
Abstract
Background
Trauma patients in rural areas are frequently transferred to regional trauma centers for expeditious evaluation and management of potentially life-threatening injuries. We sought to characterize how long the process takes, once it has begun, for acutely injured patients to be transferred from emergency departments (EDs) of referring hospitals to trauma centers and how the time is spent.
Methods
We conducted a retrospective multi-institutional case series study. We reviewed records of acutely injured trauma patients transferred from the EDs of 114 outlying hospitals to the EDs of three Level I or II regional trauma centers over a 12–24 month period. We calculated the duration of the transfer process and its component time intervals (reported as the mean ± standard deviation).
Results
Among 1099 patients transferred from 114 referring hospitals, the mean Injury Severity Score was 11.6. Mortality was 5.9%. Half of all transfers were by ground ambulance, 36% by helicopter, and 13% by airplane. The mean time from patient presentation at the ED of the referring hospital until transfer request was 126 ± 94 min, and the mean time from transfer acceptance until arrival at the trauma center was an additional 119 ± 60 min. The mean time from transfer acceptance to departure of the patient from the ED of the referring hospital was 68 ± 48 min. Transportation time accounted for 48 ± 29 min, or 40% of the total time between transfer acceptance and arrival at the accepting hospital.
Conclusions
Interhospital transfer of acutely injured trauma patients takes a substantial amount of time even after acceptance of the patient, and actual time spent in transportation accounts for only 40% of the time from transfer acceptance to arrival of the patient at the receiving hospital, on average. Efforts to speed transfers should focus on shortening the time from transfer acceptance to departure from the referring hospital.
Introduction
The defining goal of trauma systems is to provide timely, definitive care to all injured patients, regardless of location. For many patients injured in rural areas, emergency physicians working in community hospitals without special expertise in trauma care initially assess and stabilize these patients and then possibly transfer them to a trauma center. Time is potentially of the essence during this period because experienced care is widely believed to limit morbidity and mortality.1–4
Several studies have focused on the length of time that elapses before emergency physicians at referring hospitals request a transfer.5–9 This time period, frequently called the “time-to-request,” is of interest because personnel at the referring hospital administer care unilaterally during this period. In theory, once the referring physician contacts a trauma center, personnel at the trauma center can help guide care and the interhospital transfer process proceeds in earnest. The implication in many previous studies is that the transfer process after transfer acceptance takes relatively little time.
The “time-to-request,” however, describes only a portion of the entire time from initial presentation of the patient to arrival at a trauma center. Few studies have evaluated timing details of the transfer process after the decision is made to transfer the patient, and each has quantified only a portion of the process5,6,10–13 or has described only the entire time spent at the referring hospital.9,14–16 To our knowledge, no study has yet focused on describing the duration of the interhospital transfer process and its component time intervals. To better understand the transfer process, we set out to: (1) determine the length of time the process of transferring acutely injured trauma patients takes, as well as the component time intervals of this process, and (2) explore factors that are associated with the length of time the transfer process takes. Although the notion of the “golden hour”–-that the likelihood of preventable mortality routinely increases if optimal care is not instituted within the first hour after traumatic injury–-may be more useful as a heuristic concept than a literal clinical phenomenon, 17 more precise knowledge of how long transfers take and how the time is spent might suggest ways to increase the efficiency of the process.
Methods
Study design
We conducted a descriptive, retrospective case series study of acutely injured patients who were transferred to a regional trauma center. The study design was reviewed and approved by the Institutional Review Boards at the participating institutions.
Study setting and population
We reviewed records of all trauma patients transferred within eight hours of initial evaluation from the emergency departments (EDs) of outlying hospitals to three regional trauma centers: the University of California, Davis, Medical Center (UCDMC), Sacramento, California (American College of Surgeons Level I trauma center); University Medical Center (UMC), Fresno, California (Level I); and Washoe Medical Center (WMC), Reno, Nevada (Level II). Each of these centers admits over 2000 trauma patients per year and serves a geographically large rural catchment area. We used trauma registries and logs of transferred patients to identify transferred trauma patients. We examined all cases from the time period July 1999 to June 2000 for UMC and WMC and from January 1999 to December 2000 for UCDMC. We used this time period because detailed time information was available from a prior analysis of the transfer process. Transfer processes between referring hospitals and these three centers have not changed substantially since this time period.
The process of accepting the transfer of acutely injured patients is slightly different at each of the three trauma centers studied. Arrangements for interhospital transportation are typically made only after acceptance of transfers to UCDMC and UMC. In contrast, physicians who refer patients to WMC frequently contact a transport service before requesting transfer to WMC. Both UCDMC and UMC use a centralized office or “transfer center” that coordinates interhospital transfers, whereas WMC does not. Trained nurses at these transfer centers facilitate communication between referring and accepting physicians, coordinate transfer arrangements, and maintain time records of the process. At WMC transfers are arranged directly between referring physicians and WMC emergency physicians, and the specific time of transfer acceptance is not routinely recorded.
Data collection
Trained abstractors recorded data using the same standard abstraction instrument at all three centers. We examined information from the patients’ medical record (including records submitted from the referring hospital, if available), the transfer center records, and the transport service records. We recorded demographic data, mechanism of injury, referring hospital identity, mode of transport, length of stay, discharge diagnoses, and disposition upon discharge. We tabulated the following times: (1) initial presentation at the ED of the referring hospital, (2) request for transfer, (3) acceptance of the transfer by a physician at the trauma center, (4) request for a transport service, (5) arrival of the transport service at the ED of the referring hospital, (6) departure of the transport service, and (7) arrival of the patient at the trauma center. From these times, we calculated specific time intervals, each of which was independently derived from the raw time data. We designated the time of the request for transfer as the beginning of the transfer process. In rare instances in which patients departed the referring hospital before a physician formally accepted the transfer, we defined the beginning of the transfer process as the earlier of either the request for transfer or the request of the transport service. We determined transportation distances using computerized geographic information systems (Yahoo! Maps Driving Directions® website for ambulance transport and flight navigation software for helicopter and airplane transport). We characterized anatomic injury severity using the Injury Severity Score (ISS).
We collected additional data for patients transferred to UCDMC to further characterize the transfer process and explore factors that might prolong the duration of the transfer process in this subgroup of patients. We recorded the time of initial dispatch of prehospital personnel (as a surrogate for the time of the injury incident) and whether the patient was hypotensive prior to transfer (systolic blood pressure <90 mm Hg for patients >5 years age, <80 mm Hg for patients 1–5 years, and <70 mm Hg for patients <1 year). Personnel from either referring hospitals or UCDMC may arrange transportation for transfers to UCDMC. We recorded which group contacted the transport service and compared the time from transfer acceptance to the request of a transport service depending on which group contacted the transport service. We recorded the time documented by the referring physician for transfer acceptance if it was available. We compared this with the time of transfer acceptance documented by the UCDMC transfer center to ensure that there were not systematic discrepancies in times recorded at the referring hospitals and UCDMC.
Data analysis
We used analysis of variance (ANOVA) to determine whether there was any association between the lengths of time intervals and the trauma center to which the patient was transferred. We used linear regression to determine whether observed relationships between time intervals of the transfer process and associated characteristics persisted after adjustment for potential confounding factors. Because ANOVA and linear regression techniques evaluating time as the outcome might violate the assumptions of normally distributed errors and appropriateness of the systematic fit of the models, we repeated these analyses using a generalized linear model (GLM) approach based on a gamma distribution and robust variance estimation. We evaluated the relationship between the duration of the transfer process (from transfer acceptance to arrival of the patient at the trauma center) and mortality using logistic regression. We categorized the predictor, the duration of the transfer process, as 0–60, 61–120, 121–180, or >180 minutes, and we considered age, gender, ISS, mechanism of injury, and mode of transport as possible confounding factors.
We report results as the mean ± standard deviation or, for highly skewed distributions, the median and interquartile range (IQR). Prior to analysis, we set α at 0.05. We used the Bonferroni correction to adjust for multiple testing among pairwise comparisons within ANOVA and linear and logistic regression results. Statistical analyses were performed with Stata 9.0 (Stata Corporation, College Station, Texas).
Results
Demographic and injury characteristics of transferred trauma patients.
UCDMC, University of California, Davis, Medical Center; UMC, University Medical Center; WMC, Washoe Medical Center; ISS, Injury Severity Score NA, Not available.
24-month period.
12-month period.
Four referring hospitals transferred patients to both UCDMC and WMC.
Mean ± standard deviation.
Median and interquartile range.

Geographic distribution of referring hospitals and receiving trauma centers for 1099 transferred acutely injured trauma patients.
Duration of the transfer process
Duration of the interhospital transfer process and its component time intervals.
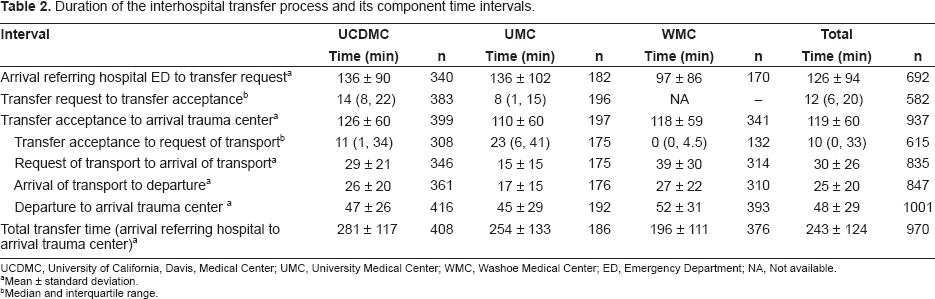
UCDMC, University of California, Davis, Medical Center; UMC, University Medical Center; WMC, Washoe Medical Center; ED, Emergency Department; NA, Not available.
Mean ± standard deviation.
Median and interquartile range.
The mean time from transfer acceptance until arrival at the trauma center was 119 ± 60 minutes. This time interval included 10 min (IQR 0, 33 min) from transfer acceptance to request of a transport vehicle, 30 ± 26 min from transport request to arrival of the transport personnel, 25 ± 20 min from transport arrival to departure of the patient from the referring hospital, and 48 ± 29 min for transportation of the patient to the trauma center. The average time from transfer acceptance to departure of the patient from the referring hospital was 68 ± 48 min. The time from transfer acceptance until arrival at the trauma center was only slightly different among the three centers with the only pairwise difference being between UCDMC and UMC [15 min faster (95% C.I. 5–26 min) for transfers to UMC].
Duration of the interhospital transfer process and its component time intervals, by mode of transport.

ED, Emergency Department.
Mean ± standard deviation.
Median and interquartile range.
ISS was not associated with the time from transfer acceptance until departure of the patient from the referring hospital (p = 0.48) (Fig. 2) or with the time from transfer acceptance until request of a transport service (p = 0.42). A penetrating mechanism of injury was associated with shorter time from transfer acceptance until departure of the patient from the referring hospital [15 min less (95% C.I. 4–26 min less)].
Relationship between the time from transfer acceptance to departure of the patient from the referring hospital and Injury Severity Score (n = 928). The solid line indicates the fitted relationship (from linear regression) and the shaded region indicates 95% confidence intervals. The dashed line indicates the smoothed relationship (based on running-line least-squares smoothing) using a bandwidth of 0.8.
Results for the above analyses were essentially unchanged with use of a GLM-based approach.
Duration of the transfer process and mortality
Increased duration of the transfer process did not have a clear association with mortality. Relative to transfers that took 0–60 min, transfers that took >180, 121–180, or 61–120 min were associated with a similar likelihood of death [OR 0.8 (95% C.I. 0.3–1.9), 1.4 (95% C.I. 0.6–3.3), and 0.8 (95% C.I. 0.3–2.5), respectively]. These relationships did not change substantially with adjustment for age, gender, ISS, mechanism of injury, and mode of transport [OR 0.8 (95% C.I. 0.2–2.9), 1.8 (95% C.I. 0.6–4.8), and 0.9 (95% C.I. 0.3–2.2), respectively].
UCDMC subgroup
Among 244 patients transferred to UCDMC for whom information was available on the time of initial dispatch of prehospital personnel, the median time from dispatch to arrival at the referring hospital was 46 min (IQR 30, 80 min). Out of 381 patients transferred to UCDMC who had records documenting at least two blood pressure measurements, 50 (13%) were hypotensive prior to transfer. The mean time from transfer acceptance to departure from the referring hospital was 17 min longer (95% C.I. 0.3–34 min) for patients with hypotension than those without.
The mean time from transfer acceptance until request of a transport service was 24 min longer (95% C.I. 16–33 min) when personnel at the referring hospital arranged transportation versus personnel at UCDMC.
The mean difference between the acceptance times documented by the UCDMC transfer center and the referring hospital records was +2.1 min (95% C.I. -0.6 to +4.9 min).
Discussion
The transfer process of acutely injured patients takes a substantial amount of time by itself even after patients are accepted for transfer. We found that the time from transfer acceptance until arrival of the patient at the trauma center took two hours on average. This was roughly the same amount of time as the interval from arrival of the patient at the emergency department of the referring hospital until transfer request. This finding was consistent across the three trauma centers, despite differences in geography, mode of transport, transport distance, and organization of the transfer process. Although one might intuitively anticipate that the duration of the transfer process would be largely dependent on the time it takes to physically transport the patient, our results suggest that transportation represents only about 40% of the time from acceptance of the transfer to arrival at the trauma center. The duration of the transfer process differed little if any on the basis of anatomic injury severity as reflected by ISS, or physiologic injury severity as reflected by whether the patient was hypotensive at the referring hospital.
The time from presentation at a referring hospital to arrival at a regional trauma center can be divided into the time before and after transfer acceptance. During the phase before a transfer is accepted, attention is typically focused on initial evaluation and stabilization of the patient. Sometimes the decision to transfer a patient necessarily depends on the results of imaging, but additional testing takes additional time, and tests to definitively diagnose suspected injuries for which no specialist is available only lead to delays. 16 The American College of Surgeons Committee on Trauma has also advocated criteria that should prompt consideration of transfer prior to extensive diagnostic evaluation. 18 Our data suggest that the time from transfer request to transfer acceptance represents only a small portion of the time from arrival at the referring hospital to transfer acceptance.
There are several possible explanations for the amount of time spent at referring hospitals after acceptance of the patient by the trauma center. Although the American College of Surgeons Advanced Trauma Life Support course emphasizes expeditious transfers, 19 a variety of factors may contribute to delays even once this process is underway: studies/procedures must be concluded; at least a minimal level of documentation should be completed, if possible; basic patient information should be transmitted to the receiving hospital; patient consent should be obtained (if applicable); transportation has to be arranged; and the patient should be prepared (e.g. lines and tubes secured, spine immobilized, and monitors in place) sufficiently to allow safe transport.
Analysis of the component time intervals of the transfer process suggests ways in which the transfer process might be better managed. Some transfers might be expedited specifically by earlier contact of the transport service. Whereas helicopter and airplane transport services were typically contacted with little delay, ground ambulance services were contacted a median of 23 min after transfer acceptance. Furthermore, among transfers to UCDMC, delegating the task of arranging transportation to referring hospital personnel was associated with a 24 min delay. Such delays suggest that personnel at trauma centers should specifically advise referring physicians to contact a transport service immediately after their telephone conversation; alternatively, personnel at trauma centers might even advocate that referring physicians start making transportation arrangements prior to contacting the trauma center. Also, recognition of the typical duration of the transfer process might help referring and accepting physicians alike assess the appropriateness of immediate transfer versus damage-control measures prior to transfer.
Previous studies of the transfer of trauma patients have frequently focused on the time from presentation at the referring hospital until transfer request.5–8 Information regarding the typical timing of events after transfer acceptance–-contact of a transport service, arrival of the transport service, departure of the patient, and arrival at the trauma center–-is less available.10,12 These previous studies were each limited to either one trauma center or the experience of a single transport service. In comparison, we analyzed transfers to three high-volume trauma centers, encompassing numerous ground ambulance, helicopter, and airplane services. The geographically contiguous catchment areas (see Fig. 1) of the three trauma centers we evaluated contain only a small number of other, more minor trauma centers, so we suspect that the results we observed are representative of all trauma patient transfers in this region for the study period.
This study has several limitations. First, documentation of times was incomplete and may have been inaccurate. Nonetheless, the transfer acceptance times recorded by personnel at the referring hospitals and UCDMC did not differ, suggesting a low likelihood of systematic errors in documentation by different parties. Second, because patients are transferred for a variety of reasons, not all patients may have needed urgent transfer. However, 13% of patients transferred to UCDMC had documented hypotension at the referring hospital. Also, the mortality rate of patients transferred to UCDMC was twice that of trauma patients who are admitted to UCDMC after presenting directly from the scene of injury. Third, expeditious transfer may not necessarily improve clinical outcomes, and hurried transfers might even conceivably worsen outcomes. We did not observe a relationship between the duration of the transfer process and mortality, perhaps in part because death was relatively uncommon in the cohort we evaluated. On the other hand, numerous studies support the notions that organized trauma care improves outcomes,1,2,20 that processes of care at referring hospitals inexperienced in trauma care could be improved,21–24 and that outcomes appear to be improved with transfer.3,4,25,26
The amount of time spent transferring acutely injured trauma patients to regional centers is comparable to the amount of time spent from presentation at the referring hospital to transfer request. Given that transportation involves an obligate amount of time, efforts to speed interfacility transfers should focus on shortening the time interval between transfer acceptance and departure of the patient from the referring hospital, and early contact of a transport service may be a simple means of doing so.
Footnotes
Acknowledgements
We thank Cindy Powers of Washoe Medical Center and Lynn Bennink of University Medical Center for assistance with reviewing records at those hospitals and Chris Ryther of American Medical Response, Clinical and Education Services Department, for contributing ambulance transport time data from AMR's Quality Improvement Clinical Network (QUICNET) database.
The authors report no conflicts of interest.