
Abstract
The majority of breast cancers express the estrogen receptor and depend on estradiol (E2) for their growth. Hormonal therapy aims at depriving estrogen signaling either by using selective estrogen receptor modulators (SERM)–-that interfere with the binding of E2 to its receptor (ER)–-or aromatase inhibitors (AI)–-that block the aromatase-dependent synthesis of E2. While SERMs are recommended for both pre- and post-menopausal patients, AIs are indicated only for post-menopausal patients. For the past 20 years, the SERM tamoxifen has been considered the “gold standard” for the treatment of hormone receptor positive breast cancers. However, tamoxifen's role is now challenged by third generation AIs, such as anastrozole, which exhibit greater efficacy in the adjuvant setting in several recently reported trials. This review will focus on anastrozole's mechanism of action, dosing, pharmacology, pharmacokinetics, and clinical applications. It will briefly discuss the clinical trials that determined anastrozole's efficacy in the treatment of advanced breast cancer (ABC) and in the neo-adjuvant setting. Finally, it will present the clinical trials that established anastrozole as a frontline agent in the treatment of post-menopausal women with hormone receptor positive early breast cancer.
Introduction–-Role of Estrogens and Aromatase in Breast Cancer
Estrogens are steroid hormones that play an important role in normal sexual development and function; they include: estrone (E1), 17-β estradiol or E2, and estriol (E3). Of these three hormones, E2 is the most abundant and biologically active. It is well accepted that E2 plays a role in the development of breast cancer; however, its precise mechanisms in mammary carcinogenesis remain unclear. Based on epidemiological and experimental data, it has been hypothesized that prolonged exposure to E2 could cause tumorigenesis via ER-dependent and -independent mechanisms. After binding with its nuclear receptor, E2 increases the proliferation rate of breast epithelia; by doing so, it reduces the time available for DNA repair potentially leading to an increased risk of mutation. 1 At the same time, E2 metabolites can be directly mutagenic; in fact, E2 can be converted to 4-hydroxyestradiol and subsequently to 3,4 estradiol quinone that binds covalently to guanine or adenine, resulting in depurination of DNA sequences leading to errors in DNA repair and point mutations.2,3 Finally, E2 can induce aneuploidy, which may also play a role in cancer etiology. 4
Estrogens are also involved in the progression of breast cancer. On the basis of the expression of ER, breast cancers are classified as hormone receptor positive or negative. 5 The majority of breast cancers (about 70%) fall into the hormone receptor positive category, and depend on the presence of E2 for their growth. In such cancers, E2 increases the transcription rate of protooncogenes such as Myc-1, c-fos, and c-jun resulting in increased breast cancer proliferation; 6 furthermore, it indirectly stimulates the production of breast epithelia growth factors, such as TGF-α and IGF. 7
Aromatase is an enzyme of the cytochrome p450 superfamily, which is involved in the synthesis of estrogens. Aromatase is the product of the CYP19 gene 8 and consists of two components: the hemoprotein aromatase cytochrome p450, and the flavoprotein NADPH-cytochrome p450 reductase. Localized in the endoplasmic reticulum of cells, aromatase catalyzes three hydroxylation reactions that convert androstenedione to E1, and testosterone to E2. E1 is subsequently converted to E2 by 17β-hydroxysteroid dehydrogenase (17β-HSD1), or to estrone sulfate (E1S) by estrone-sulfotransferases (E1-ST). E1S can then be converted back to E1 via estrone sulfatase (E1-STS) (Fig. 1). Because E1S binds to albumin, it represents the largest circulating reservoir of E2 precursor.
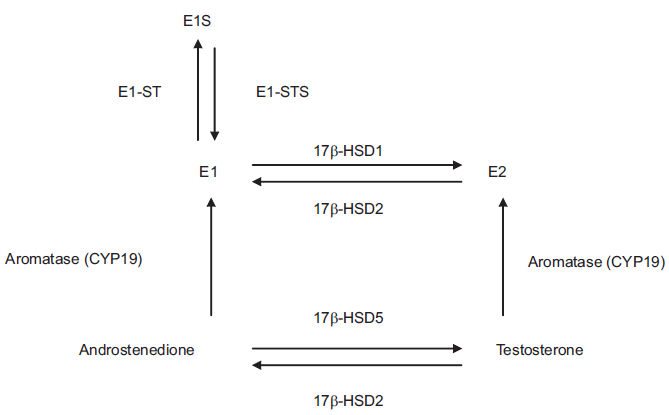
Role of aromatase in estrogen synthesis. Aromatase (CYP19) converts androstenedione to E1, and testosterone to E2. E1 is subsequently converted to E2 by 17β-hydroxysteroid dehydrogenase type 1 (17β-HSD1), while E2 can be converted back to E1 by 17β-HSD type 2 (17β-HSD2). E1 is converted to estrone sulfate (E1S) by estrone-sulfotransferases (E1-ST); E1S can then convert back to E1 via estrone sulfatase (E1-STS). Testosterone converts to androstenedione through the action of 17β-HSD2, while androstenedione converts to testosterone through 17β-HSD type 5 (17β-HSD5).
It is important to note that the site of production of E2 changes with age. In pre-menopausal women the ovaries represent the major source of aromatase and its substrate, androstenedione. Androstenedione is produced by the theca folliculi cells, and is converted to E1 and subsequently to E2 in the granulosa cells. Thus, during the reproductive years E2 mainly works as endocrine factor acting on estrogen sensitive tissues. In post-menopausal women the ovaries are still able to produce androstenedione, but they lose the expression of aromatase; at this stage, the adrenal glands become the major producer of androgens, which are then converted to estrogens in peripheral tissues such as liver, fat, muscle, 9 skin, bone, 10 and mammary tissue. 6 Thus, in postmenopausal women, E2 acts locally at these sites as paracrine or intracrine factor. 11 In post-menopausal patients the concentration of E2 in breast cancer specimens is 20-fold greater than in plasma, suggesting that intratumoral estrogen synthesis plays an important role in the progression of ER+ breast cancer 12 – although uptake and retention of E2 likely plays a role as well. The exact localization of aromatase in human breast tumors is still controversial; 13 nonetheless, the majority of breast cancer specimens exhibit aromatase activity and aromatase m-RNA levels higher than those observed in non-malignant mammary tissues, 14 supporting the hypothesis that in situ production of E2 plays a role in cancer progression. 15 A convincing proof of the relevance of in situ production of estrogens in post-menopausal breast cancer patients comes from animal studies. Yue et al used the ER+ cell line MCF-7 stably transfected with the human placental aromatase gene (MCF-7Ca) to xenograft ovariectomized nude mice. Mice were supplemented with subcutaneous injections of androstenedione to compensate for the low production of this hormone by their adrenal glands. In this model, the MCF-7Ca cell line provided an in situ source of estrogens that, in the absence of ovarian E2, was important for cancer growth; in fact, tumors derived from the MCF-7Ca cell line grew faster than those produced by the control MCF-7 cell line transfected with an empty plasmid vector.16,17
Given the importance of E2 in hormone receptor positive breast cancer, many therapeutic approaches have been aimed at depriving E2 signaling. The traditional method of E2 inhibition consists of interfering with E2 interaction with its receptors (ER α and β) using SERMs such as tamoxifen. For a long time, tamoxifen has been considered the treatment of choice for hormone receptor positive breast cancer. 18 Since the results of randomized phase III adjuvant clinical trials, such as NSABP B-14 19 and other trials performed in the 1970's and 1980's, tamoxifen has been extensively used in patients with early breast cancer as adjuvant therapy. Tamoxifen has also been a drug of choice in patients with hormone receptor positive metastatic disease, but nonetheless, only about 60% of these patients respond to the therapy, and almost all of them acquire tamoxifen resistance.20,21 Tamoxifen's biological activity is mediated by its major metabolite, endoxifen, that works both as ERα antagonist and partial agonist. 22 The agonist activity exhibited on the uterine ERα constitutes a major limitation for tamoxifen's clinical use: if on one hand tamoxifen inhibits the growth of breast cancer, on the other, it can induce endometrial hyperplasia and cancer.19,23,24 Because of its partial ERα agonist activity, tamoxifen also increases the incidence of thromboembolic events. 19 The drawbacks associated with the use of tamoxifen led to the development of alternative hormonal therapies.
Another approach to reduce E2 signaling utilizes AIs to decrease E2 synthesis. While SERMs are effective both in pre- and post-menopausal women, AIs are not indicated for pre-menopausal women, because in pre-menopausal women AIs, by lowering the E2 levels, stimulate the secretion of gonadotropins by the pituitary gland. The gonadotropins subsequently stimulate the ovaries to produce androgens counteracting AIs’ effect and possibly causing ovarian cysts. 25 In the late 1970s, the first AI, aminoglutethimide, was introduced into clinical practice. 26 Aminoglutethimide was efficient in the treatment of post-menopausal patients with advanced hormone receptor positive breast cancer, in a manner comparable to adrenalectomy or hypophysectomy.27,28 However, aminoglutethimide use was restricted by its high toxicity and low selectivity for the aromatase enzyme. 26 Since aminoglutethimide inhibits also the production of mineralocorticoids and corticosteroids, 29 it was given in combination with prednisone resulting in even more substantial side effects. Although aminoglutethimide had limitations, it opened a new area of research aimed at developing more potent, less toxic, and more specific AIs. The second-generation AIs fadrozole and formestane, developed in the 1980s, were less toxic than aminoglutethimide though their potency was unsatisfactory. Potent, specific and well-tolerated third-generation AIs were finally developed in the 1990s, and today are available for clinical use. Third generation AIs include letrozole (Femara), exemestane (Aromasin), and anastrozole (Arimidex). 30 The clinical trials that studied the efficacy of AIs showed their superiority to tamoxifen in the adjuvant setting, and their capacity of enhancing tamoxifen's effects in extended therapy.31–36
In the rest of this review we will focus on anastrozole, its pharmacology, pharmacokinetics, and clinical applications. To give a comprehensive view of the therapeutic efficacy of this drug and history of its development, we will briefly review the most significant trials that tested anastrozole as first- and second- line treatment of postmenopausal women with ABC, and as neoadjuvant treatment. Next, we will discuss in more details the trials that established anastrozole as a drug for adjuvant therapy of post-menopausal women with early breast cancer.
Mechanisms of Action of Anastrozole
AIs are classified as type I or type II depending on their nature and mechanism of action. Type I inhibitors are steroidal compounds (such as exemestane), while type II are nonsteroidal (such as letrozole and anastrozole). Both types of drugs inhibit aromatase interacting with the enzyme by mimicking androgens. Type I inhibitors form covalent bonds with the aromatase causing a permanent inhibition of the enzyme that can be restored only through synthesis of new aromatase. 30 In contrast, type II inhibitors, are competitive inhibitors. 30 An example is anastrozole (2,2-[5-(1H-1,2,4-triazol-1 ylmethyl)-1,3-phenylene]bis(2-methyl-propiononitrile)), a benzyltril triazole derivative that binds reversibly to the heme iron of the aromatase enzyme, thus inhibiting its activity (Fig. 2). Because of this reversible interaction with the enzyme, anastrozole must be constantly present to result in aromatase inhibition. 30
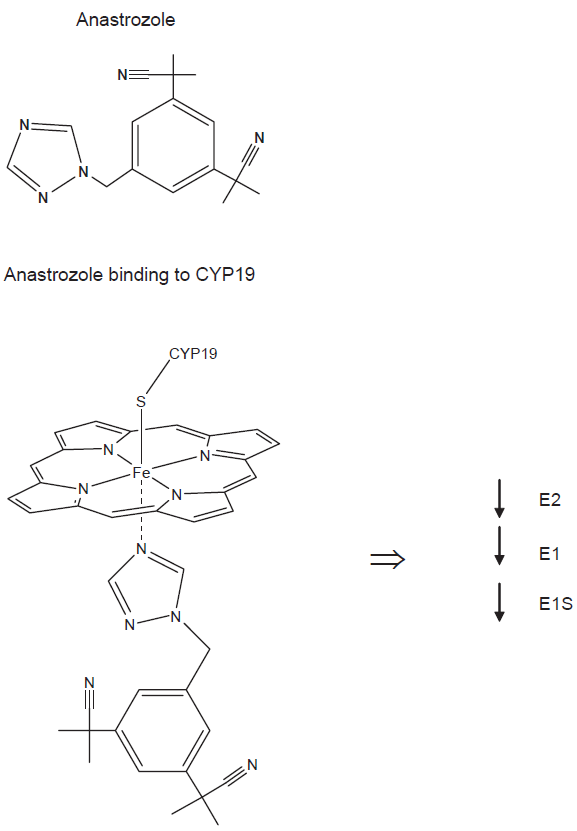
Anastrozole structure and mechanism of action. Anastrozole is a nonsteroidal AI that inhibits the aromatase enzyme by binding reversibly to its heme ion. By inhibiting the activity of aromatase, anastrozole reduces the levels of E2, E1, and E1S both in the periphery and in the mammary tissue.
Anastrozole Dosing
The in vivo potency of AIs has traditionally been determined by measuring the reduction of plasma or urinary levels of estrogens by a radioimmunoprecipitation assay (RIA). The isotopic kinetic technique has been adopted as more specific and sensitive method to measure the inhibition of aromatase turnover rates in vivo. 37 With this technique, the effects of AIs on estrogens production can be tested. Patients treated with AIs under steady state conditions are administered 3 H-androstenedione and 14 C-E1; subsequently, the levels of labeled E1 and E2 products in the plasma are measured. By using 14 C-E1 as internal standard, any possible loss that could occur during the purification steps can be corrected.
Several studies have been conducted to determine the rate of E2 synthesis and aromatase rate inhibition by AIs. In an early study, healthy post-menopausal women were randomized to receive 0.5 mg or 1 mg of anastrozole for 14 days; after three or four days both doses were able to reduce the levels of E2 to the limit of detection of RIA (3.7 pmol/L). 38 In another study, post-menopausal breast cancer patients originally treated with tamoxifen were randomized to receive either 1 or 10 mg of anastrozole daily for 28 days. Both doses resulted in a similar reduction of aromatization rate and plasma estrogens levels. 39 The results gathered in these and other early trials, in which different doses were given following a multiple-dose regimen, suggested that 1 mg of anastrozole per diem was the minimum dose able to consistently suppress E2 to the limit of detection of the RIA. 38
More recent studies were aimed at determining the effect of anastrozole in reducing the levels of intratumoral estrogens, and consequently, the intracrine activity of E2. In one trial, 12 postmenopausal women with locally ABC were treated with 1 mg of anastrozole for 15 weeks. 40 By comparing the level of estrogens in tumor tissues taken before the beginning and at the end of the treatment, it was shown that anastrozole was able to reduce the intratumoral levels of E2, E1, and E1S by 89, 83.4, and 72.9%, respectively. The plasma levels of E2, E1, and E1S were also reduced, specifically by 86.1, 83.9, and 94.2%. Another study involved post-menopausal women with locally advanced, operable, ER+ breast tumor treated with either 1 or 10 mg/day for 12 weeks. 41 Also under these conditions, anastrozole drastically reduced the peripheral and tumoral aromatase activity, and the intratumoral levels of E1 and E2.
Taken together, the results of these studies demonstrate that anastrozole is potent in reducing the aromatase activity and level of estrogens in the periphery and, more importantly, in the mammary tissue.
Anastrozole Selectivity
The activity of anastrozole is highly selective. Anastrozole has no effect on the synthesis of androgenic precursors; likewise, it does not alter the cortisol or aldosterone secretion at the baseline or after stimulation with adrenocorticotropic hormone.38,42 Finally, anastrozole does not affect the plasma concentration of the luteinizing hormone or follicle stimulating hormone in post-menopausal women, 43 or the thyroid stimulating hormone levels. 42
Anastrozole Pharmacokinetics
Within a dose range of 1-20 mg, the pharmacokinetic parameters of anastrozole remain linear. 38 Additionally, its pharmacokinetic parameters exhibit remarkably low inter- and intra-patients variability. 38 At the recommended daily dose of 1mg, anastrozole reaches the maximum plasma concentration (Cmax = 13.7 μg/L) two hours after oral administration. 43 Anastrozole is more rapidly absorbed when administered to women who have fasted; however, the extent of its absorption is not altered by food. 44 Daily doses of anastrozole ranging from 0.5 to 10 mg, administered to healthy post-menopausal women or patients, attained plasma steady-state concentrations after 9 to 10 days of treatment, and such concentrations were 3-fold higher than those observed after a single dose treatment.38,43 Anastrozole is mainly metabolized in the liver by reactions of N-dealkylation, glucuronidation, and hydroxylation that lead to a terminal halflife of about 50 hours. 45 Within 72 hours of dosing, less than 10% of anastrozole is excreted in the urine as unchanged drug, while 60% is excreted as metabolites. 46 Notably, none of anastrozole's three principal metabolites, namely triazole, hydroxyanastrozole, and anastrozole-glucoronide, exhibit anti-aromatase activity. 44 Although the liver accounts for 85% of the drug metabolism, anastrozole may be prescribed to patients with mild to moderate hepatic impairment and they exhibit plasma concentrations of anastrozole similar to those of patients with normal hepatic functions. 42 Since renal clearance is not an important pathway in the metabolism of this drug, anastrozole can be safely administered to patients with renal impairment and they show a normal systemic clearance of the drug. 46
Drug-drug Interaction
In vitro studies conducted using human liver microsomes demonstrated that anastrozole does not inhibit the activity of cytochrome p450 enzymes CYP2A6 and CYP2D6, while it inhibits the activity of CYP1A2, CYP3A4, and CYP2C9. However, the physiologically relevant concentrations reached during anastrozole treatment (0.3 μM) are about 30-fold lower than the Ki values observed in these in vitro studies (8-10 μM). Thus, anastrozole is not expected to interact with drugs metabolized by CYP enzymes in vivo. 47 The only significant drug interaction reported to date is with tamoxifen, which decreases the plasma levels of anastrozole up to 27% by unknown mechanisms. 48
Therapeutic Efficacy of Anastrozole
First- and second-line therapy in ABC
In post-menopausal ER+ ABC patients, anastrozole exhibited greater clinical efficacy compared to earlier hormonal therapies, such as megestrol acetate and tamoxifen. Two randomized, parallel-group, multicenter trials, performed in a population of post-menopausal ABC patients exhibiting progression after tamoxifen, compared the efficacy and tolerability of anastrozole (1 or 10 mg/day) versus megestrol acetate (40 mg/4 times daily). 49 In both studies, the median follow-up duration was 31 months. Anastrozole, at a dose of 1 mg/day, showed significant improvement in survival when compared to megestrol acetate, with a favorable tolerability profile. As result of these successful trials, anastrozole is now recommended for postmenopausal women with ABC whose disease had progressed after tamoxifen treatment.
Two subsequent studies suggested that anastrozole is as effective as tamoxifen when used as f irst-line therapy for ABC and exhibits a more favorable profile.31,50 One study was conducted in Canada and the United States (North America trial), while the other in Europe, Australia, New Zealand, South America, and South Africa (Tamoxifen or Arimidex Randomized Group Efficacy and Tolerability–-TARGET). These two studies had identical design: post-menopausal women with ER+ and/or PR+ or receptor-unknown ABS were randomized and treated with either tamoxifen (20 mg/day) or anastrozole (1 mg/day). Overall survival (OS), time to progression (TTP), and tolerability were evaluated as primary endpoints. A combined analysis of the North America and TARGET trials showed that at 43.7 months median follow up, tamoxifen and anastrozole exhibited comparable OS, but anastrozole exhibited increased TTP (10.7 months for anastrozole versus 6.4 months for tamoxifen p = 0.022) and a greater clinical benefit (complete response + partial response + stable disease) in patients with ER+/PR+ disease. 51 Notably, the North America study, in which more than 89% of the patients were ER+/PR+, exhibited TTP favoring anastrozole (11.1 months versus 5.6 months, p = 0.005). The TTP of the combined analysis of both studies was lower than the one observed for the North America study, possibly because only 45% patients in the TARGET study had hormone receptors positive disease. Patients treated with anastrozole had a lower incidence of undesired effects such as thromboembolic event or vaginal bleeding, and a slightly higher incidence of hot flashes and vaginal dryness compared to patients treated with tamoxifen. In light of the improved TTP and better tolerability observed in patients treated with anastrozole, anastrozole was approved by the FDA as first-line treatment of post-menopausal women with ABC in addition to the indication for disease progression after anti-estrogen therapy.
Neoadjuvant treatment
The efficacy of anastrozole has also been observed in the neo-adjuvant setting. In the Immediate Preoperative Anastrozole, Tamoxifen, or Combined with Tamoxifen Trial (IMPACT), 330 post-menopausal women with ER+ operable breast cancer or with locally-advanced disease were randomized and treated with either anastrozole (1 mg/day), tamoxifen (20 mg/day), or a combination of the two drugs for three months before the surgery. 52 This study further confirmed that anastrozole was well tolerated by the patients. The OS was similar for all the treatments, as was reduction in tumor size for all women in the trial. Nonetheless, anastrozole was superior to tamoxifen for reduction of tumor size in the group initially classified as having tumors large enough to require mastectomy. Overall, 44% of the patients that were classified as requiring a mastectomy at the baseline received breast-conserving surgery, versus 31% in the tamoxifen arm.
Similarly, the randomized, multicenter Pre-Operative “Arimidex” Compared to Tamoxifen (PROACT) trial compared the effect of neoadjuvant treatment with anastrozole or tamoxifen in 451 post-menopausal women with ER+ large operable, potentially operable, or inoperable breast cancer. 53 Patients were treated with anastrozole (1 mg/day) or tamoxifen (20 mg/day) for 12 weeks prior the surgery. While anastrozole and tamoxifen exhibited similar objective response rates, breast-conserving surgery was made possible in 43% of the patients receiving anastrozole compared to 30.8% of the patients receiving tamoxifen (p = 0.04).
A combined analysis of the IMPACT and PRO-ACT trials, which considered only patients who were given anastrozole or tamoxifen alone, confirmed the efficacy of anastrozole as neoadjuvant treatment that could potentially render previously inoperable tumors operable. 54
Semiglazov et al compared anastrozole and exemestane to chemotherapy (doxorubicin with paclitaxel) in the neo-adjuvant setting and found that AIs are equally efficacious for all the endpoints studied, including objective response, time to response, and fraction of patients achieving complete remission. 55 As expected, AIs were better tolerated with minimal adverse effects compared to the anthracycline and taxane chemotherapy. Thus, in the appropriate clinical setting of postmenopausal patients with ER+ bulky disease, anastrozole represents a good alternative to chemotherapy in the neo-adjuvant setting. 56
Adjuvant therapy in early breast cancer
Up-front therapy
To reduce the early risk of relapse that often occurs in breast cancer patients after surgery, 57 it is important to identify more effective adjuvant treatments. The Arimidex, Tamoxifen, Alone or in Combination (ATAC) is the most significant multicenter prospective double-blinded randomized clinical trial undertaken to compare the up-front use of anastrozole, tamoxifen, or a combination of the two drugs, in post-menopausal women with early localized operable breast cancer–-with an intention to treat analysis. Between the years 1996 to 2000, 9,366 patients from 21 countries were recruited to take part in the study. The whole population underwent surgery (plus or minus chemotherapy or radiotherapy) within 8 weeks prior the treatment, and was randomized into three groups: 3,125 women received anastrozole (1 mg/day) and tamoxifen placebo, 3,116 tamoxifen (20 mg/day) and anastrozole placebo, and 3,125 the combination tamoxifen (20 mg/day) and anastrozole (1 mg/day) (Fig. 3). Treatment was planned to continue for a total of five years. Patients with hormone receptor negative or unknown receptor status were included in the study, though the majority of the trial population (84%) had either ER or progesterone receptor (PR) positive tumors. An initial analysis of the trial, performed at 33 months of median follow-up, exhibited no differences between the groups that received the combination tamoxifen and anastrozole or tamoxifen alone. 48 These results demonstrated that although tamoxifen and anastrozole are endocrine agents with different mechanisms of action, they do not function in an additive or synergistic fashion. Thus, in consideration of the fact that the combination with anastrozole and tamoxifen did not have higher efficacy or tolerability benefits and was worse than anastrozole alone, this arm of the study was discontinued. Further analysis was conducted at 47 months of median follow-up, 48 after completion of the five years’ adjuvant treatment, 34 and at 100 months of median follow-up. 58 A future analysis is planned for the year 2010, when all the participants will be more than 10 years past the beginning of the treatment. Since the earliest time points, it appeared clear that anastrozole was more efficacious than tamoxifen in prolonging disease free survival (DFS; defined as the time to earliest local or distant recurrence, new primary breast cancer, or death from all causes), time to relapse (TTR), and in reducing the incidence of contralateral breast cancer (CLBC). The benefits associated with anastrozole treatment were confirmed, and remarkably maintained after the treatment was complete. At 100 months of median follow-up, DFS, TTR, and time to distant recurrence (TTDR) continued to improve, while CLBC was lower in the population treated with anastrozole. These effects were particularly pronounced in the ER+/PR– subpopulation, which represented 19% of the ER+ population. 58 On the other hand, the subgroups of patients exhibiting low ER, low PR, or high expression of HER2 exhibited a shorter TTR and did not appear to benefit from anastrozole. 59 Although the total number of deaths after recurrence was slightly decreased in the anastrozole group compared to the tamoxifen group, the difference was not statistically significant, giving similar OS. The safety profile described in the 100 months follow-up confirmed the data gathered at the previous time points. Many of the risks associated with tamoxifen therapy are due to its activity as a partial ER agonist. Tamoxifen has the advantage of protecting postmenopausal women from bone loss, but increases the risk of developing thromboembolic disorders or gynecologic complications such as hot flashes, vaginal bleeding and discharge or endometrial cancer. These major side-effects associated with tamoxifen were significantly lower in the patients treated with anastrozole. The major disadvantage of anastrozole therapy lies in the increased incidence of fracture episodes, especially of the spine. 48 Interestingly, the increase in the number of yearly fractures was observed only during the actual anastrozole treatment, whereas in the post-treatment follow-up period there were no significant differences between the anastrozole and tamoxifen treatment groups. 58 As a consequence of estrogen deprivation, anastrozole treated patients experienced a 6-7% bone loss during the five years treatment; however this loss did not result in osteoporosis, at least in those patients with normal bone density at the beginning of the treatment. 58 Arthralgia is an additional adverse effect more common in patients treated with anastrozole than in patients treated with tamoxifen (35.6% versus 29.4%, p < 0.0001). 34 Overall, very few patients withdrew from the study as a consequence of severe joint symptoms (2.1% versus 0.9% of the tamoxifen group). 60 The exact mechanism of anastrozole-related arthralgia is not known, but it might be due to E2 deprivation. 61
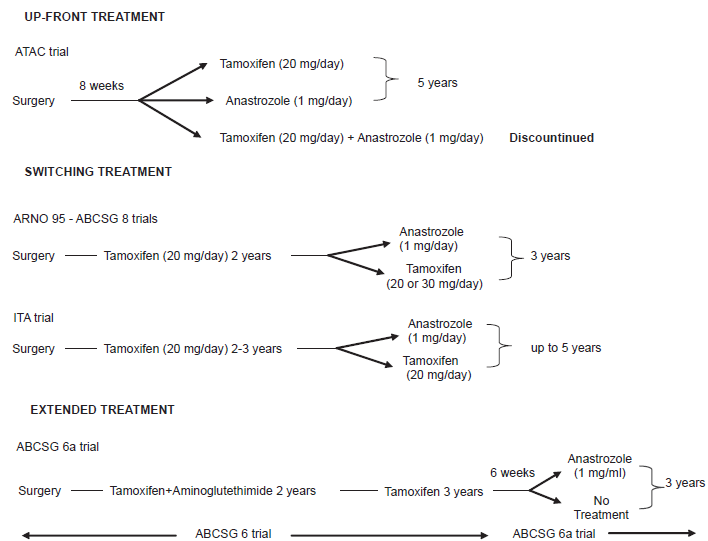
Design of the ATAC, ARNO 95, ABCSG 8, ITA, and ABCSG 6a trials. ATAC trial evaluated the use of anastrozole versus tamoxifen in up-front therapy of post-menopausal women with early breast cancer. ARNO 95, ABCSG 8, and ITA trials studied the benefits of switching to anastrozole after 2 or 3 years of tamoxifen therapy. ABCSG 6a trial examined the advantages of supplementing 5 years of tamoxifen based adjuvant therapy with an additional 3 years of anastrozole therapy.
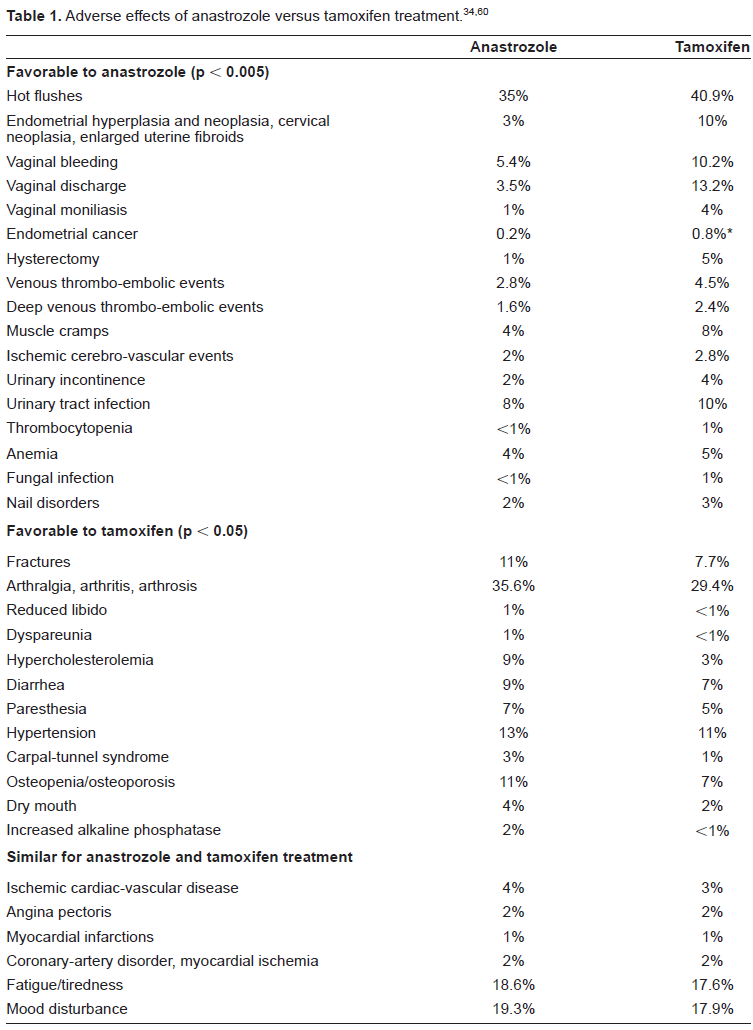
Table 1 offers a more detailed description of adverse effect related to anastrozole versus tamoxifen treatment. As a general rule, both anastrozole and tamoxifen were well tolerated but the anastrozole arm exhibited fewer treatment withdrawals due to adverse effects. 60
Switching therapy
The ATAC trial showed that anastrozole offers efficacy and tolerability benefits when used as primary adjuvant therapy. However, it did not answer the following question: Would it be beneficial for post-menopausal women with hormone receptor positive early breast cancer to start their adjuvant therapy with tamoxifen and subsequently switch to anastrozole? The Arimidex-Nolvadex 95 (ARNO 95), 62 Italian Tamoxifen Anastrozole (ITA),63,64 and Austrian Breast and Colorectal Cancer Study Group 8 (ABCSG 8)35,65 trials attempted to tackle this issue (Fig. 3). Results obtained for the 2,262 patients included in the ABCSG 8 trial have been analyzed in conjunction with the ITA and/or ARNO 95 data,35,65 while the ITA and ARNO 95 data have also been analyzed independently (see below).
In the ARNO 95 trial, 979 patients that underwent 2 years of adjuvant therapy with tamoxifen were randomized to switch to anastrozole (1 mg/day) or continue with tamoxifen (20 or 30 mg/day) for the following 3 years. In this study the primary endpoint was DFS, which included local or distant recurrence, CLBC, or death; secondary endpoints were OS and assessment of safety. The results revealed that switching to anastrozole results in greater benefit in terms of lower risk of recurrence, increased OS, and lower incidence of adverse events. 62 The combined analysis of ABCSG 8 and ARNO 95 trials, illustrated that at 28 months median follow-up the risk of developing local or distal metastasis, or CLBC was reduced by 40% in the group of patients that switched to anastrozole (hazard ratio 0.6, 95% CI 0.44-0.81, p = 0.0009). Both therapeutic regimens were well tolerated; however, patients treated with anastrozole had more fractures but fewer thromboses events than those treated with tamoxifen. 35
In the ITA trial, 448 patients who underwent two or three years of tamoxifen treatment were randomized to receive either anastrozole (1 mg/day) or tamoxifen (20 mg/day) for up to a total duration of f ive years. In this study, DFS, recurrence free survival (including local and distant recurrences but not CLBC) were primary endpoints, while OS was a secondary endpoint. At 36 months 63 and 52 months median follow-up, 64 the patients in the anastrozole group exhibited an increased event-free, disease-free, and local recurrence-free survival. In this trial there were more adverse effects in the anastrozole group, though they were less severe than those observed for the tamoxifen group.
A meta-analysis of the data gathered in the three trials confirmed that patients who switched to anastrozole exhibited a significant improvement of DFS, event free survival, distant recurrence free survival, and OS than those that continued with tamoxifen. 65
Extended therapy
The ABCSG 6a trial sought to investigate whether 5 years of tamoxifen based adjuvant therapy could be improved by 3 additional years of anastrozole (Fig. 3). 66 This study was prompted by the consideration that many women relapse after 5 years of tamoxifen, and by the results of the MA.17 trial carried out by the National Cancer Institute of Canada. The MA. 17 trial showed that the recurrence ratio of breast cancer was reduced by 42% in patients treated with prolonged adjuvant therapy consisting of 5 years of tamoxifen followed by 5 years of the nonsteroidal AI letrozole. 67 Patients enrolled in the ABCSG 6a trial were chosen from the participants of the ABCSG 6 trial who had not exhibited recurrence by the end of the study. In that original trial, post-menopausal women with hormone receptor positive early breast cancer were treated with a combination of tamoxifen and aminoglutethimide for 2 years followed by tamoxifen alone for 3 years, or with tamoxifen alone for 5 years. The treatment of the ABCSG 6a trial started within 6 weeks after completion of the 5 years of adjuvant therapy; patients were randomized to receive anastrozole (1 mg/day) or no treatment for 3 years. The primary endpoint of the study was recurrence free survival (time to the first evidence of local recurrence, distant metastasis, or CLBC), whereas OS was the secondary endpoint. At 62.3 months median follow-up, patients who received anastrozole exhibited significantly fewer recurrences than the patients belonging to the arm that did not receive any further treatment (7.15 versus 11.8%, which is equal to a relative reduction of 38%). Notably, the difference between the two groups was especially evident in terms of distant recurrence (4.1% versus 7.5%). No significant differences were observed in the OS of the two groups. Anastrozole was well tolerated, and interestingly the number of fracture events was lower than expected.
Overall the results of the ABCSG 6a study showed the possible benefits of extending adjuvant therapy beyond the commonly recommended 5 years. Treating patients with tamoxifen for more than 5 years does not result in a superior survival; 19 this is due to the adverse events associated with tamoxifen therapy, such as thromboembolic disease and endometrial cancer. Anastrozole, thanks to its less severe and more manageable adverse effects, suggests a promising option for a longer and more effective adjuvant therapy, although this remained to be confirmed in clinical trials.
Is Up-Front Treatment Preferable to Switching or Extended Treatment?
The data collected from the ARNO 95, ITA, and ABCSG 8 trials is informative and support the benefit of switching from tamoxifen to anastrozole in the adjuvant setting. However, those trials do not yet offer long-term follow-up analysis like the ATAC trial. At this point it is difficult to evaluate whether up-front therapy with anastrozole would be more beneficial than switching from tamoxifen to anastrozole. At the same time it is also difficult to evaluate at what point in time it would be optimal to transition from one drug to the other. In the absence of experimental evidences, these issues have been addressed with the aid of computer models.
Punglia et al developed Markov models to simulate 10 years DFS among patients treated with 5 years of tamoxifen, 5 years of AI, or sequential treatment that consisted in switching to AI after 2.5 or 5 years of tamoxifen.68,69 These models were based on the assumption that all commercially available AIs would have similar efficacy and tolerability, and were based on data available from clinical trials including the ATAC and ARNO trials. The first model estimated that the best adjuvant therapy consisted in switching to AI after 2.5 years of tamoxifen. With that regimen, the absolute DFS rates at 10 years were 83.7% and 67.6% for node negative and node positive patients, respectively, while up-front therapy with anastrozole yielded rates of 82.6% and 65.5% for node negative and node positive patients, respectively. According to this model, switching to AI after 5 years of tamoxifen did not further improve the DSF rates at 10 years. 68
An update of this first model showed that different subpopulations of patients might benefit from different therapeutic regimens. Specifically, the sequential treatment would be more beneficial for patients with ER+/PR+ breast cancer, whereas up-front treatment with AI would yield superior outcome in patients with ER+/PR– breast cancer. 69
Another computer model, proposed by Hilsenbeck and Osborne, predicted that the benefits of adopting up-front anastrozole therapy in patients with ER+/PR– breast cancer would not be obtained starting the therapy with tamoxifen and switching to anastrozole. On the other hand, switching to anastrozole after 3 or 5 years of tamoxifen may result in superior long-term benefit in patients with ER+/PR+ cancer. 70
Pharmacogenomics–-Moving towards a Personalized Therapy
Notwithstanding the benefit of AI therapy in postmenopausal women with hormone receptor positive disease, there is still high inter-patient variability in terms of response and tolerability to the AIs. 71 The different outcomes observed in patients treated with AIs might be due to genetic diversity. Similarly to polymorphisms of the CYP2D6 gene that influence response to tamoxifen, polymorphisms of the CYP19 gene, or other CYPs involved in AI metabolism (such as CYP2A6 and CYP2C19 for letrozole, and CYP3A4 for examestane), might affect response to AIs. 72
A relatively recent study re-sequenced the human CYP19 gene and identified 88 polymorphisms that resulted in 44 haplotypes in 60 patients from 4 ethnic groups (Caucasian Americans, Mexican American, African Americans, Han Chinese Americans). 73 Functional studies were conducted with 4 nonsynonymous coding single nucleotide polymorphisms (SNP) that alter the following amino acids: Trp 39 to Arg, 39 Thr201 to Met201, Arg264 to Cyst264, and Met364, to Thr.364 The Arg 39 Cys264 double variant allozyme, when transiently expressed in COS-1 cells, exhibits decreased levels of immunoreactive protein and lower enzymatic activity when compared to wild type (WT) enzyme. Interestingly, this allozyme showed a significant increase of Ki for letrozole when compared to the WT enzyme; such an increase could correlate with higher resistance to AIs. Also the Cys264 and Thr364 allozymes exhibited lower levels of immunoreactive protein and enzymatic activity compares to the WT enzyme, whereas the Arg 39 allozyme showed only a decrease in protein level. Of note, the Cys264 variant was expressed more frequently in Han Chinese Americans and African Americans, and the Arg 39 more in the Han Chinese Americans, suggesting that some ethnic groups might benefit more from AIs treatment than others. 73
In a subsequent study of letrozole, the role of three SNPs–-specifically, rs10046 and rs4646 located in the 3’ untranslated region, and rs727479 located in the intron 2 of CYP19–-was evaluated in the clinical response. 74 Towards that goal, 67 postmenopausal women with hormone receptor positive metastatic breast cancer were treated with letrozole (2.5 mg/day); the median follow-up of the study was 19.7 months and TTP was the primary end-point. Women with the rs4646 variant, who represented 46% of the total population under study, exhibited a significantly longer TTP when compared to women expressing the WT enzyme. Although these data suggest that letrozole treatment might be particularly efficacious in patients with the rs4646 variant, it remains to be determined if this variant is actually a prognostic factor in advanced breast cancer rather than a predictive factor for letrozole efficacy. Moreover, additional studies need to be done in order to determine the mechanisms by which the rs4646 variant inf luences letrozole activity.
There are no data available that link anastrozole efficacy to a particular gene polymorphism, as of yet, but studies on this matter are ongoing. The Pharmacogenetics Research Network (PRN) of the Mayo Clinic, the M.D. Anderson Cancer Center, and the Indiana University are evaluating whether variation in anastrozole pharmacokinetic and estrogen pharmacodinamic pathways might affect an individual patient's response to anastrostrole and the level of drug toxicity. 71
Effects of AIs Treatment on Patients’ Quality of Life
Results from the ATAC trial
The health-related quality of life (HRQoL) was evaluated in a sub-group of 1,105 women enrolled in the ATAC trial, after 2 years of treatment 75 and at the end of the 5 years’ adjuvant therapy. 76 Patients were asked to complete the Functional Assessment of Cancer Therapy-Breast (FACT-B) questionnaire including the endocrine subscale (ES) at baseline, after 3 months, and periodically every 6 months afterwards. The primary endpoint of the study was to evaluate the overall HRQoL in the tamoxifen and anastrozole group by assessing the sum of the physical well-being, functional well-being, and breast cancer subscale of the FACT-B questionnaire (FACT-B Trial Outcome Index or TOI). The secondary endpoints included comparison of the FACT-B subscales regarding emotional well-being (EWB) and social well-being (SWB), and evaluations of specific endocrine symptoms using the aforementioned ES. The results obtained after 2 years were consistent with those gathered at 5 years. The TOI improved from baseline to 2 years, and even more to 5 years, and was comparable in both treatment groups. 76 Also the EWB and SWB and ES scores were similar in the tamoxifen and anastrozole group. Interestingly, the ES scores after a decline observed in the first 3 months of treatment, became stable although it never recovered the baseline levels. Among the ES items, the tamoxifen group presented more cold sweats (9.1% versus 7.7%), night sweats (21.3% versus 17.8%), and dizziness (5.4% versus 3.1%), whereas diarrhea was more frequent in the anastrozole groups (3.1% versus 1.3%). Concerning gynecological symptoms and sexual function, patients treated with tamoxifen were more affected by vaginal discharge (5.2% versus 1.2%), while those treated with anastrozole frequently presented more vaginal dryness (18.5% versus 9.1%), pain or discomfort with intercourse (17.3% versus 8.1%), and reduced libido (34% versus 26.1%). 76
Taken together these results show that tamoxifen and anastrozole treatment have a similar influence on HRQoL over a period of 5 years.
AIs can improve the quality of life of tamoxifen-intolerant patients
The results of the study that evaluated the quality of life in the ATAC trial was limited by the fact that women on both arms of the trial tolerated well the treatments and did not exhibit menopausal symp-toms. 76 A recent study investigated whether AIs could be a reasonable alternative for women intolerant to tamoxifen who exhibit severe hot flashes and compromised quality of life–-conditions that are extremely relevant in the daily clinical practice. 77 In this study, 184 women intolerant to tamoxifen were switched to an AI (either letrozole or exemestane) and after 6 weeks they were given the possibility to switch back to tamoxifen. At 6 weeks, the hot flash score was significantly improved in the patients treated with AIs compared to those that continued with tamoxifen. Moreover, patients treated with AIs had higher mean of mood rating scale (MRS) score, and FACT-B with endocrine symptoms score. Thus, at 6 weeks 72% of the women in the study decided to continue with the AI therapy. At three months, women treated with AIs exhibited a higher severe arthragia rate than women treated with tamoxifen; however, the majority of them (58%) still preferred to be treated with AIs. Overall these results not only indicate that AIs can be preferable to women who suffer tamoxifen-induced menopausal symptoms, but they also suggest to clinicians that patients should be given the opportunity to decide which side effects are better tolerated and better fit with their life style.
Conclusions–-An Adjuvant Role for Anastrozole
The studies described in this review have highlighted the superiority of anastrozole to tamoxifen in up-front adjuvant therapy, 58 and the benefit of switching or extending to anastrozole after 2 to 5 years of tamoxifen in post-menopausal women with early breast cancer (Table 2).35,64,66 As a consequence of such convincing results, the guidelines of the national Comprehensive Cancer Network, the European Society of Medical Oncology, 78 the American Society of Clinical Oncology, 79 and the St. Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer, 80 now recommend anastrozole or other AIs for the adjuvant therapy of postmenopausal women with hormone receptor positive early breast cancer.
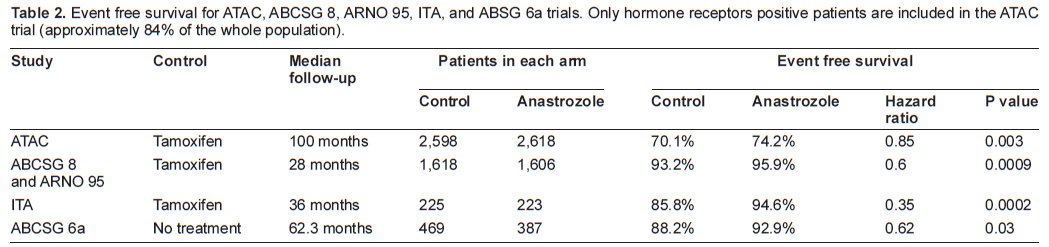
Event free survival for ATAC, ABCSG 8, ARNO 95, ITA, and ABSG 6a trials. Only hormone receptors positive patients are included in the ATAC trial (approximately 84% of the whole population).
The benefits associated with the use of anastrozole outweigh the adverse effects, which are more manageable than the toxicity associated with tamoxifen. Anastrozole treatment is mainly associated with osteoporosis and fracture events; consequently, women should have a baseline bone mineral density evaluation before starting the therapy, and possibly should be given treatments that prevent the bone loss – such as intravenous biphosphonate, oral biphosphonate clodronate, or risedronate. 79 Arthralgia (and/or joint stiffness) is another common adverse effect of anastrozole that has become of increasing importance because responsible for non-adherence and treatment withdrawal in 4 to 35% of women treated with an AI. 81 Symptoms have been reported in up to 40% of patients taking AIs, and often become apparent within the first two weeks of initiating an AI. Physicians should educate patients on the risk of developing arthralgia and on the current available treatments to reduce the pain. Recently, the Arthralgia Working Group designed an algorithm for the treatment of early breast cancer patients affected by AI-induced arthralgia that recommends the use of a variety of anti-inflammatory agents and analgesics for pain management. 82 Before starting anastrozole treatment, patients should be evaluated for a history of arthralgia or abnormalities of the synovia to determine if joint symptoms are new, or simply an aggravation of a pre-existing condition. Among non-traditional medicine approaches, acupuncture seems to alleviate the musculoskeletal pain in AIs treated patients, and may be adopted as supportive care to improve their quality of life. 83 Alternative treatments, such as tamoxifen, should be offered to patients with extremely severe symptoms or pre-existing arthralgia.
Though the use of anastrozole is well established, there are still several unresolved issues that prevent us from designing an optimal endocrine therapy for post-menopausal women with early disease. For instance, we still do not know if anastrozole is superior to other steroidal or nonsteroidal AIs. The results of numerous trials support the efficacy of exemestane, a steroidal third generation AI, in the treatment of patients previously treated with other second or third generation AIs, including anastrozole, or tamoxifen.84–90 Furthermore, another trial demonstrated the efficacy of formestane, a steroidal AI, after failure of anastrozole and letrozole treatment. 91 However, all these studies were conducted in postmenopausal women with advanced metastatic disease and are not applicable to patients with early disease. Only recently, a trial was set up with the purpose of comparing the effect of anastrozole and exemestane in the adjuvant treatment of postmenopausal women with early breast cancer (U.S. National Institute of Health; trial #NCT00248170). As yet, the results of such trial are not available.
Another important question that needs to be addressed is regarding the optimal moment of transition from tamoxifen to anastrozole, and the ideal duration of anastrozole treatment. Currently, there is no direct comparison between the benefits of the use of anastrozole up-front or after 2-3 years of tamoxifen, neither are there any data in support of a possible extended anastrozole adjuvant therapy (>5 years).
Disclosure of Potential Conflicts of Interest
The authors declare no conflict of interest and no affiliation with any drug companies, have not received any grant, honoraria, nor bear any stock.