
Abstract
Sternal wound infections represent one of the most frequent complications after cardiac surgery and are associated with high postoperative mortality. Several preventive methods have been introduced, and recently, gentamicin-impregnated collagen sponges (GICSs) have shown a promising effect in reducing the incidence of this type of complications. Gentamicin is an aminoglycoside antibiotic that has been widely used to treat infections caused by multiresistant bacteria; despite its effectiveness, its systemic use carries a risk of toxicity. GICSs appear to overcome this side effect, topically delivering high antibiotic concentrations to the wound and thus reducing the toxic-related events. Although several retrospective analyses and randomized controlled trials have studied the use of GICSs in cardiac surgery, conclusions regarding their efficacy in preventing sternal wound infection are inconsistent. We have reviewed the current literature focusing on high-risk patients.
Introduction
Microbiology of SWIs.
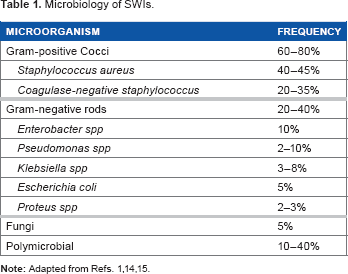
The emergence of multiresistant bacterial strains has led to a challenging situation: beta-lactam antibiotics have become ineffective against most CoNS and S. aureus clusters, and the routine use of vancomycin as a prophylactic agent is not advisable in order to avoid further antibiotic resistances.13,16 Furthermore, CoNS have the intrinsic ability to adhere to foreign bodies (eg, sternal wires) and produce a biofilm, thus increasing their resistance to antibiotics and the probability of a chronic infection.17,18
Advantages of Gentamicin Local Delivery
Local administration of antibiotics such as gentamicin, tobramycin, tetracycline, minocycline, teicoplanin, and sulbactam–cefoperazone has been performed in several surgical fields. 8 Gentamicin has gradually become the most used molecule for this purpose due to a combination of characteristics such as broad spectrum, low cost, and favorable pharmacokinetics and pharmacodynamics when administered topically.8,19
Gentamicin is an aminoglycoside antibiotic that has been widely used to treat infections caused by multiresistant bacteria (Fig. 1). Although its spectrum is mainly directed toward gram-negative species, gentamicin is also effective against several gram-positive strains.
19
Furthermore, gentamicin also shows a synergy with beta-lactam antibiotics, especially against gram-positive species such as S. aureus and CoNS.
16
Nevertheless, the principal factor limiting its systemic use is represented by its intrinsic toxicity; when administered intravenously or intramuscularly, gentamicin accumulates into renal cortex and into endolymph and perilymph of the inner ear, causing kidney injury and hearing loss.
20
These drawbacks can be partially eluded by administering gentamicin locally, reducing the systemic toxicity. Kidney and inner ear accumulations seem to appear when gentamicin serum concentration exceeds 10–12 mg/L, although a precise cutoff has not been established.8,21 Interestingly, it has been observed that, after local administration in the sternal region, the drug serum concentration does not exceed 1 mg/L, while mediastinal fluid concentration remains above 300 mg/L for 36 hours.
21
Moreover, gentamicin exhibits a concentration-dependent effect, especially against gram-negative rods: this means that a high concentration of the drug circumscribed to the surgical site can lead to a bactericidal effect not only toward sensitive bacteria but also toward poorly sensitive or even resistant ones;
20
an acute peak concentration in the surgical site, combined with a low serum level of the drug, is protective against the selection of resistant bacteria; in fact, prolonged high serum concentrations promote the so-called adaptive resistance to gentamicin.
20
Chemical structure of gentamicin.
Pharmacokinetics of GICS
Surgical implants impregnated with gentamicin started to be used in the 1970s, primarily in orthopedic surgery, aiming to treat or prevent prosthetic infections. The first devices had the disadvantage that they were not made of reabsorbable materials; hence, they had to be surgically removed once the infection had been treated. 22
As a consequence, biodegradable polymers such as polylactic acid, polyglycolic-polylactic acid, poly(ortho esters), and polyhydroxybutyrate-co-hydroxyvalerate were developed to carry antibiotic drugs to the surgical site.23,24
Finally, since the 1980s, collagen implants began to be used in several surgical specialties for local antibiotic delivery, mainly due to collagen biocompatibility and pharmacokinetic versatility.23,24
Regarding pharmacokinetics, collagen is a unique polymer because it has a complex, well-known three-dimensional structure with different hierarchical levels: primary, secondary, tertiary, and quaternary. 25 The physiochemical characteristics of the final polymer can be modified by intervening on the molecular structure (eg, intra- and intermolecular cross-links) as well as linking collagen with other polymers to obtain different drug-releasing temporal curves. Hence, when collagen is used as a carrier for a drug, any structural modification can lead to different pharmacokinetic profiles.8,26,27
Collagen biocompatibility and absorbability represent essential characteristics with respect to infection prevention or treatment, because they allow to avoid a further surgical procedure (which could be as well complicated by infection) to remove the drug-carrying device.
Gentamicin-impregnated collagen sponges (GICSs) can be inserted in three different regions during sternal closure, depending on the desired primary site of action:
behind the posterior surface of the sternum, between the bone and the sternal wires; between sternal halves; and on the anterior surface of the sternum, under the muscular fascia.
Every different position of the GICS corresponds to a slightly different spatial distribution of gentamicin, according to the closest sternal region.28,29 For instance, when a GICS was placed posteriorly to the sternum, its effect was more evident in preventing DSWI rather than SSWI. 30
One or two GICSs per patient, corresponding to 130 and 260 mg of gentamicin, respectively, were used in most of the reviewed studies, with various combinations of the above-mentioned positions. There is some evidence that collagen sponges should not be soaked in saline solution prior to use.31,32 Bennett-Guerrero et al conducted a multicenter randomized double-blind trial comparing high-risk cardiac surgical patients receiving a GICS with patients receiving a standard sternal closure. The authors found no advantages for the study group over the control group regarding the incidence of SWI up to 90 days after surgery. The GICS were soaked in saline as per the study protocol, and the authors have been criticized due to this maneuver. 31 Gentamicin is a highly water-soluble molecule, and in vitro studies have showed that exposing a GICS to saline causes the loss of 6.7%, 40.5%, and 100% of the gentamicin after 2 seconds, 1 minute, and 6 hours, respectively. 32 Manufacturers recommend not to soak the GICS prior to use.
GICS use in High-risk Cardiac Surgery Patients
Comparison of various studies that have investigated GICS use in high-risk cardiac surgery patients.
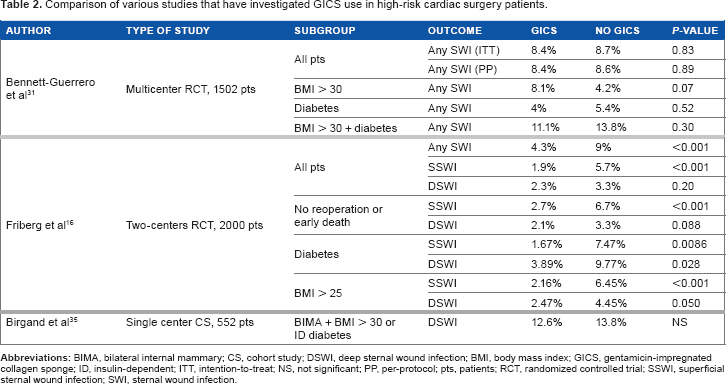
Different results were reported by a previously published randomized controlled trial, 16 where the impact of obesity was specifically subanalyzed. With a cutoff of BMI > 25 kg/m2 (1299 patients), the authors reported a significantly reduced incidence of SSWIs (2.16% vs 6.45%, P < 0.001) and DSWIs (2.47% vs 4.45%, P = 0.05) in the GICS group. The analysis of the whole population confirmed these results only for SSWIs, whereas there were no differences in terms of DSWIs (P = 0.2); these outcomes can be interpreted as a stronger effect of GICS in preventing DSWI in the obese group of patients.
Another subgroup at high risk of SWI includes patients who undergo BIMA harvesting during coronary artery bypass grafting (CABG), as this technique can impair sternal vascularization. 34 A single-center study, published in 2012 by Birgand et al (Table 2), compared the incidence of DSWI requiring surgery in high-risk patients defined as BIMA harvesting plus overweight (BMI > 30 kg/m2) and/or insulin-dependent diabetes. 35 The authors did not find any difference regarding the incidence of DSWI between patients receiving a GICS and those who did not receive it (12.6% vs 13.8%, respectively); interestingly, in that series, the probability of DSWI caused by a gentamicin-resistant bacterium was higher in the GICS group (21/27, 77.8%) compared with the other patients (23/56, 41.1%; P < 0.01). Again, as in the above-mentioned study, GICS pre-soaking in saline solution represented a weakness.
Once we consider the patients who undergo an early reoperation for bleeding (or other reasons) in the immediate postoperative course, the risk of a SWI is increased. In their prospective randomized trial, Friberg et al 16 investigated the beneficial effect of GICS in 2000 patients undergoing cardiac surgery (Table 2); their results showed a reduced incidence of SWI at two months in the treatment group (4.3% vs 9%, RR 0.47; 95% confidence interval [CI] 0.33–0.68, P < 0.001). This result appears to be even more important if we consider that the treatment group had a higher number of early reoperations for bleeding (4% vs 2.3%, P = 0.03), thus suggesting that the use of a GICS is effective in reducing SWI even in the presence of early resternotomy. The authors repeated their analysis, excluding the patients reoperated for bleeding (or other reasons) and those who died within two months; in this subgroup, there was still a significantly lower incidence of SSWIs (2.5% vs 6.7%, P = 0.001) and DSWIs (2.1 vs 3.3%, P = 0.088) in the GICS group.
In 2012, Creanor et al published a meta-analysis including randomized controlled trials, which had previously investigated the use of GICS in cardiac surgery. 36 One of the subanalyses of this study was conducted considering high-risk patients; a statistically significant difference between treatment and control group was found with regard to DSWIs (odds ratio [OR] 0.62, 95% CI 0.39–0.98), while no difference was found with regard to any SWI (OR 0.60, 95% CI 0.24–1.52). 36
Score to calculate DSWI predicted risk.
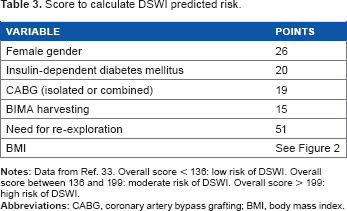
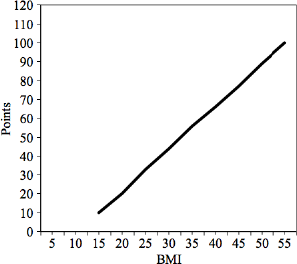
Baseline score points according to BMI (Data from Ref. 33).
Conclusion
GICSs represent a promising option to prevent the occurrence of SWIs after heart surgery. Their main advantage is related to a high local concentration of gentamicin to the surgical site, combined with low serum levels of the drug, thus avoiding systemic side effects.
Most of the current knowledge on their use in cardiac surgery derives from underpowered studies, with different techniques of application. Hence, the real clinical beneficial effects in high-risk patients undergoing cardiac surgery have not been completely established, although there seems to be a tendency toward a reduced incidence of SWIs with their use. This is particularly evident when the device is not soaked in saline solution, as the results appear to be negatively affected by this maneuver.
Currently, there are no guidelines on the use of GICS in cardiac surgery; the scoring system, proposed by Benedetto and Raja, 33 seems to be the most reliable tool presently available for the indication of their use in high-risk patients.
However, further prospective randomized controlled trials, particularly in high-risk patients, are needed to better clarify the impact of GICS in preventing SWIs.
Author Contributions
Conceived the concepts: FR and VDB. Wrote the first draft of the manuscript: FR, VDB, and CZ. Contributed to the writing of the manuscript: PC, GG, and RM. Agreed with manuscript results and conclusions: FR, CZ, GG, RM, PC, and VDB. Jointly developed the structure and arguments for the paper: FR, CZ, GG, RM, PC, and VDB. Made critical revisions and approved the final version: FR, CZ, GG, RM, PC, and VDB. All the authors reviewed and approved the final manuscript.