
Abstract
Intramedullary nailing of metaphyseal and segmental tibia fractures can be technically challenging for a variety of reasons. Restoring length, alignment and rotation of the injured limb requires careful preoperative planning and meticulous attention to surgical technique, while avoiding common pitfalls. Understanding the deforming forces on the fracture segments and normal tibial osteology provides a background for recognizing the most common pitfalls when nailing these fractures. Many adjuncts for obtaining and maintaining fracture reduction while nailing have been described, including extended positioning, use of the femoral distractor, blocking screws, and provisional plating. We discuss these techniques as well as the role of intramedullary fixation for treating metaphyseal fractures with articular extension. The purpose of this paper is to describe the background and technique for a variety of operative tips and tricks to facilitate intramedullary nailing of metaphyseal and segmental tibia fractures.
Introduction
Tibia fractures are the most common long bone injury in the lower extremity, resulting in more than 70,000 hospitalizations and 800,000 office visits annually in the United States. 1 Injury patterns range widely, from low-energy spiral patterns to high-energy, open segmental fractures. Contemporary management involves intramedullary (IM) nailing for the majority of extra-articular fracture patterns as this strategy minimizes soft tissue dissection and preserves fracture biology while optimizing biomechanics. While the standard care for primarily intra-articular patterns involving the tibial plateau or plafond with meta-diaphyseal extension remains plate osteosynthesis, IM nailing is also being utilized for proximal and distal metaphyseal tibia fractures, even those with associated simple articular fractures.
The goal of treatment in tibia fracture management includes the restoration of length, alignment, and rotation, and achieving these goals can be particularly difficult in the setting of complex fractures, particularly metaphyseal, segmental, or extensively comminuted patterns. 2 Understanding the tibial osteology, deforming forces, surgical approaches, and implants is critical when developing strategies for reduction and IM nail fixation. The purpose of this article is to review the complexities inherent to IM fixation of complex tibia fractures and to describe tips and tricks to optimize outcome.
Proximal Tibia Tips and Tricks
The unique osteology of the proximal tibia makes IM nailing of fractures in this region inherently difficult. Furthermore, the proximal segment is subjected to dynamic deformation by several joint-spanning muscle groups that results in predictable patterns of displacement. Historically a failure to understand and address these issues resulted in a high incidence of complications, with a malunion rate approaching and even exceeding 80% in some series.3,4
The extensor mechanism creates an isolated vector anterior to the proximal segment leading to an apex anterior or procurvatum deformity, which is exacerbated by the pull of the gastrocnemius on the distal femur. Standard positioning for IM nailing with the knee hyperflexed over a tibial triangle only serves to worsen this deformity. The pes anserinus tendon insertion on the medial aspect of the proximal segment is largely unopposed laterally, generating a net valgus moment in the coronal plane. Because of the large mismatch between the size and shape of the tibial canal and a medullary nail, the passage of the nail itself will neither affect nor maintain an appropriate reduction.
A precise nail starting point and trajectory as well as an accurate fracture reduction are critical in preventing malreduction during nail insertion. The isthmus of the tibial canal is lateral to the midline of the plateau, and the starting point should correspond with this. This starting point should be just medial to the lateral tibial spine as judged on an appropriate anterior posterior (AP) view of the knee in which the lateral cortex of the tibia bisects the fibular head.5,6 Medial translation of the start site will not only exacerbate the valgus deformity with nail insertion but also risks injury to the anterior horn of the medial meniscus. 7 To maximally neutralize the apex anterior vector, the entry wire should be inserted parallel to the anterior cortex of the tibia.
Semi-extended nailing is an effective method for neutralizing the deforming force from the extensor mechanism and optimizing imaging as a starting point is established. Several techniques have been described in the literature. Tornetta utilized a lateral parapatellar approach with subluxation of the patella and intra-articular nail insertion to achieve satisfactory post-operative alignment in a series of proximal 1/3 tibia fractures. 8 An extra-articular modification of this technique using either a medial or lateral parapatellar approach without violation of the knee joint capsule has also been described. 9 Recently the suprapatellar approach has gained popularity for nailing in the extended position. Guidewires, reamers, and the nail are introduced percutaneously through the quadriceps tendon and behind the patella using specifically designed cannulas (Figs. 1A and B), with no apparent increased risk of damage to intra-articular structures or knee pain compared to standard nailing in hyperflexion.10–13 All of these approaches are appropriate for semi-extended nailing and may be chosen based on the surgeon's preference, available equipment, or individual patient anatomy. Medial and lateral parapatellar approaches have the advantages of not requiring specialized equipment.
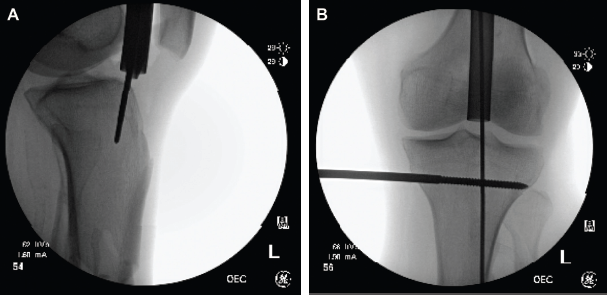
Specially designed protective cannulas should be used when nailing via the retropatellar approach.
Many adjuncts for achieving and maintaining reduction have been described, with the most commonly employed techniques being femoral distractor application, percutaneous clamping, and formal open reduction with or without provisional plate application as well as blocking screw deployment. The femoral distractor should be placed medially, taking care to insert Schanz pins parallel to the plateau and plafond, respectively, to prevent introduction of coronal plane deformity and posterior to the long axis of the tibia so as not to obstruct the nail and to help reduce any procurvatum deformity (Figs. 2A–C). Percutaneous clamps can be very effective in maintaining the reduction of simple fracture patterns during nailing (Fig. 3). Formal open reduction can also be performed without adverse sequelae, provided meticulous soft tissue handling is performed. 14 Open fractures in which the fracture site is exposed as part of the debridement also provide an excellent opportunity for a direct reduction. When an open reduction is performed, provisional plate application should also be considered (Figs. 4A–D). While originally described for use in open fractures, the technique can be applied to difficult closed metaphyseal and segmental fractures so long as the surgeon takes care to avoid excessive stripping; supplemental plates can be used provisionally as a reduction aid only or as a permanent part of the construct. Choice of implant depends on the fracture pattern and goal of the construct, but may be a 1/3 tubular, 2.7-mm or 3.5-mm dynamic compression plate (DCP) plate. If the implant is to be retained, every effort should be made to place it in an area with robust soft tissue coverage. Several studies have verified the safety and efficacy of this technique.15,16

The femoral distractor should be placed medially (

Percutaneous clamping can be used alone or in combination with other adjuncts to aid in reduction.
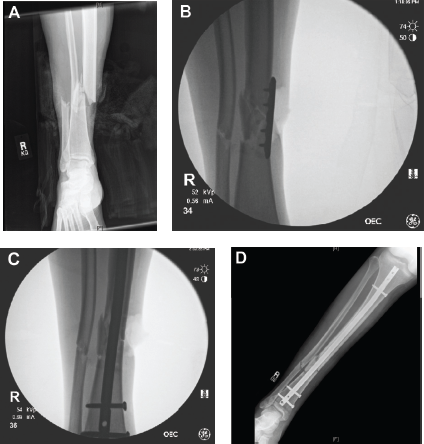
Supplemental plate fixation being used to facilitate and hold the reduction during nailing.
The final adjunctive technique in nailing proximal fractures is the use of blocking screws, which function to constrain the path of the nail, preventing angulation and translation with nail insertion (Figs. 5A–G). They have been shown to be biomechanically and clinically advantageous in locations such as the proximal tibia where there is a large mismatch between nail and canal diameter.17–19 In the proximal tibia, the nail will tend toward the posterior and lateral cortices so blocking screws are ideally placed in these locations just adjacent to the desired nail path. A drill bit, 3.2-mm Schanz pin, 3.5-mm screw, or an interlocking screw from the tibial nailing system can be utilized. The drill bit or Schanz pin should be replaced by a screw after successful nail passage. If using a femoral distractor, the proximal pin may be used opportunistically as a blocking screw as well. 20

A blocking screw placed lateral to the nail path in the proximal segment serves to prevent valgus angulation during nail insertion.
Segmental and Extensively Comminuted Fractures
Anatomic restoration of length, alignment, and rotation can also be especially challenging in segmental fractures, extensively comminuted fractures, and those with bone loss. Several steps in the pre-operative planning process can facilitate successful surgery. If difficulty in assessing appropriate limb length is anticipated, full-length radiographs of the uninjured side can be obtained to serve as a reference. Fluoroscopic images of the contralateral knee and ankle can also be obtained and used to guide rotation, as is frequently done in the femur. In difficult cases the surgeon should consider prepping the contralateral limb into the field for direct comparison.
Intraoperatively, a femoral distractor can be very helpful for restoring length. In diaphyseal fracture cases in particular, it is critical to place distractor pins parallel to the knee and ankle joints and outside of the nail path to facilitate reduction and allow nail passage. Many surgeons find it helpful to use an electrocautery cord placed fluoroscopically in the center of the femoral head and ankle joints to judge the mechanical axis of the limb, but it is still critical to obtain full length intraoperative radiographs prior to breaking down the sterile field in these cases. In the case of an open fracture with extruded or devitalized segments, Nork has described using these segments as a reduction aid rather than immediately discarding them as the traditional principles of open fracture treatment might dictate. 21 Alternatively, these segments can be soaked in chlorhexadine solution and used as a template to guide reduction, either by clamping or provisional plate fixation. Once the nailing procedure has been completed the devitalized fragments can then be discarded. If the fracture is to be managed in a staged fashion, devitalized segments can be washed, autoclaved, and then frozen at the time of external fixation for later use as templates during the definitive reconstruction. The resultant bone defect can then be managed according to surgeon preference, typically with antibiotic beads or a spacer followed by delayed bone grafting.
Distal Tibia Tips and Tricks
Unlike fractures of the proximal tibia, patterns of displacement are less predictable in the distal tibia and depend primarily on the mechanism of injury, resulting fracture configuration, and the location and degree of comminution. The Robinson classification can be helpful in understanding how various patterns will behave and the likelihood of articular involvement. 22 As in the proximal tibia, semi-extended nailing, femoral distractor, percutaneous clamps, open reduction, provisional plating, and blocking screws can be very helpful. The nail insertion portal is less critical in distal fractures but guidewire placement should be deep and central on both AP and lateral views. The main advantage of a semi-extended strategy for distal fractures is the ease of imaging and avoiding excessive manipulation of the limb in the setting of a tenuous clamp application.
Particularly relevant to the distal tibia is the opportunity to reduce and fix the fibula. This can be especially helpful in valgus fracture patterns and in the setting of simple fibula fractures where accurate restoration of length of the lateral column will help to combat valgus and guide appropriate restoration of length and rotation of the tibia.23,24 Some length-stable fibula fracture patterns are appropriate for closed retrograde medullary nailing using a titanium elastic nail or guidewire, while length-unstable patterns may be better addressed with formal open reduction and plate fixation.25,26 Indications for IM fixation of the fibula include a compromised soft tissue envelope that precludes formal open reduction with internal fixation (ORIF) as well as axially stable fracture patterns. 26
Advances in nail design have also led to improved fixation of distal fractures. Angle-stable or multidirectional distal interlocking screws are now available and have been shown to enhance construct stability.27–31 Attal et al recently evaluated the biomechanics of multidirectional and conventional interlocking screws with and without fibular fixation in a cadaveric model. These authors found a small yet significant improvement (P = 0.013) in construct stability with addition of fibula fixation to a conventionally locked nail but no difference in stability in the multidirectional system whether the fibula was addressed or not. These results highlight the improved stability that comes with multidirectional locking and suggest that fibular fixation in distal tibia fractures may not be necessary unless the ankle mortise is unstable or fibular fixation is being used as a reduction tool. 28
As mentioned, open treatment of the fibula is not without risks and should be considered carefully, particularly in patients with diabetes, peripheral vascular disease, and in the setting of a heavily traumatized soft tissue envelope. Some surgeons’ additional concern with fibula osteosynthesis is creating an overly stiff construct with the potential for inducing a tibial non-union, although there is no definitive evidence to support this in the literature.
Articular Involvement
Simple articular fracture extensions into either the knee or ankle joints are not contraindications to medullary nailing.32,33 When addressing these fractures, it is critical to adhere to the principles of articular fracture management, which dictate that the articular component be addressed with anatomic reduction and compression followed by restoring the mechanical axis of the limb. Ipsilateral fractures of the tibial plateau and shaft are relatively uncommon, and careful planning is necessary when combining plate osteosynthesis and IM nailing for these injuries. 33 The articular fracture must be addressed first and the anticipated nail insertion site must not involve the fracture. The subchondral lag screw trajectory cannot interfere with the nail path. Once the articular reduction is obtained, the buttress plate should be fixed distally with unicortical screws and after nail passage exchanged for bicortical screws passing either anterior or posterior to the nail. The surgeon must take caution when inserting the nail to prevent displacement of the articular component (Figs. 6A and B). Tibial plafond fractures associated with distal metaphyseal tibia fractures are far more common than the proximal variant. These injuries are typically a result of a lower energy torsional mechanism and the articular injury can be subtle. 34 Recognizing these patterns is important, as IM nailing without first identifying and addressing the articular pattern can displace the articular fragment during nail insertion. CT scanning should be strongly considered when a rotational distal meta-diaphyseal tibia fracture is identified. These fractures are typically amenable to percutaneous lag screw stabilization prior to nailing. 32

Combined strategies to address a noncontinuous tibial plateau and diaphyseal fracture require careful implant placement.
Summary
While metaphyseal and segmental or highly comminuted tibia fractures pose inherent difficulties for IM fixation, there are a variety of strategies available to facilitate appropriate reduction and fixation. Early failures with IM nailing have taught us that understanding relevant anatomy, both the dynamic deforming forces and the tibial osteology, is critical. Semi-extended positioning neutralizes the extensor mechanism's deforming force and greatly simplifies intraoperative imaging. A proper start site ensures maintenance of reduction as the nail engages the isthmus during insertion and avoids injury to the menisci. Use of the femoral distractor, percutaneous clamping, blocking screws, and supplemental plate fixation are strategies to consider during nailing and may be used in combination to optimize the radiographic and functional outcome of the patient. ORIF of the fibula can assist in restoring length, correcting valgus alignment, and providing an indirect tibial reduction. Simple articular extension is not a contraindication to IM fixation, but must be addressed with anatomic reduction and interfragmentary compression prior to nailing. The majority of evidence supporting these techniques is level IV and V. As IM nailing becomes increasingly common for these difficult-to-treat patterns, large-scale prospective studies will be useful in identifying the subtle yet important differences these techniques have in outcomes and complication rates in these cohorts.
Author Contributions
Conceived the concepts: MG and JB. Analyzed the data: MG and JB. Wrote the first draft of the manuscript: MG and JB. Contributed to the writing of the manuscript: MG and JB. Agree with manuscript results and conclusions: MG and JB. Jointly developed the structure and arguments for the paper: MG and JB. Made critical revisions and approved final version: MG and JB. All authors reviewed and approved of the final manuscript.