
Abstract
Background
Pleomorphic adenoma (PA) is the most common tumor of the salivary gland, while basal cell adenoma (BCA) is an uncommon neoplasm. Blood and lymphatic vessels are crucial for tumor metabolism. The aim of this study was to compare the blood and lymphatic vascular density and vascular and endothelial growth factor (VEGF) expression in PA and BCA tumors. In addition, cell proliferation was evaluated in these tumors.
Methods
Blood and lymphatic vessel content, VEGF expression, and cell proliferation were analyzed in 30 cases of PA and 13 cases of BCA by immu-nohistochemistry using antibodies for CD34, CD105, D2-40, VEGF, and Mcm -2.
Results
Regarding CD34 and CD105 expression, PA demonstrated a high vascularity and a low number of positive vessels, respectively. D2-40-positive lymphatic vessels were mainly located in the tumor capsules, with small intratumoral lymphatic vessels observed occasionally. VEGF expression revealed a remarkably heterogeneous immunoreactivity, alternating from weak or negative to positive or intense. BCA presented significantly higher CD34, CD34, CD105, D2-40, and VEGF expression compared to PA. No significant difference was found in cell proliferation between the tumors.
Conclusion
Although PA and BCA are considered part of the same spectrum of differentiation, this study showed that the blood and lymphatic vascularization of these tumors is different.
Introduction
Salivary gland tumors are rare, accounting for between 2.0% and 5.6% of all neoplasms of the head and the neck. 1 Among them, pleomorphic adenoma (PA) is the most common tumor, accounting for 60%-70% of all neoplasms.1,2 In contrast, basal cell adenoma (BCA) is a rare, benign epithelial neoplasm that comprises 1% −3% of the epithelial salivary gland tumors.1,3 PA and BCA have numerous similarities. They are composed of luminal and abluminal cells, and both have a good prognosis.1–3
In tumor biology, the blood and lymphatic vessels are important components of the tumor microenvironment. The blood and lymphatic vessels of tumors are newly formed from the preexisting host vessels in response to stimulation by pro-angiogenic and pro-lymphangiogenic factors expressed by tumor cells, such as the vascular endothelial growth factor (VEGF). Tumor cells establish a specific stromal microenvironment that fosters tumor growth, which involves blood/lymph angiogenesis. 4 Studies have shown that triggering angiogenesis and lymph angiogenesis are crucial events in tumor growth.5,6
Studies indicate that the processes of proliferation and angiogenesis delineate the biology of individual tumors. 7 Many cell cycle proteins have been employed as cell proliferation biomarkers, of which Ki-67 and Mcm-2 are the most widely used.8,9 Mcm-2 is present in the early G1 phase of the cell cycle.8,10 For this reason, research currently suggests that Mcm-2 is a more specific and sensitive cell proliferation marker than Ki-67.8,9,11
The blood and lymphatic vascularization of malignant tumors has been widely investigated, mostly concerning angiogenesis and antiangiogenic therapy. However, these studies have focused on the malignant processes, whereas few studies have been devoted to benign tumors. There are a few studies concerning blood and lymphatic vascularization in PA,12,13 while there has been no such investigation for BCA. Therefore, the purpose of this study was to compare the vascular/lymphatic microenviroment in PA and BCA. Using immunochemistry, a comparison was made by measuring the microvessel density (MVD) using antibodies for CD34 and CD105, lymphatic vascular density (LVD) using the D2-40 antibody, and growth factor using the VEGF antibody. In addition, immunohistochemical staining for the Mcm-2 antigen was conducted to evaluate cell proliferation in PA and BCA tumors.
Materials and Methods
The present study involved 30 cases of PA and 13 cases of BCA. Two pathologists reviewed all diagnoses using 5-μm sections obtained from formalin-fixed, paraffin-embedded samples and stained with hematoxylin and eosin. Demographic and clinical information were obtained from the patients' medical records. The study protocol was approved by the Committee of Ethics in Research of the Faculty of Dentistry at the São Leopoldo Mandic Institute and Research Center.
Immunohistochemistry
One paraffin block from each case was chosen for immunohistochemical staining with the following antibodies (Table 1): anti-CD34 and anti-CD105 to detect blood vessels; anti-D2-40 to detect lymphatic vessels; anti VEGF to detect vascular growth factors; and anti-Mcm-2 to detect cell proliferation.
Details of the antibodies used for immunohistochemistry.
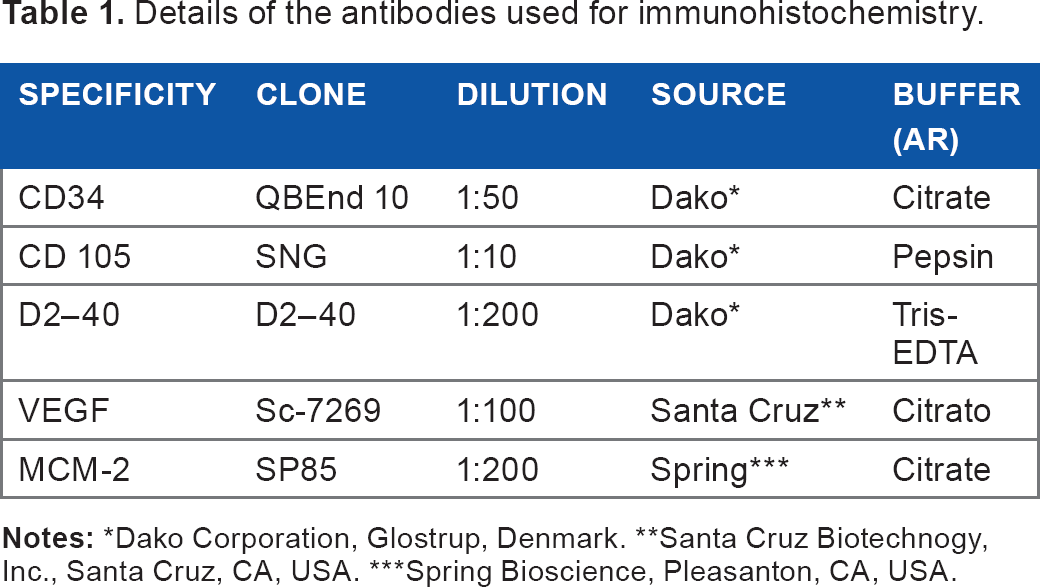
Dako Corporation, Glostrup, Denmark.
Santa Cruz Biotechnogy, Inc., Santa Cruz, CA, USA.
Spring Bioscience, Pleasanton, CA, USA.
The 5-μm sections were deparaffinized and hydrated, and endogenous peroxidase activity was quenched by immersing the slides in 3% hydrogen peroxide. Antigen retrieval (AR) was achieved by immersing the slides in boiling citrate buffer (pH 6.0) for all antibodies except for anti-CD105, which was performed using 0.4% pepsin for 30 minutes (Table 1). Only the anti-CD105 sections were incubated at 37 °C with a serum-free protein blocking solution (code x0909, Dako, SA) for 30 minutes. Subsequently, the sections were incubated with the primary antibody overnight at 4 °C, followed by EnVision polymer HRP and Envision+ (code K1491, DAKO) for one hour at 37 °C. The sections were stained for five minutes at 37 °C with 3,3′-diaminobenzidine tetrahydrochloride (DAB) and counter-stained with hematoxylin. A negative control was obtained by omitting the primary antibody. No staining was observed in this section.
Density of blood and lymphatic microvessels
Immuno-histochemical staining for CD34, CD105, and D2-40 was interpreted by two pathologists using a double-headed microscope. Observation of vascularization was performed throughout the whole specimen, but the most cellular areas were chosen for counting of the vasculature. To assess the number of vessels, images were obtained from five fields (hotspots) per case (40 X objective, 0.44 mm field diameter) using a camera attached to an Olympus CX30 microscope. The images were analyzed with Imagelab analysis software (version 2.4), which allowed manual segmentation of the target vessels. The blood and lymphatic microvascular densities obtained from CD34, CD105, and D2-40 immunostaining were expressed as the mean number of intratumoral microvessels counted. There was no restriction regarding the size of a countable microvessel; however, vessels with muscular walls and areas observed to be necrotic were excluded.
Growth factor
Growth factor immunohistochemical reactions to VEGF were used in the initial evaluation to verify the expression pattern of the sections stained with the antibody. The labeled sections were evaluated qualitatively and semiquantitatively. The qualitative analysis was performed via the evaluation of the positive cells from different areas in all cases. The relative number of neoplastic cells was considered in relation to all neoplastic cells observed for each stained section. When the number of positive cells was more than 10%, the case was considered positive. A grading system based on reactivity percentage was assigned on a scale from 0 to 3. Less than 10% cell reactivity was assigned 0; 10%–25% cell reactivity was assigned 1; 25%-50% cell reactivity was assigned 2; and reactivity greater than 50% was assigned 3.
Cell proliferation
The proliferative indexes of Mcm-2 were obtained by calculating the percentage of cells with positive nuclear staining in a total of 500 tumor cells examined by microscopy at 40x magnification.
Statistical analysis
Statistical analysis of the data was performed using GraphPad Prism 4® statistical software; the Kolmogorov-Smirnov test was used for evaluation of normality. Comparison between two groups of variables with nonnormal distribution was performed using the Mann-Whitney test. VEGF staining was evaluated using a score, with the statistical test employed being the Wilcoxon. The level of significance in both tests was set at 5%.
Results
The PA group included 20 women and 10 men. Nineteen of the tumors were located in the palate, eight in the parotid, and three in the submandibular glands. The average age of the patients was 38 years. The BCA group included seven women and five men, as well as one person whose gender was not listed. The average age was 62 years, with 12 tumors being located in the parotid and 1 tumor in the glands of the upper lip. Data were not available for one BCA and one PA case.
Microvascular density assessed using anti-CD34 and anti-CD105
CD34-positive staining revealed high vascularity in both tumor types. In PA, the vessels were detected mostly in cellular-rich areas (mean = 6.33, SD = 4.02), whereas in BCA the vessels were dispersed throughout the tumors (mean = 12.23, SD = 3.28). There was a significant difference between PA and BCA in terms of the MVD for CD34 (P = 0.001) (Figs. 1A, 1B, and 2).

Immunostaining of blood and lymphatic vessels in pleomorphic adenoma (PA) and basal cell adenoma (BCA). Many CD34-positive blood vessels are seen in PA and BCA

Box and whisker plots of lymphatic vessel density (LVD) and microvessel density (MVD) in pleomorphic adenoma (PA) and in basal cell adenoma (BCA) (n = 30 and 13, respectively) determined using CD34, CD105, and D2-40 antibodies.
When assessing MVD using anti-CD105 staining, a few small, positively stained vessels were detected in the cellular-rich areas of PA (mean = 0.47, SD = 1.17), while in BCA the number of positive vessels was slightly higher, with them being widely spread throughout the entire tumor (mean = 4.69, SD = 3.22). A significant difference was also observed between the two groups of tumors (P = 0.0001) (Figs. 1C, 1D, and 2).
Lymphatic vessel density
In PA, D2-40-positive lymphatic vessels were mostly concentrated in the tumor capsules, with small intratumoral lymphatic vessels being infrequently observed (mean = 0.34, SD = 0.44) (Figs. 1E, 1F, and 2). The lymphatic vessels in BCA were also identified at the tumor margin, with a small increase observed in the number of intratumoral vessels compared to that of PA (mean = 1.83, SD = 1.53). Comparison of the two groups showed that the difference in LVD was significant (P = 0.0004).
Growth factor
VEGF positivity was observed in both the nuclei and cytoplasm. In PA, a remarkably heterogeneous VEGF immunoreactivity was observed, alternating from weak or negative to positive or intense. Immunoreactivity was most marked in the epithelial cells and rarely seen in mioepithelial cells. In 13 cases (43%), the cells were negative or showed less than 10% reactivity (score 0); 9 cases (30%) had a score of 1; 5 cases (17%) showed 25%-50% reactivity (score 2); and 3 cases (10%) scored 3 (Figs. 3C and 4).

Histopathology of PA

Box and whisker plots of VEGF and Mcm-2 expression in pleomorphic adenoma (PA) and basal cell adenoma (BCA) (n = 30 and 13, respectively).
All BCA tumors revealed a strong positivity to VEGF, with an immunoreaction of more than 50% (score 3) (Figs. 3D and 4). Immunoreactivity was observed in epithelial cells, mostly in the basal layer. A significant difference was observed in VEGF positivity between PA and BCA (P = 0.0001).
Proliferative index
No or a small number of Mcm-2-positive cells were detected in both PA (mean = 13.23, SD = 11.63) and BCA (mean = 12.85, SD = 10.35). No significant difference was found between the Mcm-2 proliferative indexes of the tumors (P = 0.9948) (Fig. 2).
Discussion
The stromal microenvironment plays a critical role in tumor biology, with the blood and lymphatic vessels found within the tumor tissues being key components of the tumor microenvironment. Tumor-associated angiogenesis is an essential pathophysiological phenomenon for sustaining the viability of tumor cells during tumor progression.4,14,15 However, information is lacking on the role of angiogenesis and lymphatic distribution in benign tumors.
The role of angiogenesis in the onset and progression of salivary gland malignancies is well recognized, 14 with an angiogenic switch having been reported during the malignant transformation of pleomorphic adenoma to carcinoma ex-pleomorphic adenoma. 14 Previous studies from our group have shown that vascularization in PA is composed mainly of preexisting vessels in a positive correlation to the cellular density of the tumor, where the most cellular-rich areas have the highest vascular density. 12
The present study detected a small increase in vascularization from preexisting vessels, with a greater increase in newly formed vessels in BCA compared to PA, which was observed in the comparison of the MVD obtained using CD34 and CD105. This difference could be attributed to the diversity of the stroma observed in PA tumor, in which high vascularization is not required in myxoid and condroid areas. In contrast, BCA is a cellular-rich tumor containing minimal stroma -and hence the need for increased vascularity - and indicating that the preexisting vessels were insufficient for maintaining the tumor cells, thus requiring the formation of new vessels. These results confirm our previous studies, in which it was suggested that the degree of vascularization in benign salivary tumors depends on cell density, most likely due to cellular-rich tumors requiring more oxygen in order to support metabolic demands.
The ability of tumor cells to induce angiogenesis varies greatly depending on the type of neoplastic cell.16,17 The angiogenic switch has been reported to be induced primarily by malignant cells14,16,18; however the role of this switch is not well understood in benign tumors. The angiogenic switch can be analyzed by immunohistochemistry for CD105, which is expressed by proliferating endothelial cells, making CD105 a good marker for newly formed vessels. 19 The current study detected few CD105-positive vessels in PA, indicating the absence of an angiogenic switch in this type of tumor. In contrast, CD105-positive vessels were detected more frequently in BCA, suggesting that an angiogenic switch was occurring in this benign tumor.
Some growth factors play a crucial role in the regulation of blood vessel formation, with VEGF-A (commonly named VEGF) being among these.20,21 In the present study, VEGF positivity confirms the presence of an increased vascularization in BCA when compared to PA.
Lymphatic vessels play an important role in maintaining fluid balance and tissue homeostasis, as well as being a noteworthy component of the immune system. 22 Tumor research has focused on lymphatic vessels, as they represent the main route for metastases to the lymph nodes. However, the consequence of tumor-associated lymphangiogenesis in the viability of tumor cells is unclear. 23 A high lymphatic vessel density seems to be an indicator of the risk of lymph node metastasis in cutaneous melanoma, head and neck squamous cell carcinoma, and squamous cell carcinoma of the cervix.24,25 In contrast, no intratumoral lymphatic networks have been reported for other carcinomas, such as those of breast, ovarian, endometrial, and lung.26,27 No significant difference in lymphatic vessel density of high-risk salivary gland tumors and low/ moderate-risk salivary gland carcinomas has been observed with regard to nodal metastasis. 28
The benign salivary gland tumors PA and recurrent pleomorphic adenoma have been reported to have very few, if any, intratumoral lymphatic vessels, 12 with the present study finding similar results. However, this study did detect a small number of lymphatic vessels in BCA. The function of the lymphatic vessels is critically dependent upon the composition, geometry, and integrity of the extracellular matrix. 29 Therefore, in a previous study performed by our group, the stroma was suggested as a possible explanation for the absence of intratumoral lymphatic vessels in PA, in terms of it possibly collapsing the lymphatic vessels and/or pushing the preexisting vessels outside the tumor.2,12 Moreover, a possible explanation for the presence of more lymphatic vessels in BCA than PA found in the present study could be that BCA has a scarce stroma, in which these vessels are presented.
Although a difference in vascularization between PA and BCA was observed in the current study, the cell proliferation indices obtained using Mcm-2 staining were similar, indicating that both tumors have the same cell proliferation features. Indeed, PA and BCA have the same biological behavior in terms of slow growth and a low risk of recurrence or malignant transformation.1,3
In conclusion, despite the fact that PA and BCA are considered part of the same spectrum of differentiation, these tumors are different with regard to vascularization, as demonstrated by immunohistochemistry for CD34, CD105, D2-40, and VEGF.
Footnotes
Author contributions
Conceived and designed the experiments: ABS, AA, FPS, VCA. Analyzed the data: TRO, FOFR, ARS, DFS, STB, MHN, ABS. Wrote the first draft of the manuscript: ABS, VCA. Contributed to the writing of the manuscript: ABS, FPS, MHN, VCA. Agree with manuscript results and conclusions: All authors. Jointly developed the structure and arguments for the paper: ABS, AA, VCA. Made critical revisions and approved final version: ABS, AA, VCA. All authors reviewed and approved of the final manuscript.