
Abstract

Introduction
Limb salvage in patients who have sustained major extremity vascular trauma during wartime has increased significantly over time: World War II, 50%; Korean War, 87%; and Vietnam, 92%.1–3 This increased salvage rate is attributed to arterial reconstruction. Delay in revascularization continues to hamper limb salvage both in military settings as well as civilian trauma settings. Damage control surgery (DCS) has revolutionized modern trauma care both in the civilian arena and on the battlefield. Temporary intraluminal shunts are shown to provide adequate limb and organ perfusion in the damage control setting in the civilian trauma literature until a severely injured patient is stable enough to undergo a formal vascular repair, and/or major fractures are stabilized and devitalized soft tissue is debrided.4,5 Rural surgeons sometimes deal with a delay in evacuation due to geographic distances between accident site and level one trauma centers as well as weather delays. Such challenges can be found in each region of the country and in current military activities throughout the world. Eger and associates were the first to report the use of temporary shunts in the damage control setting at a fixed tertiary care facility. 6 However, there are few retrospective reports showing their successful use in the far-forward, military field environment7,8 and none showing usefulness in a strategic evacuation. This case report of using a temporary intraluminal shunt represents one extreme aspect of damage control surgery (DCS) as applied to the austere conditions of a far-forward, military special operations environment on the modern battlefield during initial combat operations in Afghanistan.
Case Report
A 20-year-old male presented to the 250th Forward Surgical Team while in support of Operation ENDURING FREEDOM in Kandahar, after sustaining a gunshot wound that traversed both thighs after the accidental discharge of a Kalishnikov assault rifle. The injury occurred approximately 30 minutes prior to his arrival. He was reported to have bled extensively at the scene. On presentation His Glascow Coma Score was 13 and Revised Trauma Score (RTS) was 7.5. He was hypotensive and tachycardic. Pulses were absent in the right lower extremity below the level of injury and only a weak signal was found by Doppler on the left. Secondary survey revealed no other injuries other than a small right lateral thigh entrance wound, a larger, 2–3 cm right medial thigh exit wound and entrance and exit wounds to the left upper thigh with significant soft tissue destruction. The mangled extremity severity score of the right leg was six. Resuscitation was begun with crystalloid and blood. He was quickly taken to the operating table where general endotracheal anesthesia was induced.
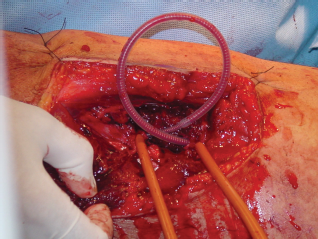
An one-shot intra-operative, bilateral, lower extremity arteriogram was performed to evaluate for possible injury to more proximal vessels and runoff. This showed normal left superficial femoral and profunda femoral arteries (Figs. 1 and 2). Flow in the right superficial femoral artery was shown to taper off with no flow past the mid-thigh. As proximal control of the inflow to the right leg was being obtained at the groin with “pottsed” vessel loops, our unit was overwhelmed with other casualties, most requiring urgent surgical intervention. His base deficit was 6, temperature 94 degrees, and he had received 4 units of packed red blood cells. Due to the barrage of additional operative casualties, this casualty's impending triad of death (hypothermia, acidosis and coagulopathy) and our tactical situation, a damage control procedure was undertaken by approaching the transected right superficial femoral artery through the medial exit wound (Fig. 3). After identifying the two loose ends of the transected superficial femoral artery and confirming a 3–4 cm gap, a Sundt external carotid artery shunt (3.5 × 5 mm reinforced silastic shunt with 1 cm non-reinforced center segment, catalog number NL850-5077, NeuroCare Group/Heyer-Schulte and Integra Neurosciences, Plainsboro, NJ) was placed to restore distal perfusion (Fig. 4). The shunt was secured in place with Rummel tourniquets. Fogarty catheters were not available at this echelon of care on the battlefield and thus thrombectomy of the distal runoff was unable to be performed. After shunt placement the patient had palpable distal pulses. To prevent compartment syndrome, four compartment fasciotomies of the lower right leg were performed prophylactically (Fig. 5). The proximal control device at the right groin was left in place and the wound was packed in case of shunt dislodgement during transport. The soft tissue wounds of both extremities were then expeditiously debrided and the patient was moved to the intensive care section of the FST for further resuscitation and to await transfer to a higher echelon of surgical care for definitive repair while we sorted through the rest of our casualties that night and into the next morning.
Scene showing 250th Forward Surgical Team operating room and set-up for one-shot arteriogram. Each proximal common femoral artery was cannulated with small bore angiocatherter and renograffin used as contrast agent. Angiogram showing a normal left superficial femoral artery with no injury. Also note lack of contrast flowing in right superficial femoral artery that was shunted shortly after this film. High velocity GSW exit wound on right medial thigh with section of superficial femoral artery missing. Shunt has been placed, restoring flow to right leg. Secured in place with Rummel tourniquets. Prophylactic fasciotomy is performed.



Although the next echelon of care was only a three to four hour flight by C-130 Air Force transport plane to the Arabian Peninsula where a vascular surgeon was stationed, diplomatic clearance for this patient to enter the country was unable to be obtained. Resuscitation and post-op care was continued in the FST ICU. While awaiting transport, however, the patient's right pedal pulse diminished. He was immediately heparinized to insure shunt patency. This was accomplished using a 5,000-unit heparin bolus intravenously followed by a 1,000 unit per hour continuous infusion. With no coagulation studies available at our facility, the heparin infusion was adjusted based on clinical assessment of the dressings of his open wounds for active bleeding. After continued heparinization, the distal pulses returned to baseline. After 36 hours from the time of initial shunt placement, the patient was evacuated by a C-17 Air Force transport jet to Landstuhl Regional Medical Center (LRMC) in Germany. This 4,000 mile evacuation route added an additional 8 hours to the intraluminal shunt time. Approximately 48 hours after the shunt was placed the patient was taken to the operating room at LRMC where a final arterial reconstruction was performed by a vascular surgeon stationed there. A reversed saphenous vein graft was used for repair and continued debridement was performed. The temporary intraluminal shunt was found to be patent at the time of definitive repair. Prior to proceeding with the repair, an embolectomy catheter was used to insure that the distal artery was free of remaining clot. After repair, the patient had palpable pulses in the right lower extremity below the injury and an ankle brachial index of one.
Post-operatively he did well and underwent several debridements and an eventual skin graft to the right inner thigh. A subsequent duplex was performed which showed normal flow without kink, SFA 32 cm/s; proximal to graft 52 cm/s; proximal to the anastomosis 73 cm/s; distal graft 50 cm/s; distal anastomosis 80 cm/s; and the mid popliteal 59 cm/s. He was able to recover full function of both lower extremities, to include running, jumping and stair climbing. This soldier was eventually repatriated back to his home in the Kandahar region of southern Afghanistan.
Discussion
This case is the longest reported transport of a patient with a temporary intraluminal arterial shunt that remained patent and concluded in successful revascularization and limb salvage. Fifteen years ago Johansen and Hedges reported the transfer of a patient with severe multi-system trauma, to include hemi-section of the right mid-thigh and distal limb ischemia, over a 950-mile route from Juneau, Alaska to Seattle, Washington. 9 Time of injury to time of shunt placement was 3 hours, and, remarkably, the time of injury to the time of definitive repair was only 16.5 hours. Despite this heroic effort and successful reperfusion with distal flow after shunt placement, the patient's injuries did not permit limb salvage and amputation of the effected extremity ensued. In that case, reperfusion injury and the lack of prophylactic lower leg fasciotomies were sited as a possible contributing factors in the loss of the limb.
Temporary intraluminal shunting has proven useful in the management of acute arterial trauma with limb ischemia especially in damage control settings. Shunts allow distal tissue perfusion while other, more life threatening head, chest and abdominal injuries are addressed. They are advocated for extremity injuries where there is concomitant soft tissue, vascular and fracture injury. In this type of injury, after proximal and distal control are established, an arterial shunt is placed to provide temporary perfusion while the orthopedic surgical team applies fracture stabilization and further debridement. Fracture management manipulation can cause dislodgement of the shunt, or worse, if the arterial repair is performed first, damage or kinking of the interposition graft or anastomotic disruption. After completion of other procedures and/or the patient is stablized in the ICU, vein is harvested from a non-traumatized extremity and a definitive repair performed. During definitive repair, most recommend clearing the distal and proximal vessels with embolectomy catheters. 10 Fasciotomies are recommended for cases of long ischemia times, concomitant venous injuries and/or direct multiple penetrating wounds resulting from blast or high velocity missiles.10,11 We also advocate the liberal use of prophylactic fasciotomies for arterial trauma requiring temporizing measures in the far-forward environment especially in the setting of prolonged evacuation routes due to the possible lack of surgical intervention and the possibility of shunt thrombosis.
Concomitant heparinization to insure shunt patency can be used and in our case was used after the patient had stabilized in the ICU. Animal studies have shown that shunts can remain patent for up to 24 hours without systemic heparinization. 12 Heparinization in general should be used, however, to prevent shunt thrombosis either locally in the shunt itself or systemically.
Use of “one-shot” arteriograms in the far-forward area can be helpful and in this case was actually time saving. Here we were able to avoid exploration of the patient's left SFA even though he had soft signs of arterial injury (location of wound, diminished distal pulse). We have used arteriograms and venograms in 5 cases in the far-forward environment both for triage purposes and for diagnosis and subsequent repair of vascular injuries. It is easy to duplicate this capability in the rural emergency room.
Thus far there have been few specific reports coming out of the Global War on Terror on the successful use of shunts in the combat setting.7,8 In 2005, Brusov and Nikolenko reported on the Soviet experience of vascular injuries from 1981–1985 in the war in Afghanistan. 11 Although there is no mention of a specific rate of shunt thrombosis, they reported the placement of 33 shunts for forward damage control situations and 38 cases of shunt use for limb reperfusion while performing other operations (i.e. orthopedic stabilization of an extremity). Definitive vascular repairs were then performed and only 2 amputations were necessary when a shunt was used indicating a high rate of ultimate limb salvage. Follow-up data on limb function was not reported. In their report shunt placement ranged from 10 to 36 hours and use was restricted to tactical or local evacuation in that all patients with shunts in place were transported and treated within the borders of Afghanistan.
When in a far-forward environment, especially in the instance of unusually long lines of communication and evacuation routes, limited personnel and resources, combined with sudden mass casualty situations, the use of simple techniques for abbreviated operations may be helpful and are often the default. 13 In the case described above, the use of the shunt was mandated by both the patient's injury and the tactical situation. Though primary repair of the right SFA was anticipated to be sooner and can be done in a far-forward environment, it is not always prudent or possible. Shunts and abbreviated operations are also mandated when forward surgical teams are following the rapid advance of mechanized units such as what occurred in the beginning of Operation Iraqi Freedom. Those FSTs sometimes had to take care of casualties without having the luxury of setting up a full operating room. 14 Significant delay in transport to a facility with the appropriate level of resources occurs due to geographic distances, weather or transport of severely injured patients to facilities that are poorly equipped to treat the patient. Such delay in instituting definite care necessitates rural surgeons to be able to perform temporizing and stabilizing measures, such as temporary intraluminal shunts to restore lower limb perfusion and such cases have been reported. 4
With more complex lower limb vascular injuries occurring in both the military and civilian settings and the need for restoring arterial flow quickly, damage control approaches with the use of shunts is a viable method to enhance limb salvage.
Footnotes
Acknowledgement
The authors extend great thanks and appreciation to the non-commissioned officers, nurses and medics of the 250th Forward Surgical Team (Airborne) because without their hard work and dedication to duty this mission would never have been a success. Their names are: Glen Carlsson, Mike Saddler, Brad West, Jim Rigot, Derek Forrest, Robert Novak, Beecher Whiteaker, Able Tavarez, Darrell Joshua, Robert Burns, Chris McGowan, Scott Coleman, Alex Lofton, Dwayne Coble, Alfredo Ramos, Gwendolyn McFadden, Seth Cuneen, and Darrell Dodge. Seth Cuneen photographed most of the events included in this manuscript.
The authors report no conflicts of interest.