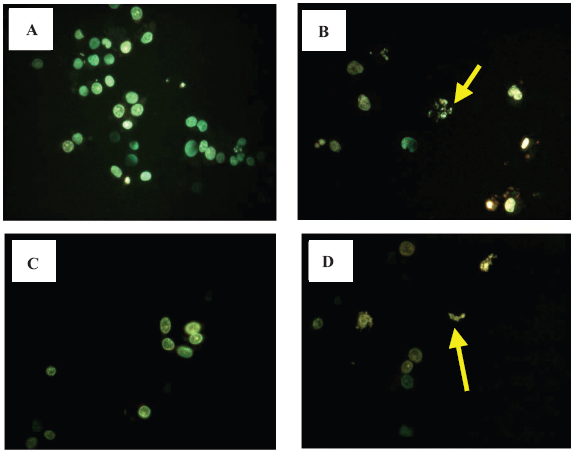
Similar to RCC cells, BT cells treated with 50 μM 5-LOX inhibitors caffeic acid (B), and non-specific LOX inhibitor NDGA (D) showed chromatin condensation, cellular shrinkage, apoptotic bodies, and cytoplasmic condensation. Cells with 12-LOX inhibitor baicalein (C) showed the same apoptotic changes slightly. In contrast, untreated cells maintained normal chromatin patterns and cell size (A) (Fig. 6).
PC cell line
Similar to RCC and BT cells, PC cells treated with 50 μM 5-LOX inhibitors caffeic acid, and non-specific LOX inhibitor NDGA showed chromatin condensation, cellular shrinkage, apoptotic bodies, and cytoplasmic condensation. Cells with 12-LOX inhibitor baicalein showed the same apoptotic changes slightly. In contrast, untreated cells maintained normal chromatin patterns and cell size.
TC cell line
Similar to RCC, BT and PC cells, TC cells treated with 50 μM 5-LOX inhibitors caffeic acid, and non-specific LOX inhibitor NDGA showed chromatin condensation, cellular shrinkage, apoptotic bodies, and cytoplasmic condensation. Cells with 12-LOX inhibitor baicalein showed the same apoptotic changes slightly. In contrast, untreated cells maintained normal chromatin patterns and cell size.
Discussion
With recent increases in routine medical check-ups and progress in diagnostic imaging techniques, the discoveries of RCC have risen. The cause of RCC is unknown. RCC generally does not respond well to radiotherapy and chemotherapy compared to many other types of cancers, and anticancer drugs as interleukin-2 is used with relative success. Surgery is currently the only therapeutic option. Hence, new molecular targets are needed for the treatment and prevention of RCC.
The natural history of BT is not well understood, but exposure to carcinogens, including aromatic amines, is considered a major risk factors for the development of BT. Workers exposed to aromatic amines frequently have a mutated p53 gene, a tumor suppressor gene involved in the carcinogenesis of many tumors.
PC comprises 32% of all cancers in American men and is on the rise worldwide. Because of increased screening, PC is frequently diagnosed at a clinically localized stage, making it amenable to the therapy. Nevertheless, it remains the second most common cause of cancer death in men. These patients generally respond to androgen deprivation therapy, but the vast majority eventually experience disease progression and become refractory to sustained hormonal manipulation. Typically, such patients progress with a rise in their serum prostate-specific antigen level. Unfortunately, standard therapeutic options at this stage of disease are limited, and while there has been some success with chemotherapy for hormone-refractory PC patients, the response is generally short-lived [12].
TC is very rare with over 90% of all TC being germ cell tumors (seminoma and non-seminoma), and the remaining percentage non-germinal tumors. The survival rate of TC has improved in recent years, reflecting the development and refinement of effective combination chemotherapy. However, it is still necessary to improve the treatment of TC.
Non-steroidal anti-inflammatory drugs (NSAIDs) have anti-tumor effects on human urological tumors (RCC, BT, PC and TC) and have attracted a great deal of attention. The typical target of NSAIDs is COX. In recent reports, a number of patients have had significantly low-risk of colorectal cancer while they continued using NSAIDs typified by aspirin. Consequently, the suppression of carcinogenesis by administering NSAIDs has come into focus. It was also reported that the size and number of adenoma were markedly reduced when sulindac which is a type of NSAIDs was given to patients with the familial adenomatous polyposis, a high risk group for colorectal cancer [13].
Regarding COX-2 in RCC, BT and PC, COX-2 expression in malignant tissues was stronger than that in normal tissues using immunohistochemical staining and RT-PCR [9,14,15].
Both COX-1 and COX-2 expressions in all tissue types of TC were stronger than those in normal tissues using immunohistochemical staining and RT-PCR [16]. Both COX-1 and COX-2 expressions appeared stronger in all tissue types of TC possibly due to the amount of PG increased in TC. Evidence revealed the PG quantity increased in breast cancer tissue compared to normal breast tissue and the expression of both COX-1 and COX-2 increased [17].
Many publications have reported COX-2 expression in malignant tissue was stronger than in normal tissue, and COX-2 expression in malignant tissue was stronger than COX-1 expression in malignant tissue. However, the correlation between the grade or stage, and COX-2 expression can be argued.
Although many papers have reported NSAIDs produce anti-tumor effects, our studies confirmed that eight kinds of COX inhibitors were unable to induce reduction of the viability in human urological tumors cells in the range of 10–80 μM by MTT assay [18].
Our results suggest COX-2 expression is strong in treating urological tumors, but the antitumor effect of COX inhibitor (including COX-2 inhibitor) is very weak in urological tumor patients in a single administration at a clinical dose. COX-2 inhibitor is suitable for chemopreventive therapy.
Regarding 5- and 12-LOX in urological tumors, 5- and 12-LOX expressions in malignant tissues were stronger than those in normal tissues using immunohistochemical staining and RT-PCR [8,19–21]. Similar to COX-2, the correlation between the grade or stage, and LOX expression can be argued.
Furthermore, LOX inhibitor (particularly 5-LOX inhibitor) could induce reduction of the viability in human urological tumors cells in the range of 10–80 μM by MTT assay. The effect of 5-LOX inhibitor was stronger than that of 12-LOX inhibitor [22]. Furthermore, urological tumors cells treated with 5-LOX inhibitor could induce early apoptosis and DNA fragmantation in urological tumors cells using flow cytometry and hoechest staining.
Several papers have reported LOX inhibitors to be targets for development of new chemopreventive or chemotherapeutic strategies for PC. Ghosh J et al. reported that inhibition of arachidonate 5-LOX triggers massive apoptosis in both androgen-sensitive (LNCaP) and androgen-refractory (PC3) human PC cells [23]. Furthermore, Ghosh J also reported the metabolites of arachidonate 5-LOX promoted survival of PC cells involving down-regulation of stress-activated protein kinase [24]. Pommery N et al. reported dual COX-2/5-LOX inhibitors induced agents potentially useful in PC chemotherapy through apoptosis [25]. Ghosh J also reported the combination of selenium and 5-LOX inhibitors may be a more effective regimen for PC control [26].
Research strongly suggests LOX expression is strong in urological tumors, but the anti-tumor effect of 5-LOX inhibitor is weak in urological tumor patients receiving a single administration at a clinical dose. 5-LOX inhibitor is suitable as a chemo-preventive therapy.
In conclusion, it is clear that COX-2 and LOX (particularly 5-LOX) are involved in the initiation and promotion of urological tumor tissues. It may be possible to use COX-2 and LOX inhibitors as anti-tumor drugs from the viewpoint of preventing cancer. However, it may be difficult to use the COX-2 inhibitor or 5-LOX inhibitor at the clinical dose with expectation of a suppressive effect on the cancer. Although the clinical application of 5-LOX inhibitor requires further research and consideration, the target of 5-LOX is a novel strategy in the treatment of human urological tumors.
Footnotes
Acknowledements
This manuscript was edited by Hilah Edney, BS, MS.