
Abstract
Background
Chronic lymphocytic leukemia (CLL) is the most common leukemia in adults. The chromosomal abnormality t(14;18)(q32;q21) is most commonly associated with neoplasms of a follicular center cell origin. However, t(14;18) has also been reported in rare cases of CLL.
Objective
We describe the clinicopathologic, immunophenotypic, conventional, and molecular cytogenetic features of two rare cases proven to be CLL morphologically and immunologically in which t(14;18) was found as the sole cytogenetic abnormality.
Methods
Morphologic, flow cytometric analysis and molecular cytogenetic of peripheral blood and/or bone marrow samples were analyzed.
Results
Cytomorphologically, the cells were small mature lymphocytes without any findings that had characteristics of follicular lymphoma (FL) such as indented or clefted nuclei. Immunologic findings were characteristic of typical CLL without expression of CD10. A cytogenetic study revealed the two cases of CLL carrying t(14;18)(q32;q21).
Conclusion
We concluded that CLL with t(14;18) is rare and should be differentiated from FL as the therapy is highly diverse between both diseases. Using immunoglobulin heavy chain gene (IGH) probes are important in the workup of patients with suspected CLL and suggest that the IGH probe should be used routinely in all CLL fluorescence in situ hybridization (FISH) panels.
Introduction
B-cell chronic lymphocytic leukemia (CLL) is an indolent mature B-cell neoplasm that is diagnosed based on the demonstration of an abnormal population of B lymphocytes in the blood greater than 5.0 × 10 9 /L, which display an unusual but characteristic pattern of immunophenotypic features.
The typical immunological profile of classic B-cell CLL is characteristically strongly coexpressing CD5, CD19, CD23, C43, and CD79a. Weak to moderate expressions of CDllc and CD20 are also found. CD10 is negative, while FMC7 and CD79b may be weakly positive. 1 However, some cases have atypical immunophenotype and overlap with the other B-cell lymphoma.2,3
In 60-80% of CLL patients, cytogenetic abnormalities can be identified, such as deletions in chromosomes 6q21, llq22, 13ql4, and 17pl3, and trisomy 12(+12).4,5 Based on these cytogenetic abnormalities, the patient's prognosis can be estimated.
The t(14;18) translocation involving IGH and BCL2 genes has been identified in up to 90% of follicular lymphomas (FLs) 6 and 20-30% of diffuse large B-cell lymphomas (DLBCL). In lymphomas of non-follicular origin, t(14;18)(q32;q21) is extremely rare. In FL, breakpoints of t(14;18) occur in the major breakpoint region (mbr) or in the minor cluster region (mcr) at the 3’ end of BCL2, whereas in CLL the breakpoints have been found to be at the 5’ end juxtaposing BCL2 to the immunoglobulin light chains. However, large series showed BCL2 rearrangements to be rare events in CLL. 4
Chromosomal translocations are uncommon in CLL, identified in less than 5% of all cases.7–10 t(14;18) is highly unusual in CLL and is found in 1-2% of cases.11–14
Here we describe two rare cases of CLL carrying t(14;18) (q32;q21). The cells were small mature lymphocytes without any morphologic or immunologic findings that had characteristics of FL, such as cleaved nuclei or CD10 expression.
Materials and Methods
Case selection
We searched the database of the Cytogenetics Laboratory for cases with t(14;18)(q32;q21), other reciprocal chromosomal translocations such as t(14;19)(q32;q13), or variant translocations t(2;19)(p13;q13) and t(19;22)(q13;q11) during the period between January 2010 and June 2014. Out of 96 cases, we identified 2 cases with t(14;18)(q32;q21). Both cases were diagnosed as CLL/small lymphocytic lymphoma (SLL) based on morphologic and immunophenotypic criteria, but no cases with t(14;19)(q32;q13) or the variant trans-locations were identified. We retrieved clinicopathological data, immunophenotype, and cytogenetics from the medical records. This study was approved by the Ethics and Research Committee of the Department.
Morphologic examination
In each case, we reviewed the peripheral blood (PB) smears, bone marrow (BM) aspirate smears, touch imprints, and core biopsy specimens with more attention given to lymphocyte morphology with respect to atypical features, including indented or clefted nuclei, the presence of prolymphocytes, immature-large cells, or plasma-cytoid features.
Immunophenotyping
The PB and/or BM samples were subjected to immunophenotypic studies by a flow cytometry using a CD45/side scatter gating strategy to analyze the lymphocyte population. Immunohistochemical stains were performed using routinely fixed, paraffin-embedded tissue sections of BM biopsy and lymph node.
Cytogenetic analysis
Conventional cytogenetic analysis was performed on metaphase cells prepared from PB and/or BM specimens cultured for 24 and 72 hours without mitogens, using standard techniques. A total of 20 metaphases were analyzed, and the result was reported according to International System for Human Cytogenetic Nomenclature (ISCN) 2009.
Fluorescence in situ hybridization (FISH) analysis for common abnormalities associated with CLL was performed using the following probes panel: TP53/CEP17, D13S319/13q34, IGH/CCND1 (DC, DF), IGH/BCL2 (DC, DF), and CEP12 to detect the common cytogenetic abnormalities according to the manufacturer's instructions (Abbott Molecular, Abbott Park, IL). A total of 200 nuclei were analyzed for every probe test, and the result was reported according to ISCN 2009.
Result
Patients
Table 1 summarizes the laboratory findings and clinical characteristics of the patients at diagnosis.
Laboratory findings and clinical characteristics of the patients at diagnosis.
Case 1
A man in his 70s was known to have hypertensive, ischemic heart disease with a history of recurrent cerebral strokes. In June 2010, he discovered incidentally from the workup of his follow up for previous diseases to have leukocytosis and absolute lymphocytosis. Complete blood count (CBC) at that time showed a hemoglobin (Hb) count of 13.5 g/dL (reference interval, 12.5-18 g/dL), a white blood count of 18.2 × 10 9 /L (reference interval, 4-11 × 10 9 /L), and a platelet count of 188 × 10 9 /L (reference interval, 150-450 × 10 9 /L). Differential count showed 74.2% lymphocytes with the presence of smear cells. The patient was referred to Hematology Clinic because of PB findings that gave initial clinical impression of CLL, which was confirmed by a flow cytometry analysis.
The patient was asymptomatic (no fever, weight loss, or sweating) and clinically stable. Clinical examination was irrelevant. No lymph nodes were palpable and no hepatosplenomegaly was observed. The lactate dehydrogenase (LD) value was within the normal range -215 U/L (reference interval, 135-255 U/L), and the β2-microglobulin level was elevated -3.5 mg/L (reference interval, 1.09-2.53 mg/L).
Until now, no treatment was given. His WBC count remained stable during follow up. The last follow up was at April 2014. The patient remained clinically stable, and his WBC count was 24.2 × 10 9 /L with 78% lymphocytes, Hb count was 14.2 g/dL, and platelet count was 179 × 10 9 /L, with no need for treatment. The patient refused to do BM examination during diagnosis and for follow up.
Case 2
A man in his 50s was known to be hypertensive and diabetic. In January 2011, he presented with 3 months history of mild enlargement of lymph nodes in the neck and submandibular and inguinal areas, but no B-symptoms or other relevant complaints. His CBC at presentation revealed leukocytosis and absolute lymphocytosis, with an Hb count of 10.8 g/dL, a white blood count of 38.4 × 10 9 /L, and a platelet count of 98 × 10 9 /L. Differential count showed that 78% were small, mature-looking lymphocytes with the presence of smear cells. Findings gave clinical suspicion of CLL, which was confirmed by a flow cytometry analysis of PB. The LD value (270 U/L) and also the (β2-microglobulin level (5.2 mg/L) were elevated.
His BM examination also confirms the diagnosis of CLL, and he had disease progression. He was treated by FCR (fludarabine, cyclophosphamide, and rituximab) chemotherapy regimen every 28 days for four cycles. After the treatment, the patient got remission until December 2013 when he presented again with generalized lymphadenopathy mainly cervical and axillary lymph adenopathy and mild leukocytosis. He also had on and off fever with night sweat. At admission, WBC count was 13.8 × 10 9 /L, Hb count was 11.3 g/dL, and platelet count was 81 × 10 9 /L. Differential peripheral blood film showed lymphocytosis (60%). Serum (-2 microglobulin level (10.9 mg/L) and also LD value (277 U/L) were elevated. A computed tomography of the chest, abdomen, and pelvis was done, which showed development of extensive huge mediastinal, axillary, paraaortic, mesenteric, iliac, and inguinal lymphadenopathy with hepatosplenomegaly indicating progression of the disease. BM examination and lymph node biopsy (tru-cut biopsy from the axillary lymph node) were done and reported as relapsed CLL/SLL with no evidence of transformation to high-grade lymphoma. After that, the patient started the same FCR chemotherapy. Currently, the patient is in remission, and his CBC at last follow up at May 2014 revealed an Hb count of 11.6 g/dL, a WBC count of 4.5 × 10 9 /L, and a platelet count of 10 9 × 10 9 /L.
Morphologic findings
Lymphocyte morphologic features were considered typical for CLL in both cases. Lymphocytes were mature, small with round nuclei, clumped chromatin, scant cytoplasm, and regular cellular outline. Rare prolymphocytes and broken cells (smudge or smear cells) were seen (Fig. 1). BM examination (case 2) showed lymphoid cells’ infiltration in a nodular pattern. The infiltrates were composed of predominantly small, mature-looking cells with occasionally admixed larger cells. No proliferation centers were identified in the BM (Fig. 2). Lymph node biopsy at relapse showed diffuse effacement of the architecture with small, round lymphocytes with condensed chromatin and scanty cytoplasm (Fig. 3).
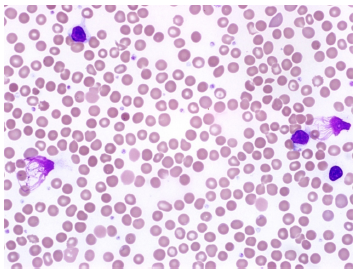
(Case 1) PB smear shows the lymphocytes are mature, small with round nuclei, clumped chromatin, scant cytoplasm and regular cellular outline, broken cells (smudge or smear cells) are seen.
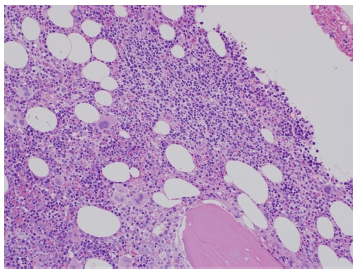
The bone marrow core biopsy section from case 2 illustrates a focal, nonparatrabecular infiltration of small mature lymphocytes.

Low power image (H and E) of tru-cut lymph node biopsy of case 2 showing diffuse effacement of the architecture with small, round lymphocytes with condensed chromatin and scanty cytoplasm.
Immunophenotyping findings
In both cases, FCM analysis showed typical immunophenotyping for CLL and revealed clonal B cells with kappa light chain expression and immunophenotype characteristics of CLL with positivity for CD19, CD20 (weak), CD23, CD22, HLA-DR, and CD5 and negativity for terminal deoxynucleotidyl transferase (TdT), CD10, FMC7, CD38, and myeloid and T-cell markers (Fig. 4).

Flow cytometric analysis of PB sample of case 1 revealed clonal B cells with kappa light chain expression. B cells express CD5, CD19, CD20 (weak) and CD23. FMC-7 and CD10 are negative.
Immunohistochemical stains performed on BM biopsy and lymph node specimens (case 2) showed that the lymphoid cells were positive for BCL2, CD20, and CD5. Staining for Ki-67 revealed a low fraction of proliferating cells (<10%). The neoplastic cells were negative for cyclin D1, CD10, and CD3 (Fig. 5A and B).

The bone marrow core biopsy section from case 2 shows the lymphocytic infiltration is positive for BCL-2 and CD20 respectively.
Cytogenetic findings
In case 1, karyotype analysis detected the presence of the balanced reciprocal translocation t(14;18)(q32;q21), as a sole chromosomal abnormality in 6 among the 20 analyzed cells. FISH confirms the presence of IGH-BCL2 fusion in 65% of analyzed nuclei. The result of cytogenetic investigations is as follows: 46, XY, t(14;18)(q32;q21) [6]/46, XY[14].nuc ish (TP53x2)[200]/(D13S319x2)[200]/(CCND1, IGH) x2[200]/(IGHX3), (BCL2X3)(IGH con BCL2X2)[130/200]/(D12Z3) X2[200] (Fig. 6).
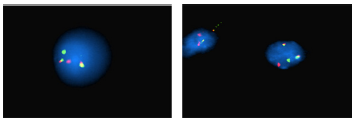
(Case 1) Fluorescence in situ hybridization (FISH) using LSI IGH/BCL2 Dual Color Dual Fusion probe. The nucleus containing the t(14;18) translocation showed the presence of one orange signal indicating the native BCL2 gene, one green signal indicating the native IGH gene and 2 fusion signals indicating the presence of the 2 derivatives chromosomes resulting from the translocation.
Similarly, in case 2, FISH detected the presence of IGH-BCL2 fusion in 70% of analyzed nuclei and reported as follows: nuc ish (TP53x2)[200]/(D13S319x2)[200]/(CCND1, IGH) x2[200]/(IGHx3), (BCL2x3),(IGH con BCL2x2)[140/200]/(D12Z3)X2[200]. Karyotype analysis was not performed due to an insufficient number of metaphases.
Discussion
CLL is the most common leukemia in adults. The morphologic features and immunophenotype of CLL cells are well characterized. 15 Chromosomal translocations are uncommon in CLL.7,10 t(14;18)(q32;q21) is considered highly specific for FL but has been found also in DLBCL.16,17 The presence of t(14;18) is highly unusual in CLL. In the literature, few cases have been reported. Its prevalence is found in 1-2% of cases.7,9,11–14,17
Both patients were men, one in his 70s and one in his 50s at the time of diagnosis. Both patients presented with leukemia, and case 2 also presented with nodal disease at relapse. In our study, although BCL2 gene rearrangement occurs much more frequently in FL, our cases were diagnosed as CLL rather than FL as the lymphocytes had the typical morphologic and immunophenotypic characters of CLL. Lymphocytosis was incidentally discovered without any clinical symptoms in case 1 and with only mild lymphadenopathy without B-symptoms in case 2. Similar to our patients and depending on combination of immunophenotype and morphological studies, few cases of CLL had been reported previously.17,18 Also, in our study t(14;18) was the sole karyotypic abnormality, which is extremely rare and has been reported previously in few cases of CLL.7,10,11,13,14,17,19
In the large study by Sen et al that contained 2215 cases of CLL, only 2 cases were identified carrying t(14;18). But unlike our cases, in both patients, in addition to t(14;18), trisomy 12 (+12) was identified in the same clone. 11
In the most recently published article by Tang et al, who searched for cases of CLL with t(14;18) between 1996 and 2010 and identified 12 cases (less than 1% of all cases) classified as CLL/SLL, only two cases carried t(14;18) as the sole karyotypic abnormality. 20 This finding with other reported studies,7,10,11,13,14,17,19 in addition to the current study, indicates that the overall CLL cases carry t(14;18) (q32;q21) as the sole cytogenetic abnormality is extremely very rare.
In addition to t(14;18), other translocations involving the BCL2 gene have been shown in rare cases of CLL.10,21–23 Dyer et al. 18 estimated the overall incidence for translocations involving the BCL2 gene in CLL as 2.3%, with t(14;18) being the most common.
The prognostic significance of t(14;18) in CLL is still a controversial matter. 17 Some studies have suggested that CLL with molecular and/or cytogenetic evidence of BCL2 translocations does not appear to be associated with poor prognosis or progressive disease.7,8,10,19,24 However, other studies failed to demonstrate a strong association between t(14;18) and an inferior outcome.11,13,14,19 Our patient (case 1) is clinically stable, did not need treatment until now (more than 3.5 years), shows no evidence of progression, and had an indolent course while case 2 showed progressive disease and required chemotherapy. After more than 2 years of remission, relapse occurred and the patient presented with extensive generalized lymphadenopathy but without evidence of transformation to high-grade lymphoma. However, as the number of cases of CLL with t(14;18) in all reported studies is very small, prospective studies will be required to assess the prognostic relevance of t(14;18) in CLL.
Some reported studies suggested that the bcl2 translocations occurring in CLL are different from those that typically occur in FL,4,18,25 and further molecular analysis studies are needed to confirm this finding as this distinction cannot be made by either conventional cytogenetical methods or by our FISH assay for IGH and BCL2.4,17
In both patients, the immunophenotypic analysis showed negativity to CD38 although the clinical course in both patients was different as case 1 was clinically stable whereas case 2 showed disease progression. This observation did not support the findings reported by Damle et al who demonstrated that the CD38 expression level was a significant prognostic marker in CLL. CLL with a higher percentage of CD38+ cells (using the 30% cut-off for CD38 positivity) comprised unmutated CLL cases, whereas CLL with lower percentage contained almost the mutated cases indicating CD38 expression in CLL can serve as a surrogate marker for the immunoglobulin variable heavy-chain (VH) genes mutation status.26–28 Subsequently, CLL can be segregated into two subgroups on the basis of the presence or absence of significant numbers of VH gene mutations.7,8 However, this finding is currently controversial.29–32
The cellular origin of CLL is still in debate. Extensive molecular investigations of the B-cell receptor (BCR) indicate that 60-65% of CLL patients carry mutated immunoglobulin heavy-chain variable genes, while approximately 35% harbor unmutated IgV genes.26,33
The association with IGHV gene mutations suggests that a fraction of cases derived from germinal center (GC)-experienced B-cells, while the remaining cases (unmutated IGHV genes) derived from B-cells that have undergone differentiation in a GC-independent fashion.34–36 Also, transcriptome analyses of CLL revealed that immunoglobulin variable region (IgV) gene unmutated CLL derived from unmutated mature CD5(+) B cells and mutated CLL derived from a distinct CD5(+)CD27(+) post-germinal center B-cell subset.37,38
Our experience in evaluation of CLL cases included a probe to detect BCL2 gene rearrangement, and if positive, we included both t(14;18) and t(11;14) in a FISH panel to exclude a rare type of negative FL (CD10) and mantle cell lymphoma (MCL), respectively, especially with atypical morphology or immunophenotype as in rare cases overlapping and confusion in diagnosis may occur. Correlation of FISH analysis with clinical, immunophenotype, and morphological findings is recommended for all cases of CLL, and also lymph node biopsy should exclude diagnosis of FL in cases of CLL with t(14;18) if associated with lymph-adenopathy, atypical immunophenotype, and/or atypical morphology.
Summary
We concluded that CLL with t(14;18) is rare and should be differentiated from FL if associated with lymphadenopathy, atypical immunophenotype, and/or atypical morphology as the therapy is highly diverse between both diseases. Also, we conclude that using IGH probes is important in the workup of patients with suspected CLL and suggest that the IGH probe should be used routinely in all CLL FISH panels
Author Contributions
Conceived and designed the experiments: GE, AA. Analyzed the data: GE, HE. Wrote the first draft of manuscript: GE. Contributed to the writing of the manuscript results and conclusions: KF, OA, HO, HE. Jointly developed the structure and arguments for the paper: GE, KF, OA, HO, HE. Made critical revisions and approved final version: GE, AA. All authors reviewed and approved the final manuscript.
Footnotes
Acknowledgment
The authors would like to acknowledge Mr. Waleed Al-Bissi from Histopathology Division for assistance in this study. Also, they thank Dr. Inesse Ben-Abdallah Bouhajar for her help in the study and collection of cytogenetic data.