
Abstract
The care of multiply injured patients with orthopedic injuries has evolved from prolonged periods in traction to early total care (ETC). ETC is advantageous in ease of nursing care and aiding patient recovery. However, concerns have been raised that this ‘second hit’ of surgery places these severely injured patients at risk of excessive inflammatory responses that can lead to systemic inflammatory response syndrome (SIRS). Damage control was initially used in abdominal trauma but has been adapted for use in orthopedics. The mainstay of treatment involves external fixation of long bone and pelvic fractures which acts to defer definitive fixation until physiologic stability is restored. The indications for implementing each approach are not clear and this article provides a narrative review of the topic.
Introduction
The management of multiply injured trauma patients has both changed and improved over the last 30 years. The dissemination of the advanced trauma life support principle 1 to the multidisciplinary team provides a systematic and uniform approach to the assessment of trauma patients. Furthermore, the implementation of regional trauma networks has focused the treatment of these patients at specialist centers where resources and specialist teams are available to correctly manage multiply injured patients.
Traditionally, treatment consisted of traction for a prolonged period as this group was deemed too unwell for major surgery. 2 However, these patients, particularly those with more severe injuries, are at risk of multiple complications including adult respiratory distress syndrome (ARDS), infection, pneumonia, malunion, nonunion, and death. 3 This led to the introduction of the “early total care” (ETC) which involved early operative stabilization of long bone and pelvic fractures. The aim of this aggressive management was to aid nursing care, reduce complications, and improve patient recovery. However, the risk that this additional surgical insult may contribute to a systemic inflammatory response (SIR) led to the development of the “damage control orthopedic” (DCO) approach. This involves temporarily splinting long bone and pelvic fractures with external fixation while the patient's physiology recovers from their initial trauma. However, controversy still exists on how to decide which patients would benefit from each approach and this article gives a narrative review of the topic.
Physiology of Trauma
Severe trauma with fracture of long bones results in tissue injury and the intravasation of medullary fat and marrow into the systemic circulation, which triggers excitation of the coagulation and inflammatory pathways.4,5 Systemic inflammation has the benefit of readying the body for action by increasing blood supply and increasing delivery of white cells. However, the body treads a fine line with overreaction leading to ARDS or multi-organ dysfunction syndrome (MODS). 6 A counter-regulatory mechanism is present but loss of control in severe trauma can lead to ARDS and MODS. Additional surgical treatment can also induce an inflammatory response but in a healthy patient with an isolated injury this has no consequences. However, in multiply injured patient the second hit of surgery can cause an excessive inflammatory reaction with subsequent development of systemic inflammatory response syndrome (SIRS), ARDS, and MODS.
The important host factors that influence inflammation are the cytokines, leukocytes, and endothelium. 7 Previous studies have shown a rise in IL-6, IL-8, C-reactive protein levels, and neutrophil elastase during the acute phase of trauma.8,9 The level of IL-6 has also been shown to have a greater rise in patients undergoing ETC compared to DCO. 10 This supports the concern that patients undergoing ETC are subjected to a second inflammatory “hit” that may trigger ARDS, as their lungs have been primed by the initial injury to the capillary endothelium associated with shock from systemic injuries. In this scenario, the embolization of fat and marrow contents during intramedullary instrumentation stimulates further inflammation with the potential loss of control leading to SIRS.
Early Total Care
Studies from the 1980 and 1990s reported that early stabilization of femoral shaft fractures was beneficial in polytrauma patients.11–13 Early fracture fixation has been shown to decrease the duration of ventilation, decrease the time in the intensive care unit, decrease the rates of ARDS, fat embolism syndrome, multiple organ failure, and late sepsis, decrease the overall length of hospitalization, and reduce the cost of medical care.11–17 These patients are at risk of suffering from various respiratory complications that develop over the first few days and a window of opportunity for early stabilization may be available in the first 24 hours. One randomized trial comparing ETC and DCO in 83 patients with an injury severity score (ISS) of greater than 18 reported that the group with early stabilization had fewer pulmonary complications, shorter hospital stay and number of days spent in the intensive care unit and on a ventilator, and a substantial cost savings. 14 A meta-analysis demonstrated a large relative risk reduction (relative risk, 0.30; 95% confidence interval, 0.22–0.40) in respiratory complications in association with early operative fixation (usually within 24 hours). 4
Damage Control Surgery
The principle of damage control surgery was first proposed in the context of general surgical trauma in 1993. 18 The principle is to address major injuries first before transfer to intensive care for stabilization when definitive surgery can be managed. DCO uses this same principle and involves the external stabilization of pelvic and long bone fractures. This approach minimizes operative time and blood loss while facilitating nursing care and earlier mobility.14,19 DCO allows definitive treatment to be deferred until physiologic stability is restored mitigating the risk of secondary lung injury. 20 Studies have shown that DCO treatment is associated with a lower SIR than after ETC. 21 Harwood et al performed a multi-centered randomized controlled trial of 35 polytrauma patients with ISS scores over 16 and long bone fractures reporting that serum inflammatory markers were increased in those undergoing ETC. 10 Specifically regarding pelvic injuries, the rationale for early pelvic stabilization is to restrict pelvic volume and to encourage tamponade reducing blood loss. However, DCO procedures are not definitive and consideration should be given over when the patient should return for definitive treatment as well as a higher risk of infection from the pin tracts.
Chest Injuries
The safety of long bone fixation in patients with pulmonary injuries is controversial. The presence of pulmonary contusions has been shown to be a good independent predictor of the development of ARDS and pneumonia.22,23 Therefore, the addition of a second hit from a surgical intervention in patients with these additional pulmonary injuries is thought to carry a higher risk of respiratory compromise. Pape et al performed a retrospective review of 106 patients with multiple injuries and reported that early intramedullary nail fixation in those patients with a severe chest injury was associated with an increased risk of both ARDS and death. 24 However, the findings from the literature are not consistent with a retrospective review from Charash et al of 138 patients reporting that the complication rate from delayed intervention is higher (56%) when compared to early stabilization (16%). 25 Therefore, patients with the combination of a serious chest injury and femoral fracture require a multidisciplinary decision regarding the timing and type of surgical intervention, while needing close monitoring during fracture fixation.
Head Injury
Patients with head injuries are well known to be at risk of secondary brain injury if exposed to hypotension, hypoxemia, or increased intracranial pressure. Principles of management include the maintenance of mean arterial pressure and oxygenation to ensure adequate cerebral perfusion. Surgical intervention risks periods of both hypoxia and hypotension with the subsequent secondary brain injury and this may be linked to a poorer neurologic outcome. These patients require appropriate resuscitation and careful monitoring of blood pressure, oxygenation, and intracranial pressure during surgery. In addition, discussion among traumatologists, intensivists, and neurosurgeons should decide on optimum timing in each individual case.
Many studies have retrospectively analyzed patients with the combination of head injury and long bone fractures. Jaicks et al reviewed 33 patients and reported that after early fracture fixation, fluid requirements were greater, more suffered from hypotension and intraoperative hypoxia, and the Glasgow Coma Scale score was lower on discharge than in patients who had delayed fracture fixation. However, those with delayed fixation had more neurologic complications and stayed longer in the intensive care unit. 26 Similarly, Townsend et al retrospectively reviewed 61 patients with severe or moderate closed head injury and femoral fractures and demonstrated an eight-fold increase in the risk of intraoperative hypotension if the operation was carried out within two hours of admission to hospital and a two-fold increase if the operation was carried out within 24 hours of admission. 27 In contrast, Starr et al reported a 45-fold increase in pulmonary complications with delayed femoral fixation compared with immediate fixation. They also demonstrated that the risk of central nervous system complications and death was increased in the delayed fixation groups. 28 A review of cases series concluded that patients with brain injury who underwent long bone stabilization within 48 hours were similar to those treated with later stability in terms of mortality, length of stay in ITU, and need for mechanical ventilation. 29
Decision Making: Early Total Care or Damage Control Orthopedics
Deciding when and how to definitively fix long bone fractures in polytrauma patients remains controversial. The evidence discussed is contradictory and the majority of evidence originates from retrospective reviews. Therefore, careful consideration should be given to each individual case and a multidisciplinary team approach to decision making should be adopted. This is beneficial in both prioritizing the injuries that are life and limb threatening while ensuring intervention is performed at the optimal time.
Pape et al randomized 165 patients to receive ETC or DCO and although showed very little difference between the groups, the authors did report a five-fold increase in acute lung injury in the “patients at risk.” 30 These findings suggested that a subgroup of patients may benefit from the DCO approach and further research has analyzed which parameters could be used to recognize this at risk group. Bone et al set out four factors that put ETC patients at high risk and these are shown in Table 1. Stubig et al demonstrated that patients with a high ISS (of 25–39) had a tendency toward a higher incidence of ARDS when treated with ETC compared to DCO, whereas in less severely injured patients ETC showed benefits. 31 However, the ISS is not often calculated on admission and is not a direct measurement of a patient's physiological status.
Patients at risk from early total care. 33

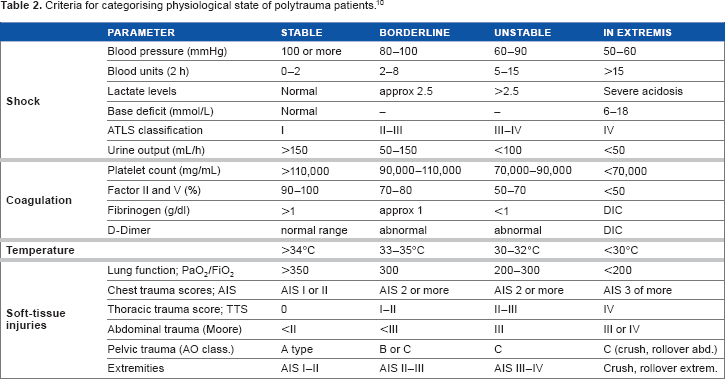
Pape et al. defined criteria that divide polytrauma patients into those that are “stable,” “borderline,” “unstable,” and “in extremis” and these criteria are outlined in Table 2. The authors recommend that those patients who are deemed stable are able to have ETC, those who are unstable or in extremis should have DCO, and if uncertainty exists over the borderline cases then they should also undergo DCO. 10 Further work has been carried out to simplify the decision making process as the criteria described are complex. Some authors suggest that stabilization has been achieved when the patient has good oxygenation and urinary output, and at this point it is safe to proceed with definitive stabilization of the long bone fractures.2,32 O'Toole et al focused on the measurement of lactate as a tool in deciding if patients with multiple traumatic injuries were adequately resuscitated. Their approach is to perform reamed nailing after adequate resuscitation shown by normalizing lactate, plus optimized ventilatory, and hemodynamic parameters. 20 The authors do not recommend treating those with lung injury differently.
Criteria for categorising physiological state of polytrauma patients. 10
Conclusion
The ETC and DCO approaches are both routinely employed in the management of polytrauma patients with orthopedic injuries. The majority of patients are likely to benefit from ETC but a subgroup of “at risk” patients are best managed using the DCO principle. The use of ISS, lactate, ventilation, and hemodynamic parameters can aid the identification of this subgroup.
Author Contributions
Conceived the concept: RWJ. Wrote first draft of manuscript: RWJ. Contributed to writing of manuscript: RWJ, GC, MD. Agree with manuscript results and conclusions: RWJ, GC, MD. Jointly developed structure and arguments of paper: RWJ, GC, MD. Made critical revisions and approved final version: RWJ, GC, MD. All authors reviewed and approved the final manuscript.