
Abstract
Mucoepidermoid carcinoma is the most common malignant tumor of salivary glands. However, it is a rare entity in larynx. Laryngeal cases are frequently misdiagnosed with other malignancies and they are under-reported. So, recognizing the clinical and histological features of this tumor is essential. Laryngeal mucoepidermoid carcinoma can arise in supraglottis, glottis and subglottis. Generally, it presents as a submucosal mass; therefore, progressive symptoms without any identifiable lesion in laryngoscopy must be well considered. The prognosis is somehow dependent on the histological features. In high-grade tumors, recurrence is more common and radical surgery with radiotherapy is recommended. In this paper, we provide a thorough literature review on mucoepidermoid carcinoma in the larynx. The most important distinguishing features of mucoepidermoid carcinoma and its two major differential diagnoses (squamous cell carcinoma and adenosquamous carcinoma) are clearly stated and pitfalls in true diagnosis of this tumor are discussed.
Introduction
Mucoepidermoid carcinoma (MEC) is the most common malignant tumor of salivary glands and comprises approximately 5% of all salivary gland tumors. Laryngeal cases comprise one third of malignant laryngeal salivary-type tumors. 1 However, it is a rare entity in the larynx and is frequently misdiagnosed as other laryngeal tumors. Therefore, recognizing its clinical and histological features and distinguishing it from other common laryngeal malignancies are essential.
Methodology
We performed a thorough review of literature on mucoepidermoid carcinoma in larynx. The main concepts in the literature and reported cases are summarized. In addition, the most distinctive histological and clinical features of mucoepidermoid carcinoma are clearly stated in Tables 1 and 2, respectively. For comparison, histological and clinical features of two major differential diagnoses, squamous cell carcinoma (SCC) and adenosquamous carcinoma (ASC), are also presented. Pitfalls in true diagnosis of this tumor are also discussed.
Distinguishing histological features of MEC and its two main differential diagnoses.

Except in high grade tumors.
Clinical features of MEC, SCC and ASC in the larynx.

0%-43%, high-grades; 62%-92%, intermediate-grades; 92%-100%, low-grade.
Clinical Features
Laryngeal mucoepidermoid carcinoma develops from the reserve cells in excretory ducts of submucosal glands 2 or from squamous cells in the surface epithelium. 2 This tumor was first described by Arcidiacono and Loineo in 1963, as a rare entity. 3 The majority of laryngeal cases occur in supraglottis (61%), but they have also been described in glottis (26%) and subglottis (13%) as well as in hypopharynx (Fig. 1). This tendency differs from squamous cell carcinoma of larynx, which most frequently affects the glottis.4,5 Ho et al argued that this tendency is due to the abundance of laryngeal glands, histologically identical to the minor salivary glands, in the submucosal region of larynx. Mucoepidermoid carcinoma of larynx originates from the intercalated cells which are one part of these glands; therefore mucoepidermoid carcinoma is likely to develop at supraglottis where the laryngeal glands are most frequently distributed.6,7

Anatomical distribution of mucoepidermoid carcinoma in the larynx.
The infrequency of reports on laryngeal mucoepidermoid carcinoma could be attributable to difficult recognition of this tumor type when it occurs outside the salivary glands. In addition to the possibility of sampling errors, interpretative errors of tumor specimens have been reported. 8
Laryngeal MECs occur in people of all ages (peak incidence in the 6th decade) and rare cases have been reported in children and adolescents.9,10 This tumor has a definite male predominance and has a wide spectrum of clinical behavior from locally invasive to highly malignant.11,12 Nearly half of the cases develop cervical lymph node involvement;10,13,14 and the lungs are the most frequent site for distant metastasis. 12 An extremely rare case of metastatic laryngeal mucoepidermoid carcinoma in the temporal bone has also been reported. 15
Histopathology
Microscopically, these tumors, similar to mucoepidermoid carcinomas in other sites, are composed of varying proportions of mucous, epidermoid, and intermediate-type cells. 16 Thay are classified as low, intermediate, and high grade (Figs. 2–4). In general, low-grade tumors are predominantly cystic with few mitotic figures and no cellular anaplasia. Intermediategrade tumors are usually more solid and have cellular anaplasia; high-grade tumors typically have solid growth, anaplasia, and a high mitotic rate. 17
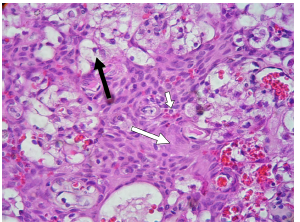
Low-grade mucoepidermoid carcinoma with cystic spaces and mucous tumor cells. Short and long white arrows indicate intermediate and epidermoid cells, respectively. Black arrow shows mucus cells.
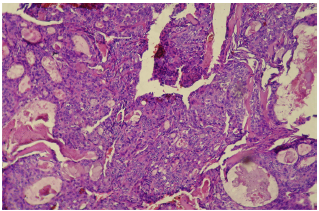
Intermediate-grade mucoepidermoid carcinoma with few mucus cells and prominent population of intermediate and epidermoid cells.

High-grade mucoepidermoid carcinoma with poorly differentiated, irregular nests of tumor cells and very focal mucinous differentiation.
Diagnosis
There are pitfalls not only in early detection but also in true histopathologic diagnosis of these lesions. Tumors often spread submucosally with an intact surface. As a result, primary lesions are not detected by laryngoscopy and most patients are diagnosed in the advanced stages. Therefore, progressive hoarseness and dyspnea, which indicate glottic involvement, as well as stridor and airway obstruction, which imply subglottic lesions, should be taken into consideration. 18 When a laryngeal tumor is detected, its true histological diagnosis is essential. SCC and MEC have similar histopathologic features and presence of intermediate and mucus cells are the only key for differentiation. 19 Since they have different prognosis and treatment modalities, this differentiation is important. Low-grade MECs have better prognosis in adults than SCCs 20 whereas high-grade tumors are associated with a lower survival rate, even lower than the survival rates of SCC. 19 Moreover, many early SCCs of larynx are best treated by irradiation whereas MECs are successfully treated by surgical excision. 21 Despite of all these differences, these tumors are vastly misdiagnosed with each other histologically. 19 Some cases have been reported in the literature that were initially diagnosed as SCC but the presence of glandular structures in metastatic lymph nodes and positive mucicarmine stain changed the final diagnosis to MEC. For that reason, some authors recommend to apply mucicarmine stain to all mistakable cases except for obvious squamous cell carcinomas arising from the surface mucosa. 22 As well, some recent studies have focused on distinctive immunohistochemical expression of MUC-type mucin family in salivary gland tumors and head and neck SCCs. 23 Distinguishing high-grade MEC and SCC by different expressions of Cytokeratins (CKs), especially CK14, has also been suggested. 24
On the other hand, presentation of tumor in metastatic lymph nodes could be helpful in establishing a true diagnosis in high grade tumors. Therefore, careful exploration of metastatic lymph nodes for cystic features and mucus cells in any laryngeal tumor with diagnosis of SCC is recommended.
Distinguishing ASC from MEC is more difficult. A significant number of tumors originally diagnosed as high-grade MEC are ASC, which has more aggressive behavior and shorter overall survival. 25 Chenevert et al stated that 22 of 100 alleged MECs in their research study were ASC. 26 Both neoplasms could be of ductal or surface mucosa origin and share some similar cell types. Mucoepidermoid carcinoma does not usually exhibit anaplastic nuclear features and is not associated with carcinoma in situ of the overlying mucosa. ASC, in contrast to mucoepidermoid carcinoma has tendency to demonstrate intercellular bridges, keratin pearl formation and distinct areas of adenocarcinoma. 27 The main histological and clinical features of MEC, ASC and SCC are presented in Tables 1 and 2.
Prognosis
The prognosis is somehow dependent on the histological features; high-grade tumors have a higher risk of death than low-grade tumors. 28 Pires et al reviewed the literature and reported that overall 5-year survival rates ranged from 0% to 43% for patients with high-grade mucoepidermoid carcinomas, 62% to 92% for patients with interme-diate-grade tumors, and 92% to 100% for patients with low-grade tumors. 29 It has been stated that in patients with tracheobronchial MEC, the proportion of squamoid cells in tumor histology may be an indicator of tumor malignancy and lymph node metastases. 30 The prognosis is not, however, fully dependent on the pathological features. Low to intermediate grade tumors may behave poorly 31 ; even, patients with low-grade MECs have occasionally developed distant metastases at early stages.2,32 The ability to achieve complete surgical resection is one of important prognostic factors and patients who do not achieve complete surgical resection will have a poor prognosis. 12 Clinical studies of patients with head and neck mucoepidermoid carcinomas have also revealed that patients over 56 years of age are significantly associated with decreased survival rate. 2 As a result, considerable note must be taken of the clinical course and both histological classification and clinical behavior, are essential elements to make appropriate therapeutic decisions.2,14
Management
As the main method for therapy, most agree on wide excision; however, radiotherapy or conservative surgery has been used for low grade tumors. 33 The extent of excision is comparable to that of squamous cell carcinoma and extensive tumors require total laryngectomy. 19 The necessity of radical neck dissection is controversial and is usually performed when lymphadenopathy is present; 34 however, it is highly recommended to do elective dissection for all high-grade tumors.
Radical surgery followed by radiotherapy has improved local control in salivary gland malignancies. 35 In addition, postoperative irradiation for MEC patients with positive surgical margin has been reported to be effective. 36 Since high grade MECs have a high incidence of local recurrence (up to 50 percent), postoperative radiotherapy is recommended in these cases.
Nevertheless, recent studies support the elective neck dissection and postoperative radiotherapy not only for high-grade tumors but also for low-grade histologies with positive margins or extracapsular spread. 37
Conclusion
Mucoepidermoid carcinoma is a rare entity in the larynx and is frequently misdiagnosed with other laryngeal malignancies especially squamous cell carcinoma and adenosquamous carcinoma. Therefore, recognizing the distinct clinical and histological features of this tumor is essential. Progressive hoarseness and dyspnea without any identifiable lesion in laryngoscopy may implicate a submucosal mass like mucoepidermoid carcinoma. Histological classification and clinical behavior, are both essential elements to make appropriate therapeutic decisions in these tumors. In the case of high-grade histologies, recurrence must be considered and combination of radical surgery, radical neck dissection and postoperative radiotherapy is recommended.
Disclosures
Author(s) have provided signed confirmations to the publisher of their compliance with all applicable legal and ethical obligations in respect to declaration of conflicts of interest, funding, authorship and contributorship, and compliance with ethical requirements in respect to treatment of human and animal test subjects. If this article contains identifiable human subject(s) author(s) were required to supply signed patient consent prior to publication. Author(s) have confirmed that the published article is unique and not under consideration nor published by any other publication and that they have consent to reproduce any copyrighted material. The peer reviewers declared no conflicts of interest.