
Abstract
Background
There is controversy about the appropriate treatment for severely displaced and unstable comminuted fracture of distal radius (type C of AO or OTA classification). Recently, there has been an increase in the number of predilection for surgical management of this fracture.
Aim
To determine the radiographic outcome in type C fractures of the distal radius treated with closed reduction and pin in plaster.
Materials and Methods
Eighty consecutive patients 60 male and 20 female, average age 40 years (22–60 years), with type C fractures of the distal radius seen between February 2001 and July 2003 in Shahid Kamiab Hospital of Mashad University, were treated by closed reduction and pin in plaster, followed up by anteroposterior and lateral radiographs to evaluate radial height, inclination and volar tilt.
Results
There was significant improvement in the measurements of radial height, inclination and volar tilt after closed reduction and pin in plaster, and at the time the pins and plaster were removed. (P = 0.00).
Conclusion
Closed reduction and pin in plaster is an effective, simple and low cost method in type C fractures of distal radius with satisfactory outcome.
Introduction
Fracture of distal radius is one of the most common injuries encountered by the orthopedic surgeon. This fracture is predominant in elderly patients with low functional demands and significant osteoporosis. 1 Recently, there has been an increase in the number of high-energy fractures of the distal radius (severely displaced and comminuted) seen in young adults, because of motor vehicle accidents and sports activities. 2
There is controversy about the appropriate treatment for severely displaced and unstable comminuted treatment fractures of distal radius (type C of AO or O.T.A classification). 3 Recently, there is a high incidence of fractures of distal radius in young adults, resulting in documentation of the surgical management of these injuries. 2
Surgical treatment (open reduction and internal or external fixation) introduce additional surgical trauma, and incision of important capsular and ligamentous structures may be associated with a high complication rate. 9
Non surgical treatment (closed reduction and plaster immobilization, closed reduction and percutaneaus pin fixation, pin in plaster fixation as well as fixation with an external fixator) are less invasive methods and have no additional soft-tissue (capsule and ligaments) injuries,16–17 but suffer from the inability to reduce depressed articular fragments.5–15 The purpose of this study is to determine the radiographic outcome in type C fracture of the distal radius treated with closed reduction and pin in plaster.
Materials and Methods
This was a prospective study of 80 consecutive patients (60 male, 20 female) with distal radius fractures (type C of AO or OTA classification) treated by closed reduction and pin in plaster between February 2001 and July 2003 in the Orthopedic Department of Shahid Kamiab University Hospital.
The mean age was 40 years (range from 22–60 years).
Thirty five fractures occurred on the left side and forty-five fractures on the right side.
All fractures were type C according to AO classification. Thirty fractures were group C1, 34 were group C2, and 16 were group C3 (Table 1).
Clinical data for 80 patients with distal radial fractures treated by closed reduction and pin in plaster.

Closed reduction and pin in plaster were performed a mean of 3/5 days (range from 1 to 16 days) after the injury. Six patients who required open reduction to reduce depressed or displaced articular fragments were excluded from the study. Also, 5 patients who were from other cities and were not available for follow up were excluded.
Technique of pin in plaster (traction cast) consists of:
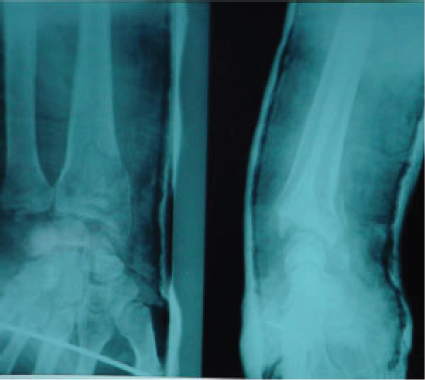
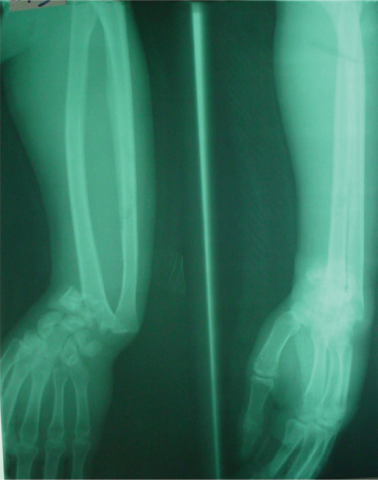
Traction by Chinese finger tap, approximately 5 minutes, after adequate anesthesia (general anesthesia). Gentle manipulation of fracture. A 2.4 mm Steinmann pin insertion through the proximal ulna (or middle third of radius) and second pin through II, III metacarp. Application of plaster cast to above the elbow, incorporation the two pins in plaster Molding the cast. (Figs. 1, 2, 3, 4).
A 47 years old man with type C 3 distal radial fracture due to falling down. Case 1 after closed reduction and pin in plaster application. Case 1 after removal of pin and plaster. A 35 years old man with a type C 3 distal radial fracture Due to motor accident.


The pins and plaster were removed after fracture union at a mean of 45 days (range from 40–60 days). All the patients followed up by A.P and lat. Plain radiographs per two weeks, but the radial height (12 mm), radial inclination (23 degrees) and volar tilt (11 degrees) (Fig. 1), was evaluated at the initial visit, immediately post reduction and the time of pins and plaster removal (without cast). patients who had received open reduction and internal fixation or external fixation, and who were unavailable for follow up, were excluded from the study. The differences between various mesurements were evaluated by student's t-test and statistical significance between pre reduction and post reduction was defined as p value. The mean follow up duration was 81 days (75–94 days).

Case 2 after closed reduction and pin in plaster application.

Case 2 after pin and plaster removal.
Results
There was a significant improvement in the measurements of radial height, radial inclination and volar tilt after closed reduction and pin in plaster, and at the time the pins and plaster were removed. The measurements of the three intervals were stationary, and the reduction was lost minimally at the time of pin and plaster removal (Fig. 2).
The radial height improved from an average of 62.9 mm to an average of 108.9 mm (t = 13.7, p = 0.000), the radial inclination improved from an average of 11.7 deg. to an average of 20.1 deg. (t = 22.86, p = 0.000), and the volar tilt improved from An average of -5.7 deg. to an average of 6.4 deg. (t = 26.8, p = 0.000).
The mesurements were stationary until pin and plaster removal, so, differences between prereduction and postreduction, prereduction and at the time of pin and plaster removal for radial height, inclination and volar tilt were significant (p = 0.000) (Table 2).
Distal radial measurements as determined by radiography at the three intervals (pre reduction, post reduction, pin plaster removal) Differences between pre reduction and post reduction, pre reduction and pin and plaster removal for radial height, radial inclination and palmar tilt were significant.

We had only 5 cases of pin infection who were treated by oral antibiotic therapy.
We had no other complications such as nerve and vascular injury.
Discussion
The current treatments for severely displaced and unstable fractures of distal radius (type C, AO or O.T.A classification) consist of:
Closed reduction and pin in plaster (traction cast) (CRPP). Closed reduction and external fixator (CREF). Open reduction and external fixator (OREF). Open reduction and internal fixator (ORIF).
The lack of clinical data on the relative indication of various treatment methods and lack of randomized study of fixation methods and results for a specific type of distal radius fracture, make impossible recommending one treatment over another. 12
Recently, most orthopedic surgeons agree with surgical management (OREF or ORIF) of type C fractures of distal radius, particularly in young adults, for restoration of bone anatomy (reduction of displaced or depressed articular fragments). 2
Several studies clearly showed that restoration of the radial length, inclination and palmar tilt are the most important factor in achieving a good end result particularly in young adults.2,4,9,10,13,14
The pin in plaster method as a simple form of external fixator acts as a means of neutralizing the forces that lead to shortening and collapsing of the distal radius after reduction. 12
This study showed the efficacy of closed reduction and pin in plaster method in restoration and maintenance of anatomy of distal radius (radial length, radial inclination, radial palmar tilt).
Many other reports of efficacy of C.R 8 pin in plaster have been published for more than 50 years.12,14–16
This method has some disadvantages including.12,13
Inability to achieve direct reduction (specially depressed articular fragments) Long time immobilization of the radio ulnar and radio carpal joints Pin tract infection.
Conclusion
Closed reduction and pin in plaster is an appropriate treatment for severely displaced and unstable fractures of distal radius (type C of AO or O.T.A classification) that leads to good radiographic results with respect to radial height, radial inclination, and radial tilt. This method is also suitable because of its low cost and simplicity.
Footnotes
The authors report no conflicts of interest.